All published articles of this journal are available on ScienceDirect.

Spinal Surgery in Patients with Parkinson’s Disease: Unsatisfactory Results, Failure and Disappointment
Authors Info & Affiliations
Abstract
Previous studies on spinal surgery in PD patients report an exceptionally high rate of complications. Failure and re -operation are frequent outcomes. This is a retrospective case series with the aim of establishing the rate of complications in patients with concomitant Parkinson’s disease.
Ten patients were subjected to spinal surgery from 2005 to 2009. The indications and type of operation varied. Cases of Failed Back Surgery and re-operation were sought. Follow – up was between 6 – 42 months. All 10 patients presented some clinical or radiological complication. The most common complications were screw pull – out and progressive spinal deformity. Re – operations were performed in 5 patients, while clinical and radiological results were poor in the majority of cases. Patients with Parkinson’s disease have a very high complication rate and often have to undergo revision surgery. This particular group of patients should be informed of the increased risk of failure and be closely followed – up on a regular basis.
INTRODUCTION
Parkinson’s disease (PD) is a degenerative disorder of the central nervous system, affecting the substantia nigra in the midbrain. Its prevalence increases exponentially with age, being estimated at 1.5% of the population over 60 years in Europe [1]. Recent advances in the treatment of Parkinson’s disease have improved the life expectancy and quality of life of patients. It nonetheless remains a debilitating disease, with those affected becoming increasingly incapable to perform their daily activities. PD patients are also affected by spinal disorders, and as the population ages, are expected to represent an increasingly substantial proportion of patients requiring spinal surgery.
The typical parkinsonian posture is flexion of the trunk, hip and knees, thus shifting the center of gravity and subjecting the patients’ spine to abnormal loads. In fact, the stooped posture that is so characteristic of the disease as to have been described by James Parkinson himself in 1817 [2] probably predisposes to an increased rate of spinal degeneration, although this remains to be confirmed. Nonetheless, degenerative conditions and particularly degenerative scoliosis have been found to be more frequent in PD patients than their age- matched counterparts [2, 3]. Furthermore, PD is also associated with an array of postural deformities besides the typical abnormal posture such as camptocormia (marked forward flexion of the thoracolumbar spine), Pisa syndrome (lateral flexion and axial rotation of the trunk), anterocollis (dropped head syndrome) and degenerative scoliosis [2, 4].
The purpose of the present case series is to assess the number and type of complications of spine surgery in PD patients and determine whether the presence of PD predisposes patients to a higher rate of such complications.
METHODS
A multicenter retrospective review study was performed. Patients were identified by consulting with the treating physicians and searching their institutions’ archives. The patients’ records from multiple centers were retrieved, identifying those where PD was diagnosed prior to undergoing spine surgery. Patients’ charts, imaging studies and surgery reports were reviewed. Comorbidities other than PD were recorded. All the cases were reviewed by a single, independent observer, not associated with the treatment or follow-up of any of the patients (MP). Implant position, sagittal balance, fusion state and instances of progressive deformity, implant failure or revision surgery were noted.
Overall, ten patients with confirmed PD were identified retrospectively. The indications and type of surgery were varied. Follow up was between 12- 36 months.
RESULTS
The group consisted of 7 women and 3 men. The average age at the time of surgery was 69.6 years. The patients’ diagnosis included kyphosis due to vertebral fracture in 5 patients, lumbar degenerative scoliosis in 3 patients (with concomitant stenosis in one patient) and lumbar stenosis in 2 patients. The thoracic spine was involved in one patient, the thoraco- lumbar in 5 patients and the lumbar spine in 4 patients. Six patients had some medical disorder besides PD. These included 3 patients with hypertension, 2 patients with hypothyroidism and one patient with chronic atrial fibrillation and hypertension. Follow up was between 12- 36 months, with 2 patients being lost after the 12-month follow up examination.
Since this cohort of patients was treated in various institutions, different clinical assessment tools were used for evaluation. This unfortunately made pooling of data and direct comparison unfeasible. Nonetheless, in the initial follow - up period, nine out of ten patients showed improve-ment of symptoms and clinical parameters. One patient with kyphosis and compression fracture of T12 treated with kyphoplasty and T9 - L3 fusion had persistent low back pain. Spinal radiographs were found to be normal at the first follow – up visit, but screw pull- out at L2 and L3 was seen at the second visit 2 months postoperatively. All other patients continued to improve until the 6 month follow- up. At one year, 6 patients (60%) showed lasting improvement, while 3 patients (30%) had a deterioration of their clinical parameters. By 2 years, all patients had experienced a worsening of their symptoms, a decline in their physical abilities scores and varying degrees of progressive kyphosis.
Ultimately, all 10 patients developed some form of surgery- related complication. 5 of the 10 patients had to undergo additional surgery (Figs. 1, 2). Of these, three patients were complicated by hardware failure and had revision surgery, with one developing adjacent segment disease (ASD) in addition to screw pullout. One patient developed ASD without associated hardware failure and also underwent revision surgery. Lastly, one patient sustained fractures in two vertebrae, one distant to and one at the proximal end of the fusion. That same patient sustained two further vertebral fractures one year after being treated with kyphoplasty. Of the 5 patients that were not re – operated, 2 developed severe camptocormia despite solid fusion, one developed flat – back deformity and was lost to follow-up and one developed proximal junctional kyphosis but declined further surgery. Overall, hardware failure in the form of screw pull – out occurred in 30% of patients, adjacent segment disease in 30% and vertebral fractures in 10% (one patient). There was loss of sagittal balance in 100% of patients, even in the presence of a solid fusion. Revision surgery was performed in 50% of the patients, as a result of hardware failure in 30%, worsening kyphosis in 10% and vertebral fracture in 10%.
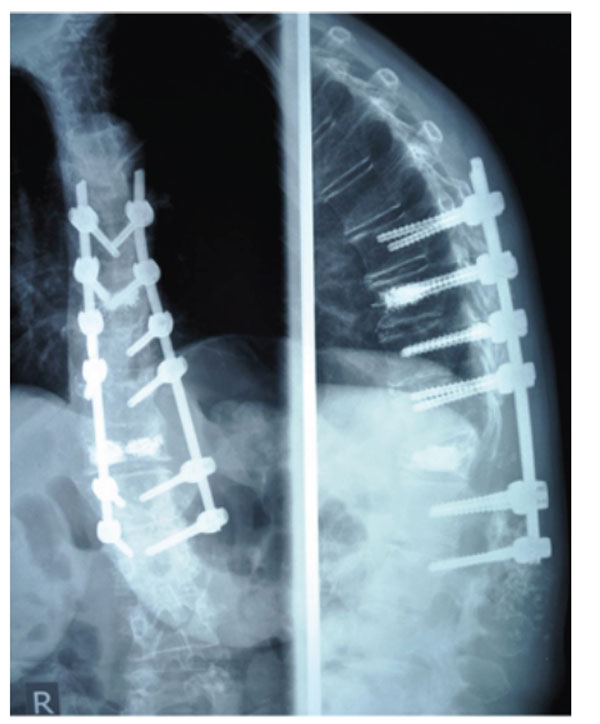
Lateral spinal radiograph of a patient (No 3 in Table 1) having underwent kyphoplasty and fusion for kyphosis and vertebral compression fracture 2 months postoperatively. Notice pull - out of lower screws.

Same patient as Fig. (1) after revision surgery. Notice extension of fusion into L4.
The patients’ characteristics, diagnoses and procedures are summarized in Table 1.
Patients diagnoses, surgeries and complications.
| Patient | Age | Diagnosis at First Presentation | Index Surgery | Time to Complication Development | Type of Complication | Time to Revision Surgery | Revision Surgery | Remarks |
|---|---|---|---|---|---|---|---|---|
| 1 | 71 | VCF T5, T9, L5 | Kyphoplasty | 16 months | Marked kyphosis T7- T8 | 18 months | Fusion T2 –T7 | |
| 2 | 74 | Lumbar scoliosis | Fusion | 14 months | ASD, Pre- junctional Kyphosis | Declined further surgery | ||
| 3 | 52 | Kyphosis, VCF T12 | Kyphoplasty, fusion T9 –L3 | 2 months | Pull out L2, L3 | 3 months | Fusion T9- L4 | |
| 4 | 68 | Kyphosis, VCF T12 | Fusion T9 – L5 | 2 years | Camptocormia | No hardware failure | ||
| 5 | 65 | Kyphosis, VCF L1 | Fusion T7 –L5 | 18 months | Camptocormia | No hardware failure | ||
| 6 | 72 | Lumbar stenosis | Laminectomy L3-L5, fusion L2-L5 | 18 months | Pull-out L2, ASD L1-L2 | 20 months | Fusion T12 – L5 | Stooped posture remains |
| 7 | 70 | Lumbar scoliosis | Fusion T12 – L5 | 12 months | VCF T6, T12 | 12 months | Kyphoplasty | VCF T7, T9 2 years post op |
| 8 | 77 | Lumbar stenosis and scoliosis | Laminectomy L3 –L5, fusion L3-L5, interspinous implant L2-L3 | 24 months | Flat back | Flexion contracture hips and knees | ||
| 9 | 68 | Disc herniation L3-L4, L4-L5 | Laminectomy L4 - L5, interspinous implant L3- L4 | 24 months | Sciatica, ASD L2-L3. | 24 months | Laminectomy L2-L3, Fusion L2-L5, interspinous implant L1-L2 | Stooped posture 3 years post op |
| 10 | 79 | Kyphosis, VCF L1 | Spinal Fusion T9-L3, Transpedicular Vertebrectomy L1-Harms cage | 27 months | Pull-out L2, L3 screws | Fused in Stooped posture |
ASD = adjacent segment disease VCF = vertebral compression fracture.
DISCUSSION
Previous studies on spinal surgery in PD patients are sparse and of retrospective design; they all have in common an exceptionally high rate of complications. Babat et al. [5] studied 14 patients with varying diagnoses, 12 of which (86%) required additional surgery. Nakashima et al. [6] report on 3 patients with vertebral body collapse that underwent circumferential fusion. All 3 had a marked progression of kyphosis, however no further operations were performed. Peek et al. [7] published a case report of a patient treated for PD- associated camptocormia. Due to recurring hardware failures, he required multiple re- operations, lengthy hospitalizations and prolonged immobilization in orthoses and hip spicas. Upadhyaya et al. [4] mention two PD patients that underwent spinal fusion. One was complicated by deep infection; the other underwent revision surgery due to pseudoarthrosis and screw pull-out. Wadia et al. [8] report two cases of camptocormia corrected with spinal fusion. The first patient had to undergo two revisions within a year of his index procedure due to hardware failure. The other also experienced hardware failure but was deferred from revision surgery due to poor general health. In the largest series to date, Koller et al. [9] studied 23 patients with PD, 10 of which had a previous failed back surgery. Overall, the revision rate was 33.3% (with an average follow-up of 14 months) while the surgical complication rate (infections and hardware failure) was 52.2%. In a study from Korea, Moon et al. [10] report their results on 20 patients with PD that underwent lumbar fusion. There was no statististically significant difference between the pre- operative and post- operative visual analog scale (VAS) scores in their cohort. Likewise, there were 4 instances of pseudarthrosis and one instance of screw pull- out. The authors state that their low rate of complications, in comparison to other studies of the same sort, is probably due to the short segment fusions that were performed in their cohort (14 one- level, 5 two- level and 1 three- level). Long fusions were studied in the paper from Bourghli et al. [11], wherein 12 patients with PD underwent posterior fusion from T2 to the sacrum for various disorders. Revision surgery was performed in 6 patients, 3 for hardware failure, 2 for proximal junctional kyphosis and one for epidural hematoma.
As the population ages and with improved results in medical and surgical treatments, increasing numbers of PD patients will require spine surgery. However, it is becoming increasingly clear that this subgroup of patients is at an elevated risk of complications and adverse outcomes. Indeed, the collective experience so far is that multiple re-operations have been necessary to achieve a satisfactory outcome in patients who already have to cope with a debilitating disorder.
Being older, PD patients are expected to have decreased bone mass. In addition, the very nature of the symptoms of PD forces patients to inactivity. This in turn results in disuse osteoporosis. Indeed, it has been demonstrated that PD patients have decreased bone mass when compared to age matched controls [12, 13]. Therefore, in addition to muscular dysfunction, poor bone quality further contributes to implant and fusion failure. The muscular dysfunction that results from PD not only makes the posterior tension band weak, but also makes spinal adjustment in areas adjacent to surgical fusions unfeasible. Myopathies of different kinds are quite common in PD patients [14-16], but even in the absence of a frank myopathy, the flexed posture that these patients assume will result in excessive loading of any implant.
Reports from orthopaedic and other surgical literature have also shown that PD patients are more likely to develop common complications such as pneumonia, confusion, urinary tract infections and decubitus ulcers [17]. Surgical site infections are also quite common, as described in the series of Babat et al. [5] and Koller et al. [9]. In our series, no deep infections were noted, which is most likely attributable to the small number of patients.
Management of spinal conditions in patients with PD is complex because of poor muscular supporting capability, diminished bone mineral density, motor control dysfunction in addition to the increased risk of surgical complications and the presence of comorbidities in this aged population. In general, before considering surgery, parkinsonian symptoms should be controlled as much as possible, whereupon a consultation with a neurologist is essential. Bone mineral density should also be evaluated and appropriately corrected. The patient should be monitored closely for the development of post- operative complications and rehabilitation should commence as early as possible [18]. For spinal surgery in particular, careful pre- operative planning for proper fusion level selection and restoration of sagittal balance is always fundamental, but in PD patients it is probably even more crucial. Koller et al. [9] also recommend adding fusion to any decompression surgery, and extending fusions as much as necessary into the thoracic spine or into the pelvis using S2 or iliac screws.
In conclusion, PD patients are a subgroup who from the outset present with advanced age and its associated comorbidities, brittle bone, postural imbalance, poor muscular strength and control as well as a propensity for developing common post- operative complications. As ours and others’ studies have shown, these patients are also at a higher risk to have failed back surgery and to undergo revision. As the evidence amasses, it is becoming increasingly clear that PD patients are a high risk subgroup. More studies are needed not only to clarify the exact causal relationship between PD and failed back surgery, but also to bring to light the appropriate surgical techniques to achieve better results for these patients.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

