All published articles of this journal are available on ScienceDirect.

Traumatic Ceramic Femoral Head Fracture: An Initial Misdiagnosis
Authors Info & Affiliations
Abstract
Background and Purpose:
Ceramic heads are widely used in modern total hip arthroplasty (THA). Although a rare complication, fractures of ceramic heads are described in the literature, evoking uncertainties regarding the in vivo stability of this material, especially when impaction of a fractured ceramic head can lead to disastrous results.
Methods:
In this case report, we present a fracture of a ceramic head after trauma. A misinterpretation of the initial radiographs led to severe fragmentation of the ceramic head two weeks after the incident, later resulting in complete destruction of the arthroplasty.
Results and Interpretation:
Remarkably, radiographs obtained more than one year after the trauma led to this delayed diagnosis. A single radiographic evaluation, especially in patients with persistent pain after major trauma, with a ceramic head in a THA, seems to be insufficient
INTRODUCTION
In the 1970’s, Boutin implemented ceramic in modern total hip arthroplasty (THA). Although initial fracture rates of 13.4 % for ceramic heads were described before the 1990’s, the inferior rate of wear and friction when compared to metallic heads, and optimized tribology was very promising in THA [1-3]. Gradual improvements in processing of the material led to a significant reduction of the fracture rate to below 0.1 % [3]. Thus, alumina ceramic heads have currently become the standard material in THA with ceramic bearing surfaces.
Nevertheless, multiple case reports have been published describing ceramic head fractures [4-11]. The causes of fractures are diverse and vary from traumatic events [5, 9, 12, 13] to impingement between the neck and the liner rim [7]. Spontaneous fractures without any history of trauma have also been described [4, 6, 8, 10, 11]. However, only two reports describing delayed fractures of ceramic heads were found [12, 13].
In this report, we present a 24-year old patient who underwent primary THA at our institution and was a victim of high-energy trauma seven years later. Initial radiographs were misinterpreted in a non-designated total joint clinic at the time of primary admission (after the accident). A destructive ceramic head fracture was diagnosed more than one year after initial trauma at our institution, with major destruction of the ceramic head and the remaining THA. This was followed by an extensive revision. Based on this experience, the general question of adequate radiographic diagnosis after trauma to a THA, especially one with partial or full ceramic bearing surfaces, will be further discussed in this report.
PATIENT AND CASE DESCRIPTION
Case
A 24-year old patient with secondary osteoarthritis of the hips due to Legg-Calve-Perthes disease underwent primary hybrid THA of the left hip seven years before trauma, followed by primary cementless THA of the right hip one year later at our institution (Fig. 1) Six years after the right THA, he was involved in a motorcycle accident, in which he suffered direct trauma to this hip, as well as a complex ankle fracture which was treated in a smaller regional hospital on admission. Although initial anteroposterior radiographs of the pelvis and right hip axial views were performed, no signs of fractures, aseptic loosening or implant damage were diagnosed by the attending trauma surgeons (Fig. 2). Two weeks after surgical treatment of the ankle fracture, the patient noticed a sudden “cracking” sound in his right hip, as well as shortening of the right lower limb. Interestingly, the patient had no relevant pain.
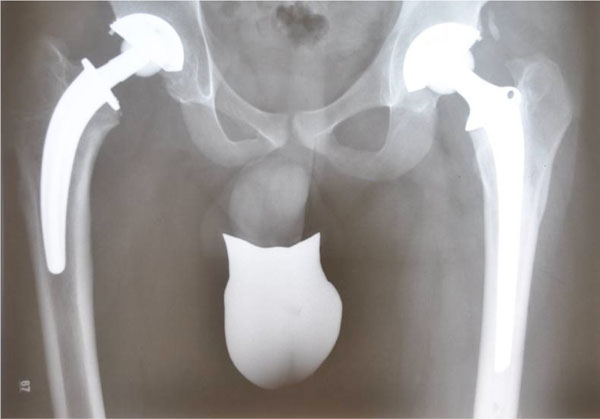
Anteroposterior pelvic radiograph (24 year old male) after primary THA for secondary osteoarthritis due to Perthes disease (Right Hip: cementless CFP stem and TOP acetabular cup; Left Hip: Hybrid THA with cemented ENDO Mark III stem + cementless TOP acetabular cup, Waldemar Link GmbH, Hamburg, Germany).
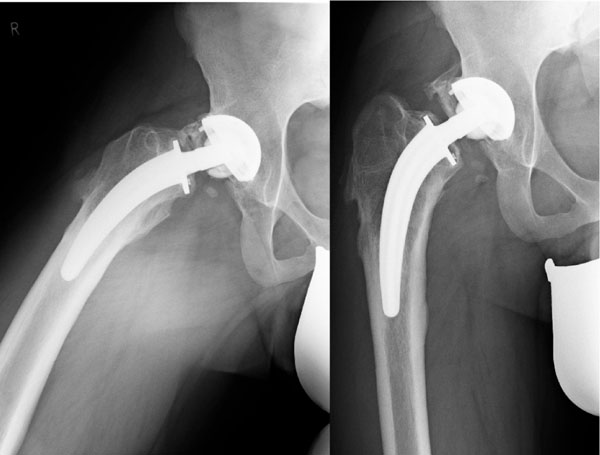
Conventional pelvic radiographs directly after trauma, revealing ceramic head fracture.
Despite this sign, he had no further medical observation or secondary radiographic evaluation over the next month. In the following months he was increasingly troubled by back pain and an unpleasant cracking “phenomenon” with movement of his right hip; no severe hip pain or associated direct thigh pain was mentioned at any time. Further conventional radiographs, in two planes, more than a year after the initial radiographs, revealed a completely destroyed multifragmented ceramic head (Fig. 3). A thorough clinical examination revealed a shortening of 2 cm of the right lower limb, yet the patient was able to walk without relevant pain.

Anteroposterior pelvic radiograph eight months after the initial radiographs, showing a fractured ceramic head.
Surgical Revision
Intraoperatively, extensive damage of the ceramic head and correlating taper junction of the femoral neck was found (Figs. 4, 6, 7). Concomitantly, there was severe debris-related metallosis throughout the entire joint (Fig. 5). The intervention consisted of conversion of the short cementless CFP stem to a cementless revision stem and an acetabular cup revision to a ceramic-ceramic bearing surface (Alloclassic stem and Allofit-IT acetabulum with Delta Ceramic Inlay, Zimmer, Warsaw, Indiana, USA and Ceramtec, Plochingen, Germany). Meticulous debridement of all affected soft tissues and extensive lavage was additionally performed.
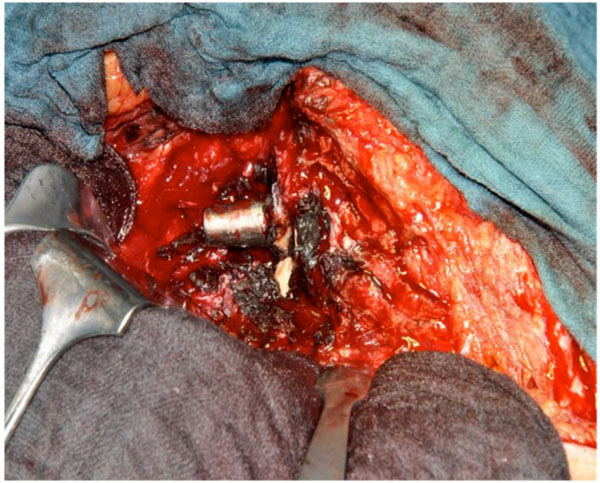
Intra-operative image showing countless debris and the damaged taper junction of the femoral neck (in situ).

Intra-operative image showing debris with ceramic fragments.
Intra-operative image showing the fragmentation of the ceramic head.

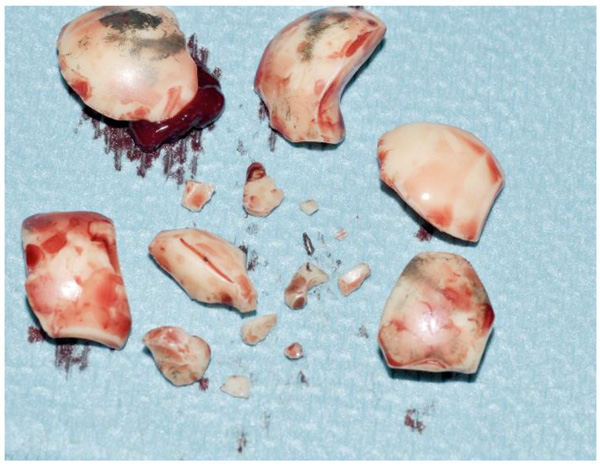
Image showing the explanted components: a fragmented ceramic head, a damaged stem and acetabular cup and liner.
Postoperative Treatment and Follow-Up
The postoperative course was uneventful, with radiographs revealing a correct position and articulation of the cementless implant (Fig. 8). A 12 month postoperative inquiry was performed and the Oxford Hip Score obtained, with both indicating satisfactory joint function [14]. The patient had no pain and was able to perform his daily activities.

Postoperative anteroposterior pelvic radiograph.
DISCUSSION
Although a relatively rare complication in modern THA, the described ceramic head fracture was misinterpreted in initial radiographs, which showed a discreet fracture of the ceramic head. Two assumptions can be made which led to this misdiagnosis. Firstly, the complex ankle fracture was probably more painful than the ceramic head fracture and this misled the surgeons. Secondly, which is more fact than assumption, is that the initial center of admission was incapable of reaching the correct diagnosis when one considers that the initial radiographs revealed a ceramic head fracture.
The “cracking sound” incident two weeks after trauma, as described by the patient, was probably due to the complete fracture of the ceramic head. Ultimately, a multifragmented ceramic head fracture was diagnosed one year later. This raises the question of the need of a possible guideline or recommendation for patients suffering acute trauma of the lower limb with a total hip arthroplasty, especially those with ceramic bearing surfaces.
This case remarkably demonstrates the variability and intensity of symptoms: when one considers the implants’ damage, the patient was able to walk without any pain originating from the hip. His only complaint was mild back pain over the subsequent months. This clearly presents a challenge for the assisting physician to obtain a correct diagnosis. The posttraumatic patient who previously underwent THA should therefore be carefully followed. We suggest a close follow-up including repeat conventional radiographs several weeks after trauma. Furthermore, in some cases, a CT-Scan could provide the correct diagnosis [15]. Ultimately, if a definite diagnosis in the initial assessment center (e.g. low volume or non-dedicated joint replacement center) cannot be assured, presentation of the case to a dedicated joint replacement center should be considered.
We present our case report to increase awareness among physicians and training staff who treat trauma patients who underwent previous total joint replacements, in order to expedite the diagnosis of possible posttraumatic implant fractures/failures.
ACKNOWLEDGEMENTS
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. No funds were received in support of this study.
CONFLICT OF INTEREST
The author(s) confirm that this article content has no conflicts of interest.

