All published articles of this journal are available on ScienceDirect.

Effect of Interlaminar Epidural Steroid Injection in Acute and Subacute Pain Due to Lumbar Disk Herniation: A Randomized Comparison of 2 Different Protocols
Authors Info & Affiliations
Abstract
In order to assess the efficacy of epidural steroid injections (ESI) in acute and subacute pain due to lumbar spine disk herniation, we conducted a randomized trial, comparing 2 different protocols. Fourty patients with radicular pain due to L4-L5 and L5-S1 disc herniation were assigned to receive either 3 consecutive ESI every 24 hours through a spinal catheter (group A) or 3 consecutive ESI every 10 days with an epidural needle (group B). All patients had improved Oswestry Disabilty Index (ODI) and the Visual Analog Scale (VAS) for pain scores at 1 month of follow-up compared to baseline, while no significant differences were observed between the 2 groups. The scores for group B were statistically significant lower at 2 months of follow-up compared to those of group A. The improvement in the scores of group B was continuous since the mean scores at 2 months of follow up were lower compared to the respective scores at 1 month. Protocol B (3 consecutive ESI every 10 days) was found more effective in the treatment of subacute pain compared to Protocol A (3 consecutive ESI every 24 hours) with statistically significant differences in the ODI and VAS scores at 2 months of follow-up.
INTRODUCTION
Low back pain and radicular pain is a socioeconomic problem of huge significance, affecting all age groups and economic classes. More than 70% of people in developed countries will experience low back pain at least once in their lives [1]. Disc herniation and spinal canal stenosis are the most common causes of low back pain. Particularly in the case of disc herniation, the pathophysiology of pain development involves not only a mechanical effect from the compression of the nerve root by protruded disk but the implication of inflammation around and within the compressed nerve root as well [2, 3]. Based on this inflammatory involvement, epidural steroid injections (ESI) have been extensively used with controversial results [4-16]. ESI can be accomplished by one of the following approaches; caudal, interlaminar or transforaminal. The aim of the present study was to assess the efficacy of 2 different protocols of interlaminar ESI in acute and subacute pain of the lumbar spine through a randomized comparison.
MATERIALS AND METHODOLOGY
Forty patients with a mean age of 52.4 years (range 28-60) and predominant radicular pain due to a lumbar spine herniated disc were prospectively randomized to 2 ESI protocols. We had 22 males and 18 females. The randomization was performed using random number tables. A detailed explanation of the type of the procedure and the possible side effects and complications were given to each patient. Written informed consent was obtained from patients before inclusion in the study. All patients had radicular pain due to L4-L5 and L5-S1 disc herniation that was documented with Magnetic Resonance Imaging (MRI) and electromyographic examination. Patients with extruded discs and stenosis of the spinal canal were excluded from the study. All patients had positive straight leg raising test and no patient had any neurological deficit. All of them had previously received conservative treatment for a period of 4 -6 weeks. Treatment was the same in both groups and consisted of a non-steroidal anti-inflammatory drug (diclofenac 100mg/day divided at 2 doses/day) and a muscle relaxant (thiocolchicoside 12mg/day divided at 3 doses/day). Despite conservative treatment patients had no improvement of the clinical presentation and all denied the proposed surgical intervention. No patient received any medication [analgesics, Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)] for the radicular pain within the previous 2 weeks before inclusion in the study protocols and during the protocol. Exclusion criteria were bleeding history, use of anticoagulants, known allergy to any of the components of the epidural injection, previous lumbar spinal surgery, radiologically proven facet syndrome and lumbar instability, extruded herniated discs, lumbar spinal stenosis and pregnancy. The institutional review board of the University Hospital of Ioannina approved the study.
Patients were assigned to 2 protocols. According to the first protocol (Protocol A) patients received the medication through an epidural catheter placed at the L3-L4 level with an interlaminar approach and a caudal orientation. The patients in this protocol had 3 consecutive ESI every 24 hours through the catheter. In the second protocol (Protocol B) patients had 3 consecutive ESI every 10 days with an 18-gauge epidural needle through an interlaminar approach at the L3-L4 level and a caudal orientation as well. All injections were performed by the same anesthetist blinded to patient’s protocol. Fluoroscopic guidance was used in both groups to ensure correct placement of the needle and thus enhance the safety of the procedure. The medication used in each ESI was the same in both protocols and included (3+3) mg of betamethasone acetate and betamethasone as sodium phosphate, 150mg clonidine and 5ml of 2% ropivacaine hydrochloride diluted with NaCl 0.9% till an overall volume of 10ml was achieved. All patients followed the same rehabilitation program that included restriction of their outdoor daily activities for 4 weeks after treatment, as they were allowed to indoor and outdoor activities after that period without being involved in their occupation (work).
Patients were evaluated before ESI and at 1 and 2 months after the last injection with the greek version of the Oswestry Disabilty Index (ODI) [17] and pain was estimated using a Visual Analog Scale for pain (VAS). Side effects from ESI were recorded. The evaluation of each patient was performed by an independent investigator blinded to the type of ESI that the patients received. A t test for independent samples was used to determine whether there was a significant difference in mean values of the pain scores or not. P < 0.05 was considered formally statistically significant; all p-values were two tailed. All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS 16.0 Inc., Chicago, IL, USA).
RESULTS
No patient reported any treatment-related side effect either acute or during the 2-month follow-up period. The outcomes are represented in Figs. (1, 2). No statistically significant differences were observed in the baseline scores between the 2 groups. The mean (SD) baseline ODI value before ESI was 54.8 (11.7) for patients in A group, while the respective score for patients in group B was 53.8 (6.3). The mean baseline VAS values were 7.0 (1.5) and 6.45 (0.8) for patients in A and B group respectively.
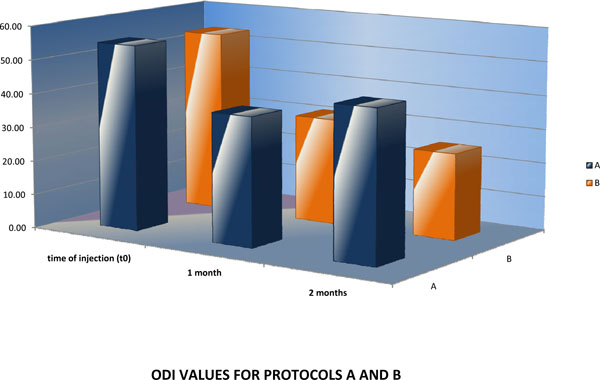
ODI values for protocols A and B.
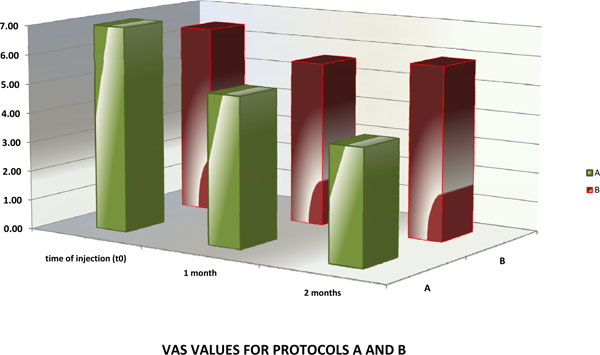
VAS values for protocols A and B.
All patients had improved scores at 1 month of follow-up compared to the scores before ESI. Patients enrolled in protocol B had lower ODI values [mean (SD) value of 31.4 (7.2)] compared to patients enrolled in protocol A [mean (SD) value of 37.9 (16.5), but the difference was not statistically significant (p = 0.18). The VAS values were similar in the 2 groups at 1 month of follow up [mean (SD) values of 5.1 (0.8) and 5.6 (1.7) in groups A and B respectively].
At 2 months patients that had 3 consecutive ESI every 10 days (group B) had statistically significant lower scores than patients that had 3 consecutive ESI every 24 hours through a catheter (group A). The mean (SD) ODI value was 25.4 (13.3) for group B and 44.2 (14.6) for group A, with a p value of 0.01 for the comparison between the 2 groups. Finally, the mean (SD) VAS value was 3.9 (1.4) for group B and 5.9 (2.1) for group A and the difference was also highly statistically significant (p = 0.01).
DISCUSSION
Lumbar epidural steroid injections is one of the most commonly performed interventional procedures for managing back and leg pain, sometimes used as the final non-surgical treatment modality before surgical intervention [4, 6, 7, 10, 11, 14]. Indications for lumbar epidural injections include low back pain associated with radicular symptoms, failure of medications, therapy and rest with persistence of functionally limiting back and leg pain beyond 6 weeks, advanced imaging studies demonstrating nerve root compression with clinical correlation or physical examination findings consistent with nerve root irritation (ie, positive dural tension signs and/or evidence of neurologic deficits). Contraindications are divided into absolute, such as the use of anticoagulants or the presence of coagulopathy, an active local or systemic infection and uncontrolled diabetes or spinal malignancy and into relative such as allergy to injectate, history of steroid psychosis, congestive heart failure, pregnancy or history of failed epidural injection [16].
The underlying mechanism of action of epidurally administered local anesthetic and steroid injections is not well understood. Multiple hypotheses have been presented. The effect is believed to result from interruption of the pain-spasm cycle and nociceptor transmission by the local analgesic and by reduced inflammation induced by the corticosteroids. Corticosteroids stabilize cell membranes, inhibit neural peptide synthesis and action, suppress neuronal discharge and suppress sensitization of dorsal horn neurons, while local anesthetics dampen C-fiber activity [18-27].
Five randomized trials related to lumbar interlaminar procedures that study patients with disc herniation and radiculitis exist in the literature [12]. Arden et al. [5] studied 228 patients with unilateral sciatica. Patients were assigned to receive either 80 mg of triamcinolone acetonide and 10ml of bupivacaine at 3 doses (weeks 0, 3 and 6) or placebo injections of 2ml of normal saline. Patients in the experimental group showed statistically significant improvement in function over placebo in 3 weeks, but this benefit was lost in 6 weeks. Wilson-MacDonald et al. [15] examined 93 patients with MRI evidence of a disc prolapsed, spinal stenosis or a combination. The experimental group underwent an epidural injection of 40mg bupivacaine 0.5% with 80mg of methylprednisolone, while the control group an intramuscular injection of 40mg bupivacaine 0.5% with 80mg of methylprednisolone. Patients in the experimental group showed a useful improvement in nerve root symptoms. Long-term relief was negative. Carette et al. [8] included 158 patients with sciatica due to herniated nucleus pulposus. The treatment group was injected with 80mg of methylprednisolone acetate and 8mg of isotonic saline, while the control group with 1ml isotonic saline. Both groups underwent 3 epidural injections 3 weeks apart. Significant improvement was seen in leg pain in the methylprednisolone group after 6 weeks with no difference after 3 and 12 months. Cuckler et al. [9] examined 73 patients with a clinical diagnosis of either acute herniated nucleus pulposus or spinal stenosis. The experimental group was given 80mg of methylprednisolone and 5 ml of procaine 1%, while the control group was given 2ml saline and 5ml of procaine 1%. No significant short or long-term improvements were notable between the two groups. Finally, Snoek et al. [28] included 51 patients with lumbar root compression documented by neurological deficit and a concordant abnormality noted on myelography. The treatment group was injected with 80mg of methylprednisolone, whereas the control group with 2ml of normal saline. No significant differences were noted in either group.
The present prospective randomized study represents the only available up-to-date study that compares one group treated with 3 consecutive ESI every 24 hours with another treated with 3 consecutive ESI every 10 days. Based on the results of our study, ESI were proved to be effective regarding the improvement of ODI and VAS scores in patients with predominant acute and subacute radicular pain due to lumbar spine herniated disks regardless of the protocol patients were assigned to. However, the scores for patients that had 3 consecutive ESI every 10 days were statistically significant lower at 2 months of follow-up compared to those that had 3 consecutive days ESI through a catheter. The improvement in the scores of group B patients was continuous since the mean scores at 2 months of follow up were lower compared to the respective scores at 1 month.
Some limitations of the present study should be acknowledged. First of all, it was a study that was limited to sample size. Other limitations include the small duration of follow-up and the absence of a control group. Another limitation is the possible source of bias resulting from the fact that all enrolled patients were those who rejected the surgery. It is unknown whether the reported results would be reproduced if patients that did not exclude a surgical procedure as a solution to their problem were included in the study. However, no statistically significant differences were observed in the baseline scores between the 2 groups.
CONCLUSION
The efficacy of 2 different protocols of interlaminar ESI in acute and subacute pain was assessed. All patients had improved scores at 1 month follow-up, with no significant differences between the 2 groups, whereas patients that had 3 consecutive ESI every 10 days showed significant lower scores at 2 months of follow-up with continuous improvement of their clinical condition.

