All published articles of this journal are available on ScienceDirect.

Femoral Offset (3D) in Patients without Osteoarthritis – Index Values from 200 Hip Joints
Authors Info & Affiliations
Abstract
Introduction:
Femoral offset (FO) is a crucial parameter for hip joint biomechanics. Reference values for FO are particularly important when joint geometry has to be reconstructed during surgical interventions. Such reference values are scarce in literature and have mainly been obtained from osteoarthritis (OA) patients. The aim of this study was to conduct a patient-specific study of FO without osteoarthritis and to create a dataset of FO index values.
Materials and Methodology:
One hundred (49 female, 51 male; mean age: 59 (18 - 83) years) pelvic computed tomography (CT) scans were analyzed to determine FO in each patient. Bilateral symmetry and correlation between demographic data and FO were analyzed.
Results:
The mean FO ± SD was different for male (4.36 ± 0.56 cm) and female patients (3.95 ± 0.35 cm) (p <.0001). No Side differences of FO were observed in male and female patients. Significant correlation between height and FO was only observed in male patients.
Conclusion:
The values obtained in this study can be used as index values for the restoration and evaluation of hip geometry. For men, FO can be approximated using the correlation between FO and height.
INTRODUCTION
During total hip arthroplasty (THA) and the correction of deformities in the hip joint, anatomical relations between the pelvic and the femoral components of the hip joint are reconstructed. Depending on the diagnosis different strategies for the reconstruction are pursued ranging from exact anatomic reconstruction to remodeling of the joint geometry.
Although in primary THA a near anatomical reconstruction of the joint geometry is favored in most cases of revision surgery after THA, an increase in femoral offset (FO) to raise the abduction force by increasing the lever arm of the abductor muscles is discussed [1]. During the correction of congenital deformities, for example in high hip displacement after congenital hip dysplasia, a complete remodeling is performed by correcting the leg length and establishing a “new” hip joint femoral offset.
To establish a “new” joint geometry or reconstruct the existing one, patient-specific index values for key parameters such as hip center and FO are needed [2]. These values also make it possible to quantify the changes in hip geometry. Finally, index joint geometry values for FO are needed as well for a correct diagnostic evaluation of postoperative complications such as early hip joint dislocation [3, 4].
At present the contralateral side serves as a reference to assess if hip joint geometry has been restored correctly [5]. Where that is not possible due to preceding THA or congenital or posttraumatic deformities, patient-specific index values for FO are still not available. In the literature we could only find values from patients suffering from manifest osteoarthritis (OA) of the hip joint [6-8] or from cadaveric samples that were collected 100 years ago and all younger than 40 years at the time of death [9, 10]. In these studies no side differences of FO were observed but differences between the sexes were found.
Since the FO greatly influences the joint reaction forces and is therefore likely to influence the development of OA in the hip [11], we hypothesized that within a contemporary population without hip OA: i) FO would be different from the data obtained from OA patients, ii) the average measured for FO values would also be sex-specific, and iii) there would be no individual side difference. The aim of this study was to conduct a three-dimensional, sex-specific analysis of the FO and to create a dataset of FO-index values for men and women. This information will help to plan and interpret the correctness of hip joint reconstruction and remodeling more accurately.
MATERIALS AND METHODOLOGY
Demography
For this retrospective study patients were randomly recruited from the radiology clinic’s existing database over a period of four years from 2004 to 2008. Demographic data are shown in Table 1. The computed tomography scans (CT) ranged from the iliac crest to the proximal femur and included at least to the lesser trochanter.
Demographic Data of the Investigated Population Separated for Males and Females
| Female | Male | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | min | max | avg | sd | n | min | max | avg | sd | |
| age | 49 | 24 | 83 | 59.1 | 14.3 | 51 | 18 | 83 | 58.8 | 17.0 |
| height | 49 | 152 | 174 | 161.9 | 5.7 | 51 | 163 | 200 | 177.1 | 7.7 |
| body weight | 49 | 44 | 102 | 64.7 | 12.7 | 51 | 51 | 130 | 80.5 | 15.1 |
Age height and body weight exhibited a normal distribution (n number of patients; min minimum; max maximum; avg average; sd standard deviation).
The exclusion criteria were hip osteoarthritis Kellgren-Lawrence score ≥ 2, presence of hip endoprosthesis and fractures and tumors in the lower extremities.
CT Scans
CT scans were conducted in supine position using a Toshiba Aquilion 64© and a Philips Mx8000 IDT 16© Scanner. The slice thickness created was between 3 mm and 5mm at a Gantry inclination of 0°. Pixel size ranged from 0.583 mm × 0.583 mm to 0.885 mm × 0.885 mm.
CT data were analyzed using ImageJ and GnuPlot (both Public Domain). The method has been described to a certain extent already [12]. In brief: to avoid rounding during the 3D reconstruction, bony landmarks were marked in the 2D slices using image-processing software. Both the right and the left sides were analyzed.
Center of femoral head (CFH): coordinates of the femoral head center were marked manually in the slices of the greatest diameter in the horizontal plane (Fig. 1).
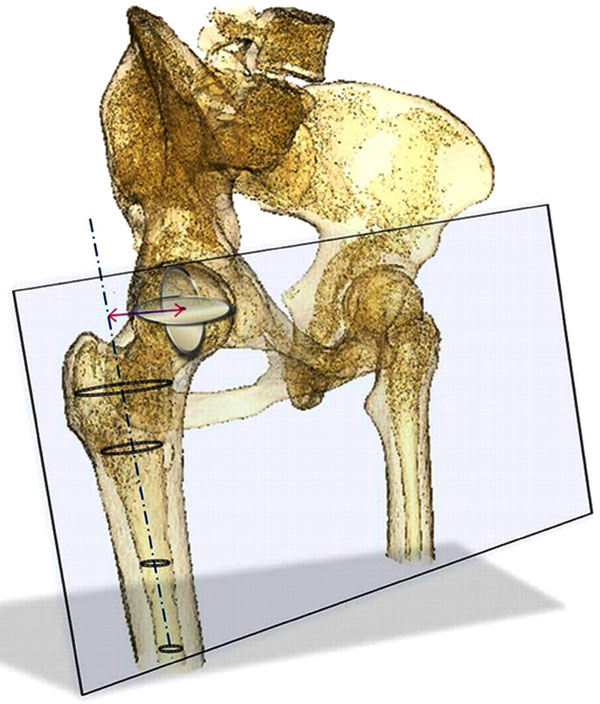
The 3D calculation of the femoral offset is schematically shown in a 3D-reconstruction of the pelvic bone and the proximal femur produced by the Amira 4.1.1 (Amira®, San Diego, California, USA) software package. Ellipses have been fitted automatically into the medullary canal (shown here for the right side). The femoral axis was calculated by the best line of fit through the ellipse-center points. A virtual plane was created containing the femoral axis and the center of the femoral head. The femoral offset was calculated as the distance between the femoral axis and the femoral head center perpendicular to the femoral axis.
Axis of the proximal femur (FPA): the proximal femoral axis was calculated as best line of fit for the centers of the ellipses that were automatically fitted to femoral medullary canal on each slide (Fig. 1).
Femoral offset (FO) was determined as the length of the vector perpendicular to the FA from the FA to the CFH (Fig. 1).
Statistical Analysis
Data were analyzed using the Kolmogorov-Smirnov-Z-test and Levene-Test for normal distribution and homogeneity of the variances. Correlation analyses as well as scatterplots were performed for demographic data and measurements of FO and BWLA were obtained. Pearson correlation analysis was used for parametric and non-parametric data as appropriate. A p-value less than .05 was considered to be significant.
RESULTS
Demographic data for male and female patient exhibited a normal distribution for age, height and body weight values. The data is shown in Table 1. Height and body weight values were significantly higher in male patients (p <.0001).
Mean FO ± SD was significantly different for male (4.36 ± 0.56 cm) and female patients (3.95 ± 0.35 cm) (p <.0001) but no significant side differences in FO were observed in male and female patients (p<.0001). Average values were therefore used for further correlation analysis.
Due to the significant sex differences in FO and height, separate correlation analyses between FO and demographic data were performed for males and females (Fig. 2a, b).
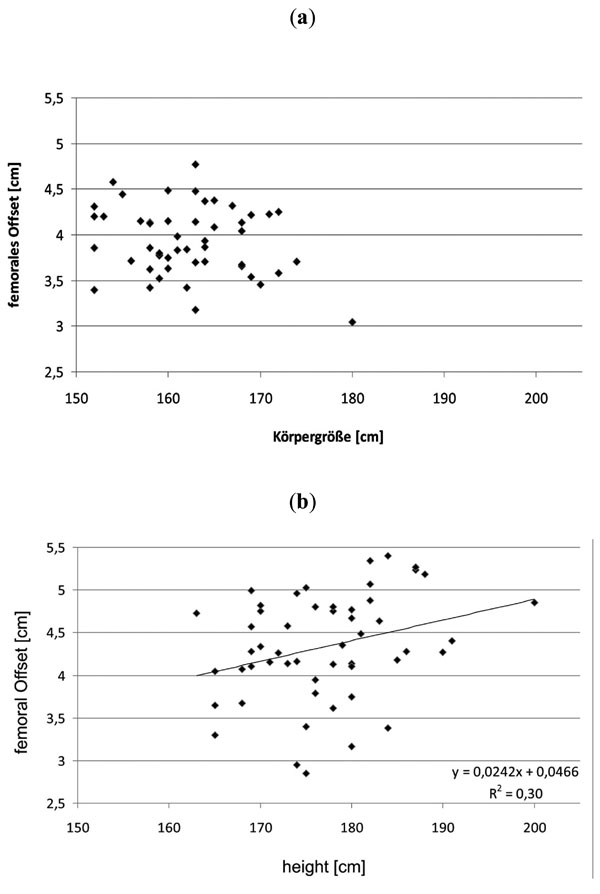
The scatterplot for the correlation between FO and height for both females (a) and males (b) is shown. Note: a significant correlation between FO and height could be observed in males, whereas such a correlation could not be found in females. A linear line of fit is given in the diagram for males (FO femoral offset). (r=0.09, n = 51, p<0.03).
In male patients a significant correlation between height and weight and FO could be observed (p 0.03). In female patients no significant correlation between any demographic data and FO could be observed. Correlation coefficients and p-values are given in Table 2.
Correlation of FO with Height and Body are Shown Together with p-Values
| Female | Male | ||||
|---|---|---|---|---|---|
| Height | Body Weight | Height | Body Weight | ||
| FO | corr. coeff. | -0.22 | 0.04 | 0.30 | 0.29 |
| p | 0.13 | 0.80 | 0.03 | 0.04 | |
FO femoral offset; corr coeff correlation coefficient.
DISCUSSION
In this study a 3D analysis was used to determine the femoral offset in 204 hip joints. FO turned out to be sex-specific and symmetrical. A significant correlation was found between height and FO in males, which allowed us to approximate height-specific values for FO. The values obtained represent index values that can be used to evaluate changes in the hip joint geometry after surgical interventions, mainly THA. This may make it possible to gain a deeper understanding of the postoperative symptoms that occur in patients after joint replacement procedures.
LIMITATIONS
A possible limitation of this study was that only the very proximal femur was scanned in the computer tomography, that could have caused a deviation of the calculated femoral axis from the anatomical shaft axis determined by the diaphyseal part and might have further influenced the values retrieved for the FO. The diaphyseal part, however, is neither the part where primary total hip prostheses anchor nor the area where muscles important for the biomechanical characteristics of the hip insert. We therefore took the very proximal part as the most relevant for the determination of FO.
Femoral offset in Patients with and without Osteoarthritis of the Hip
The FO measured in our patient population without OA yielded slightly lower values than Atkinson et al., and Maruyama et al., found in their investigations [6, 10]. A possible explanation for this might be that in their studies, the femoral axis was determined by the diaphyseal part of the femur, thus by the long femoral axis (FLA). Maruyama [10] has already described the influence of the deviation of those axes and the anterolateral bowing of the femur on the femoral offset.
Our study showed almost identical results compared to the data retrieved from the cadaveric samples in the study of Unnanuntana et al. [9]. Interestingly, the average height of the populations investigated almost completely match even though the average height of the general population has increased since those cadaveric samples were collected [13]. However, as the age limit in Unnanuntana's study was set at 40 years at the time of death the decrease of height with age was possibly excluded and might have assimilated the populations in terms of height. Furthermore, that population lived at a time when systemic bone diseases were more frequent and skeletal deformities altering the FO could have occurred more often. Although the measuring methods used in the study of Unnanuntana et al., were different, they also focused on the proximal part of the femur when determining the FO. Just as in our study neither Atkinson nor Unnanuntana found differences in FO between the patient’s left and right side [6, 9].
Femoral Offset and Joint Reaction Force
Studies based on 3D CT analysis of the FO in patients suffering from idiopathic osteoarthritis showed rather similar results [7, 8]. The virtual absence of differences between the values measured within these two populations is quite remarkable considering the influences of FO on the joint reaction forces [11]. Moreover, it has been shown that the FO is associated with the development of degenerative hip joint diseases [14, 15]. From investigations concerning joint wear and tribology we know that a decrease [16] in FO increases the wear between the articulating partners by increasing the joint reaction forces. Assuming that the femoral offset directly influences the development of osteoarthritis, we would have expected the FO to be higher in our patient population without hip osteoarthritis. Other parameters influencing the resultant joint reaction forces like pelvic geometry and bodyweight, however, were not captured. Therefore no conclusion could be drawn from the comparison of our values with those from Husmann et al., [8] and Sariali et al., [7] regarding the development of osteoarthritis.
Sex-Specific Femoral Offset
The sex-specificity of the FO measured in our study agrees well with earlier investigations [6, 9]. The absolute differences between the FO of males and females, however, vary between the study of Atkinson et al., and Maruyama et al., (both 7 mm, both 14%), Unnanuntana et al., (2.9 mm, 7%) and our study (4.1 mm, 9%). This deviation in the absolute expression of the sex-associated differences in FO can be explained by the different methods for determining FO. While in our study and Unnanunata´s the FPA was used to determine the FO, the FLA was used by Atkinson et al. and Maruyama et al. If the influence of the anterolateral bowing of the femur is taken into account, which is more pronounced in males than in females [10], these varying sex-specific relative differences can be accounted for.
Correlation of Femoral Offset and Height
We do not think that the significant correlation between height and FO found in males, but not females, should be attributed to the sex differences. Rather, we believe that the population investigated was too small and that in a larger population such a correlation would have been observed in females, too. The results of this study show that the contralateral side is the most accurate template for the reconstruction of the femoral offset for both men and women. Where the contralateral side cannot serve as a template, the FO values measured and the correlation found in our study might help to identify possible reasons for symptoms that occur postoperatively, as FO has been shown to be closely linked to the incidence of a variety of alterations [1, 3, 4, 17].
CONCLUSION
The FO was sex-specific and symmetric in this study. FO is clearly correlated to height in men, whereas such a height correlation could not be found in women. Although the absolute values obtained for FO can only be compared very cautiously, due to methodological differences between the studies, the FO in patients suffering from OA does not seem to differ from that in patients without OA. The results from this study can be used as index values for the establishment and evaluation of hip geometry when no other, more specific reference source is available. For men, FO can be approximated using the correlation found between FO and height.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

