All published articles of this journal are available on ScienceDirect.

Update on the Management of Compound Lower Limb Fractures
Abstract
Compound lower limb fractures pose a significant challenging pathology for orthopaedic and plastic surgeons to manage due to the combined soft tissue damage, bone injury and potential vascular compromise. These fractures require extensive team-work and expertise between several surgical specialties and the advice of non-surgical specialties, to ensure good clinical outcomes. Extensive research has improved the outcomes of compound lower limb fractures and current recommendation on the optimal management is always being updated to enhance patient outcomes. This review serves to provide an overview of the management of compound tibial fractures using current evidence and recently updated UK guidelines. The optimal time for surgical debridement, surgical intervention, antibiotic regime and soft tissue coverage will be outlined as well as the indications for amputation.
TREATMENT OF COMPOUND LOWER LIMB FRACTURES
Compound lower limb fractures are often complicated injuries to manage and require joint surgical experience and expertise from plastic, orthopedic and vascular specialists due to the associated soft tissue damage and musculoskeletal injuries. Compound fractures of the lower limb require immediate examination, systemic antibiotics, debridement and stabilization, followed by timed soft tissue coverage and extensive rehabilitation. This review aims to explain the new guidelines regarding compound lower limb fractures, highlighting a number of important issues including fracture examination, antibiotic use, timing of debridement and surgical intervention.
Several classification systems exist, to grade compound tibial fractures, in order to ensure appropriate management. The most widely used system is the Gustillo and Anderson score, which is based on three factors: (A) size of the open wound, (B) degree of contamination and (C) extent of soft tissue injury, as shown in Table 1 [1]. The Gustillo and Anderson system has been found to have poor interobserver reliability, especially among inexperienced surgeons [2]. However, due to its simplicity, the Gustillo and Anderson Score is recommended for daily use to assess the severity of a compound fracture [2]. Other more comprehensive methods of classification such as the AO system have not been found to be user friendly and therefore only recommended for audit purposes [3].
Gustilo and Anderson Classification of Open Fractures
| Grade | Criteria |
|---|---|
| I | Open fracture, minimal contamination, comminution and soft tissue damage, wound <1 cm in length |
| II | Open fracture, moderate contamination, comminution and soft tissue damage, wound > 1 cm in length |
| III | Open fracture extensive contamination, comminution and soft tissue damage. |
| IIIA | Type III fracture with adequate periosteal coverage of the fracture bone despite the extensive soft-tissue laceration or damage |
| IIIB | Type III fracture with extensive soft-tissue loss and periosteal stripping and bone damage. Will need further soft-tissue coverage procedure |
| IIIC | Type III fracture associated with an arterial injury-requiring repair, irrespective of degree of soft-tissue injury. |
The management of compound lower limb fractures needs to be standardised as district hospitals treat approximately 250,000 tibial fractures a year of which 25% of them will be compound fractures [4, 5]. Therefore, the British Orthopaedic Association (BOA) and the British Association of Plastic, Reconstructive and Aesthetic Surgeons (BAPRAS) have worked together, to create standardised guidelines ensuring the appropriate management of compound lower limb fractures in the UK [3]. These guidelines aim to improve patient outcomes [3]. In 2007, both parties came together to increase the awareness about compound fractures and to update the management of such injuries [3]. The British Infection Society and the Association of Medical Microbiologists were also asked to attend, to ensure antibiotic prophylaxis for open fractures is both adequate and appropriate [3].
The literature indicates that surgical experience, coupled with good multidisciplinary team-work, results in better outcomes for poly-trauma patients and complex lower limb injuries [6]. The treatment of compound fractures must therefore involve a multidisciplinary approach, involving close collaboration between orthopaedic and plastic surgeons [3]. A hospital that cannot provide this level of expertise should ensure that patients with such injuries are transferred to a specialist centre to ensure optimal surgical management can take place [3]. The UK guidelines recommend that the following patients should be transferred to specialist centers: (1) transverse or short oblique tibial fracture patterns, with fibular fractures at a similar level; (2) tibial fractures with comminution/butterfly fragments, with associated fibular fractures; (3) segmental tibial fractures; (4) fractures with bone loss; (5) soft tissue injury with skin loss where tension free, direct closure is not possible after wound debridement; (6) degloving injury; (7) injuries to more than one artery of the leg; (8) injury to muscles requiring resection of devitalised muscle, via wound extension [3].
IMMEDIATE MANAGEMENT ON PRESENTATION TO ACCIDENT AND EMERGENCY DEPARTMENT
Patients with compound tibial fractures must be assessed and managed appropriately following the Advanced Trauma Life Support (ATLS) guidelines [7]. Having sustained a compound tibial fracture means there is a major musculoskeletal injury, which suggests that these patients had been exposed to significant amounts of force. Therefore, meticulous assessment and management is vital to exclude any associated potential life or limb threatening condition [7].
The priorities of examination remain the same, with primary examination of: airway; breathing; circulation; disability and exposure, followed by secondary survey [7]. After life threatening injuries have been excluded, careful examination of the wound must be carried out as shown in Fig. (1) [3]. It is important to obtain the maximal amount of information about the mechanism of injury, to form an accurate idea of energy transferred during the injury. A high index of suspicion for sustaining tibial fractures is indicated when the history includes motor vehicle injuries, pedestrian vs vehicle injuries, a fall from a height greater than three meters, missile injuries, injuries involving entrapment, as well as lower limb ischemia [7]. A history suggestive of exposure to foreign material such as farmyard soil is likely to involve virulent pathogens, for example Clostridium perfringens [8]. Examination should commence with the skin to help exclude crush or burst wounds, large or multiple wounds and closed de-gloving injuries [7]. Signs of compartment syndrome, vascular injury and nerve injury must be investigated and managed immediately.
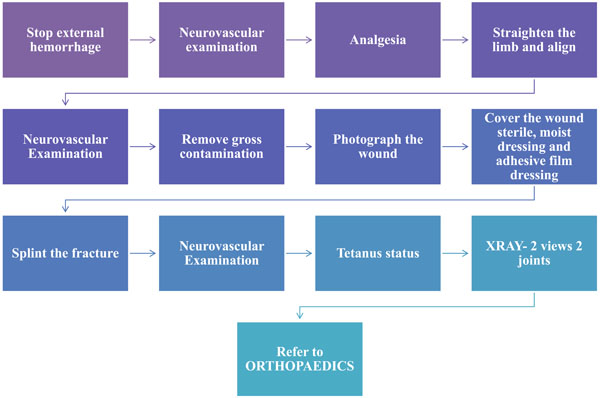
Method of managing open fractures in the accident and Emergency Department [3].
ANTIBIOTICS
Open lower limb fractures are often complicated by microbial contamination [1, 9]. The potential risk of infection and type of microorganisms depends on the severity of the associated soft tissue damage [10]. Many studies have been published on the correct surgical antimicrobial prophylaxis for lower limb fractures. A recent Cochrane review highlighted that immediate antibiotic prophylaxis is vital to decrease infection, however the exact type and duration of antibiotics is not clear [11]. The administration of antibiotics has been found to reduce the risk of infection in compound fractures by 59% [11]. Jaeger et al. in 2006 assessed the national Scottish and Swedish-Norwegian guidelines and the proposed German recommendations [12]. After reviewing the guidelines the authors recommended 24 hours of antibiotics following type I and II Gustillo fractures, 72 hours for grade III and no more than 24 hours of antibiosis for soft tissue injuries [12].
Taking blood cultures has not found to be useful as Lee et al. showed in a series of tibial injuries that only 8% of 226 organisms grown on cultures caused the tibial infection [13]. Therefore, the overall opinion is that cultures offer unneeded contamination and often show skin flora contaminants [13]. It has been found that most open fractures infections are cause by gram-negative rods and gram-positive staphylococci and so antibiotics should cover both species [13, 14]. However, in some open lower limb fractures cohorts MRSA has been found to be associated with the infection.
The optimal antibiotic regime to decrease the infection rate with open fractures is not clear from the literature. Patzakis et al. showed that Cephalothin, a first generation Cephalosporin, has a lower infection rate when compared to penicillin and streptomycin (2.3% compared to 9.7%) [15]. Numerous studies have shown that all open fractures should be treated with a combination of a first-generation Cephalosporin and an Aminoglycoside [16]. Other studies however, have advocated only adding Aminoglycoside for type III fractures [17]. The literature also indicates that Penicillin or Ampicillin should only be used, if there is a high risk of anaerobic infection [18].
Over the last ten years, interest has grown in topical antibiotic therapy, to prevent infection after compound fractures [19]. Topical therapy has shown to keep the optimal antibiotic therapy within the wound and reduce the risk of systemic side effects [19]. One way of providing topic antibiotic is to incorporate a heat resistant antibiotic in polymethyl-methacrylate cement, which is then placed in the wound cavity covered by a semi-permeable membrane [3]. Recently, Aminoglycoside-eluting polymethyl-methacrylate beads were studied by Ostermann et al. showing that 1085 compound fractures treated with Tobramycin-eluting beads had significantly lower rates of infection compared to those fractures not treated with the beads [20]. A recent study compared topical and systemic antibiotic therapy in the management of type II, IIIA, and IIIB compound fractures [21]. The findings illustrated similar rates of infection between local therapy with Tobramycin beads and systemic antibiotic therapy, which included a first-generation Cephalosporin [21]. Antibiotic bead pouches have been advocated by the British guidelines when there is segmental bone loss, gross contamination or established infection to decrease infection rates [3].
Due to the extensive literature it is now being advised that antibiotics should be administered as soon as possible after the injury, ideally within three hours [3]. The evidence to date supports the use of first generation Cephalosporins [3]. However, in the UK, this group of antibiotics is avoided due to the associated Clostridium difficile related diarrhoea [3]. Unfortunately evidence is limited with regards to non-Cephalosporin activity. Therefore, UK guidelines are based on microbiological principles and the likelihood the patients will be exposed to hospital organisms including Staphylococci, Coliforms and Pseudomonads as shown in Table 2 [3].
Antibiotic Classification from BAPRAS Guidelines [3]
| Indication | Antibiotic |
|---|---|
| Until first Debridement | Amoxiclav (1.2g 8 hourly) Cephalosporin (1.5g 8 hourly) |
| At first debridement continued until soft tissue closure or max of 72 hrs | Co-amoxiclav (1.2g) or a cephalosporin (such as cefuroxime 1.5 g) and gentamicin (1.5 mg/kg) |
| Induction of anaesthesia at the time of skeletal stabilisation and definitive soft tissue closure. | Gentamicin 1.5 mg/kg and either vancomycin 1g or teicoplanin 800mg. Not be continued post-operatively. |
| Anaphylaxis to penicillin | Clindamycin (600mg iv pre-op/qds) in place of co-amoxiclav/cephalosporin |
TIMING OF OPERATIVE INTERVENTION
Historically wound debridement was favoured within 6 hours of the injury; this management is supported by two studies [22, 23]. Kreder and Armstrong studied 56 open fractures and concluded that debridement within 6 hours decreased the infection rate from 25% to 12% [24]. The second study by Kindsfater and Jonasse showed operative treatment within 5 hours was associated with a lower risk of infection [25].
Many studies have recently brought the ‘6 hour’ window into question, as they have found no association between the rate of infection and timing of debridement [26-29]. Harley et al. found no increase in infection rate and non-union rate, when debridement took place up to 13 hours after the injury [26]. The study also concluded that the strongest predictor for deep-seated infection was the grade of the fracture and not the time to debridement [26]. Patkins and Wilkins further confirmed, that the greatest determining factor was the timing of antibiotics and not the delay of debridement for more than 12 hours [27]. Naique et al. compared debridement of compound fractures within 6 hours and between 6 and 24 hour and excluded any difference in infection rates [28]. Lastly, an extensive literature review by Crowley, investigating the time to debridement, showed that the 6 hour rule needs to be re-evaluated [29]. Due to the emerging new studies, the new British guidelines have stipulated, that debridement should be performed by a senior orthopaedic and a plastic surgeons and should be done on a routine trauma emergency list, within 24 hours of injury [3]. Although the guidelines have recommended that there are exceptions to this rule, for example immediate surgery is advocated when there is gross contamination, tissue devascularisation or compartment syndrome associated with the injury [3].
PRINCIPLES OF WOUND DEBRIDEMENT
Early thorough debridement is the most important surgical procedure for open lower limb fractures [1, 8, 10]. Debridement involves the excision of all devitalized tissue apart from the neurovascular bundles [1, 8, 10]. After the limb is cleaned with a soapy solution, all tissues must be assessed from superficial to deep [30]. It is important that all areas are explored and inspected carefully via appropriate wound incisions, to identify occult damage [31]. Muscle viability is assessed by following the rule of the four C’s. This means you should assess in turn the muscle’s colour, contraction, consistency and the capacity to bleed [31]. A second wound debridement should only be carried out if it is not possible to assess the soft tissue damage [32]. Serial debridements are not recommended has they have proven to be associated with poorer outcome [32]. Debridement aims to prepare the wound so that later elective surgical procedures can be carried out [3]. The wound must be extended along the nearest fasciotomy incision to gain an adequate view [3]. Dirt and debris should be removed [30]. Loose fragments of bone that are avascular, do not contribute to fracture union; they merely serve as a source of infection and must therefore be removed [32]. It is recommended to use copious amounts of warm saline to wash the bone; there is no additional advantage to using antiseptics or antibiotics [33].
If soft tissue debridement is not carried out immediately, the wound should be covered with a temporary dressing, which prevents bacterial influx and tissue desiccation [34]. Negative pressure systems, such as Vacuum Assisted Closure (VAC), is such a dressing that has been recommended [34]. De Franzo et al. demonstrated in 75 patients with compound fractures, that VAC dressings prevent the desiccation of cortical bone [35]. Negative pressures dressing have shown to decrease the infection rate in compound fractures, if applied before elective surgical intervention [36]. Conclusive evidence exists, that proves that the VAC devices are useful and safe in temporarily managing complex wounds or until definitive closure can be carried out [3].
SURGICAL STABILISATION OF COMPOUND TIBIAL FRACTURES
The optimal surgical fixation technique for compound tibial and femoral fractures remains a controversial topic. There are many ways of stabilising fractures including external fixation, plates and screws, reamed and undreamed locking nails.
PROVISIONAL STABILISATION
It is important that external fixation is applied as soon as possible, regardless of how soon definitive fracture fixation will take place [37, 38]. Early stabilisation is important to restore alignment of the limb, limit soft tissue damage and reduce gross movement at the fracture site [37]. This will improve blood circulation, and also reduce pain and stiffness [38]. Traction or long plaster slabs are not recommended for provisional stabilization [3]. Spanning external fixation is advised when definitive fracture fixation has not been carried out at the time of primary debridement [3]. When placing the external fixator the placement of the pins in the tibia, the fracture pattern and the future plastic surgical procedure that will be required must be considered, as well as the need to span the ankle and knee [39].
DEFINITIVE STABILISATION
Many factors determine whether stabilisation should be carried out with internal or external fixation. However, it is recommended that internal fixation should be carried out as soon as possible [37, 38]. The anatomy of the fracture determines the type of internal fixation used [3]. A diaphyseal injury, with minimal bone loss, is best treated with intramedullary nailing but articular fractures have a better outcome with plates [3]. Injuries with significant bone loss such as articular fractures, complex multilevel fractures or those associated with ankle or knee joint instability have better outcomes if stabilised using external fixation [3]. If internal fixation is used, than definite cover should be carried out simultaneously, as delaying definitive cover after internal fixation is associated with an increased infection rate [40]. The timing of optimal internal fixation is still debated [40]. Overall, external fixation is better when there is a significant amount of bone loss and fractures associated with smaller amounts of bone loss are best managed with internal fixation [3]. Furthermore internal fixation should not be used in highly contaminated injuries [3]. Lastly the dead space created, either from the debridement or the injury itself, will play a determining role when deciding upon the type of internal stabilisation best used [3].
TYPES OF FIXATION
Intramedullary Nailing (IM)
IM nailing remains a popular choice amongst surgeons, when treating tibial shaft fractures. In the systematic review by Bhandari et al., which included five randomized trials, unreamed nailing was favoured as the type of fixation device for treating tibial shaft fractures [41]. They investigated the rate of reoperation, nonunion and deep infection following unreamed nailing. It was concluded that the risk of reoperation was as high as 18%, implying that one reoperation would be avoided for every five patients treated with IM nailing instead of EF [41]. They also showed that there is a significant reduction in the risk of superficial infection with IM nailing, with one superficial infection avoided for every three patients treated [41]. They also found increase in the risk of nonunion and deep infection [41]. Another surgical dilemma is whether treating tibial fracture should be carried out using reamed or unreamed IM nailing. Theoretically, reaming the medullary canal and the placement of a larger nail will ensure better biomechanical stability [42-45]. Furthermore, reaming can be advantageous as it has shown in many multiple animal models to increase surrounding muscle and soft tissue blood flow [43-45]. However, there is an ongoing concern that there is destruction of the endosteal blood supply from reaming IM nailing, which could impact on bone healing [46]. Keating et al. compared reamed and unreamed nails and found no statistical difference between the two groups, with regards to time to union, rate of union, infection and frequency of implant failure (breakage of the nail) [44]. There was also no difference with functional outcome, when looking at timing of returning to work and recreational activity [44]. However, a significantly larger amount of broken screws was observed with the unreamed nails, but no increased number of broken nails [44]. Therefore, further data is needed to find out whether reamed or unreamed IM nailing should be used for fixation of tibial fractures.
External Fixator (EF)
EF has been very popular, in the treatment of open tibial fractures [47]. They are relatively easy to use and have a much shorter operating time, which limits the effect on the blood supply to the tibia [47]. However, there have been concerns about using EF due to the high incidence rates of pin site infection and the increased risk of malunion [47].
Sarmiento et al. reported a rate of 33% of patients suffering from malunion and a combination of shortening and angulations, following treatment of tibial fractures with EFs and functional braces [45]. These patients were then later offered an operation to correct the deformities [45]. Furthermore, 2.5% of patients were reported to go on to nonunion [45].
External fixation has been compared to unreamed nailing in the literature. A recent meta-analysis showed no statistically significant difference between these two methods of stabilisation with respect to union, delayed union, deep infection and chronic osteomyelitis [48]. External fixation was found to have a significant higher association with autologous bone grafting, due to an increased rate of malunion and further surgery [48]. Bhandari compared reamed fixation versus external fixation using a number of prospective studies and found reamed nails significantly reduced the risk of re-operation when compared with external fixators without reducing the rates of deep infection or nonunion [41]. Some surgeons feel immediate intramedullary nailing poses an increased risk of septic complications but delayed nailing after initial external fixation could decrease this risk [49-52]. Overall the studies which have investigated delayed IM nailing after initial external fixation have shown that rate of deep infection was 17%, with 2.5% developing chronic osteomyelitis, and delayed union rates of 14% and malunion 11%. Few studies have compared external fixation and delayed reamed intramedullary nailing. Inan et al. investigated the use of the Ilizarov external fixator (IEF) in 61 patients. The study demonstrated a shorter time to union with 19 weeks for IEF compared to 21 weeks for the IM nailing group [51]. They also reported complications such as pin tract infection, joint contracture in the IEF group and osteomyelitis in the IM nailing group. The study also showed four cases of malunion with IEF and similiarly in the IM nailing group [51].
PLATING
Bach et al. showed in their randomised trial that, when comparing plate and screws to external fixation, that 50% of patients treated by tibial plate required further operations as opposed to 6.7% in the external fixator group [52]. They concluded that these fractures are best treated with external fixators rather than plating, due to higher plate failure rate and complications such as deep infection and non-union [52].
SOFT TISSUE RECONSTRUCTION
Adequate soft tissue cover is vital to ensure infection-free fracture union [53]. Caudle and Stern reviewed the outcomes of compound tibial fractures and demonstrated that muscle coverage within 5 days had lower rates of infection and increased rate of fracture union [53]. Small and Mollan showed that early coverage, within 72 hours had lower complication and infection rates, when compared to those reconstructed after 72 hours [54]. Sinclair et al. also advocated early soft tissue reconstruction in his study. He reported a lower infection rate with definitive skeletal fixation and soft tissue reconstruction within 72 hours [55]. Hertel et al. compared the patient outcomes that were reconstructed on the day of injury, to patients who underwent reconstruction on average 4.4 days post injury [56]. Fracture union was greater and infection rate lower in the group that was treated on earlier [56]. The evidence highlights, that soft tissue coverage should be carried out as soon as possible [53-58]. The concept of ‘fix and flap’ - a term first coined by Marco Godina et al. [59] can only be used in specialist hospitals, where surgical expertise is readily available [3]. Complex reconstruction should only be undertaken, when the patient has been prepared and examined and the plastic and orthopaedic teams are able to work together [3]. However, is it advocated that definite soft tissue reconstruction should not be delayed for more than seven days under any circumstance [3].
MANAGEMENT OF ASSOCIATED VASCULAR INJURY
Devascularised limbs require urgent surgical exploration with the aim to restore circulation within 3-4 hours, in order to avoid irreversible muscle death [60]. Howard and Makin et al., proved that early exploration is needed as showed a 50% amputation rate, in delayed revascularisation after eight hours [58]. Devascularisation is commonly associated with displaced fractures of the femur and posterior fracture dislocations [3]. Absent peripheral pulses and reduced capillary refill, are indicators of vascular compromise which means a senior surgical opinion must be sought at once if these signs are present [3]. As soon as the site of injury has been identified during exploratory surgery, vascular shunts are the most optimal management strategy to restore blood flow [60]. Angiography has shown to cause unnecessary delay, when managing such injuries and are therefore not advised [60, 61]. If the limb is salvageable, the fracture must be stabilised with an external fixator, before replacing the shunts with reversed vein grafts [62]. The presence of vascular injuries can cause complications such as delayed fracture healing, infection and marked oedema that may increase compartment pressures leading to compartment syndrome and so any vascular compromise must be promptly managed [63].
INDICATIONS FOR PRIMARY AMPUTATION
The indications for primary amputation have significantly decreased with modern surgical techniques [3]. The UK guidelines are very strict in their indications for amputation. Indications for amputation include (1) an avascular limb exceeding 4-6 hours of warm ischaemia as literature has shown that the greater the ischaemia time, the more muscle loss takes place from necrosis, (2) [60] incomplete amputations where the distal part of the limb has been subjected to significant trauma, as seen with extensive crush injuries [3]. Furthermore, amputation is to be only considered for limbs with (1) segmental muscle loss affecting more than two compartments (2) segmental bone loss greater, than one-third of the length of the tibia and (3) open foot injuries associated with tibial fractures [3].
Recovery of normal plantar sensation occurs in over half of open tibial fractures patients who initially present with loss of sensation. Therefore, loss normal plantar sensation must not be assumed to be due to nerve division and is not an absolute indication for amputation [63]. Transtibial amputations are considered to be better treatment options than above knee amputation because of the decreased energy expenditure [64]. Long-term follow-up has shown better quality of life outcomes in individuals with below knee amputations when compared to individuals with above knee amputations, as patients have shown to adapt better to their new situation [65].
CONCLUSIONS
Compound fractures remain a challenging pathology to manage that will continue to need specialist’s input. Standardised guidelines of fracture management, based on extensive research, are improving the clinical outcomes. Literature clearly proves that antibiotics must be administered as soon as possible, to improve patient outcomes. The six-hour rule is no longer supported by current studies, and early stabilisation is advocated with the type of fixation determined by the soft tissue involvement, degree of bone involvement and other patient factors.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

