All published articles of this journal are available on ScienceDirect.

Effect of a Hyperkyphosis-specific Exercise Program on the History of Falls, Fear of Falling and Satisfaction in Older People with Hyperkyphosis: A Pilot Study
Authors Info & Affiliations
Abstract
Background:
Hyperkyphosis, an excessive curvature of the upper back, has been linked to increased falls and fear of falling. Previous work has focused on improving the hyperkyphosis curve itself. There is, however, a dearth of studies that have focused on improving falls, fear of falling, and participants’ satisfaction with the educational material.
Objective:
This study aimed to determine the effect of a hyperkyphotic-specific exercise programme on falling, fear of falling, and satisfaction with the educational material.
Methods:
Thirteen individuals with a hyperkyphosis of over 40 degrees were randomly divided into an exercise group (n=6; age: 71.50 ± 7.84 years) and a control group (n=7; age: 67.29 ± 9.76 years). The exercise group received a 16-week hyperkyphosis-specific exercise programme with educational material. The control group received only the educational material. Before and after the exercise programme, the history of falls in the past year and fear of falling were assessed by 2 questionnaires (the history of falls in the past year and the Fall Efficacy Scale-International). Satisfaction with the educational material was evaluated after the exercise programme. Data were analysed by descriptive statistics and a 2×2 model mixed between-within subjects analysis of variance.
Results:
There was no significant interaction between group and time for the history of falls in the past year (p = .182, effect size = .156) and fear of falling (p = .216, effect size = .135), but the effect size of the interaction effect was large. Furthermore, participants in both groups expressed positive satisfaction with the educational material.
Conclusion:
Hyperkyphosis-specific exercise programme resulted in improvement in the history of falls and fear of falling, but the results were not significant. A larger randomised controlled trial is needed to clarify the effectiveness of the exercise programme in reducing the number of falls and fear of falling in this population.
1. INTRODUCTION
Age-related hyperkyphosis is the most prevalent spinal deformity in older adults. It is characterised by an excessive forward curvature of the thoracic spine (> 40°) [1, 2]. Hyperkyphosis has a significant negative impact on the health outcomes of older adults [3]. The consequences of having hyperkyphosis are reported to be impaired physical function [4], decreased balance [5], increased risk of falls, and reduced quality of life [1, 6, 7].
In terms of biomechanics, increased anterior thoracic curvature in the spine shifts the body’s center of gravity towards the limits of stability, which may perturb the person’s balance, thereby increasing fall risk [8-10]. It has, therefore, been postulated that knowledge and exercise programme to reduce thoracic kyphosis may decrease the risk of falls in older persons with hyperkyphosis. Furthermore, the knowledge gained on thoracic hyperkyphosis could be used to develop a comprehensive treatment programme and prevent falls in older adults.
Hyperkyphosis-specific exercise programmes have been suggested as the first step in the treatment of patients with hyperkyphosis [11]. Hyperkyphosis-specific exercises comprise of a programme of exercises focused on multiple musculoskeletal impairments, including spinal extensor weakness, poor postural alignment, and reduced mobility of the thoracic spine. Specific exercises included spinal extensor strengthening, improved thoracic mobility, and postural alignment correction [12, 13]. A systematic review by Bansal et al. [11] evaluated the effectiveness of exercises on the thoracic kyphosis angle in older adults. This review revealed that the evidence regarding the effects of exercise on the thoracic kyphosis angle is limited and of low methodological quality. Sinaki et al. [14] reported that a 4-week specific back extension and gait programme combined with a spinal weighted kypho-orthosis improved balance and fear of falling in older female adults with osteoporosis-kyphosis. Furthermore, Sh et al. [15] conducted a quasi-experimental study to evaluate the effect of corrective exercises on falls and fear of falling in 30 elderly women people with hyperkyphosis. They demonstrated that a corrective exercise programme was able to reduce the fear of falling and the number of falls in elderly women with hyperkyphosis. Berdishevsky [16] conducted a case study to investigate the effects of a hyperkyphosis-specific exercise programme combined with the SpinoMed brace on the kyphosis angle, pain, quality of life, and spinal muscle strength in women patients with Scheuermann’s kyphosis aged 76. The researcher demonstrated that the hyperkyphosis-specific exercise programme and SpinoMed braces were effective for the treatment of their patient. The results from the above studies have limited generalizability to the older male population. Furthermore, little is known about the effect of hyperkyphosis-specific exercises on reducing falls and fear of falling in elderly people.
In contrast to the mentioned studies, the study conducted by Greendale et al. (2009) [17] demonstrated that 24 weeks of yoga decreased hyperkyphosis but did not improve either the balance or the fear of falling in older adults with thoracic hyperkyphosis. In summary, the evidence regarding the effectiveness of exercise interventions on falls and the fear of falling appears very limited and still controversial. To date, despite a comprehensive search, no studies could be found that examine the effects of a hyperkyphosis-specific exercise programme on falls and fear of falling in older people with hyperkyphosis.
Numerous authors suggest that exercise programmes are feasible and safe for older people with hyperkyphosis and may lead to improved thoracic kyphosis [18, 19]. Bautman et al. (2009) [20] explored compliance with spinal rehabilitation (e.g., spinal mobilisations, taping, and exercises for spinal correction) and the safety of rehabilitation in hyperkyphotic patients. They demonstrated that spinal rehabilitation is safe, but the exercise program has low compliance. However, the evidence for the adherence to the study as well as the safety of implementing a hyperkyphosis-specific exercise intervention for the elderly population, is still limited.
In the management of spinal deformities, postural education, which consists of information and advice, is commonly used for improving spinal posture [21]. Several studies gave educational booklets about postural education for treating thoracic hyperkyphosis [13, 22]. Despite this need for the management of thoracic hyperkyphosis, no previous research has investigated participants’ satisfaction with the educational booklet.
Therefore, this study aimed to investigate the effect of a hyperkyphosis-specific exercise programme on falling, fear of falling, and participants’ satisfaction with the educational booklet in older adults.
2. METHODS
2.1. Research Design
The current study was designed as a pilot study for a randomised controlled trial to investigate the effectiveness of a 16-week home-based hyperkyphosis-specific exercise programme on falling, fear of falling and participants’ satisfaction with the educational booklet in older people with hyperkyphosis. This study was approved by Teesside University, School of Health and Life Sciences, Ethics Committee (study number: 263/18). The participants were recruited into this study through poster advertisement. Posters were placed on the Teesside University, cafes, shops, libraries, community centres, church halls in Middlesbrough and Stockton-on-Tees. Participants who have a thoracic kyphosis angle ≥ 40° were randomly assigned to either the exercise group (hyperkyphosis-specific exercises together with a postural educational booklet) or the control group (the postural educational booklet). The randomisation procedure used opaque sealed envelopes to randomise participants.
2.2. Participants
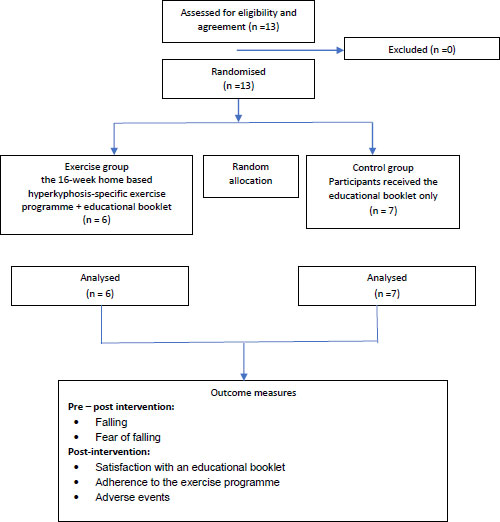
Individuals were eligible if they were male or female, aged 50 or older, had a thoracic hyperkyphosis of 40°, were free of any medical conditions affecting balance, had the ability to stand independently, and could walk independently without the use of a gait aid. The exclusion criteria include peripheral neuropathy, inner ear disorders or severe hearing loss, visual impairment, neurological or musculoskeletal disorders or medical conditions that prevent participants from exercising; prescription drugs are known to affect the central nervous system; history of spinal or lower extremity surgery; and a diagnosis with vertebral compression fractures within 6 months of the study; inability to perform the exercises, diagnosis of brittle bone diseases, and serious medical conditions that limit participation in the exercise programme. The flow of participants through the study is shown in Fig. (1).
2.3. Measurement
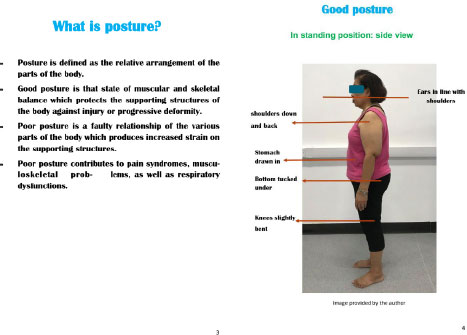
Falls are defined by the World Health Organization as "an event which results in a person coming to rest inadvertently on the ground or floor or another level, excluding intentional change in position to rest on furniture, wall or other subjects" [23]. A history of falls is a good predictor of future falls. It is important to specifically ask all patients if they have fallen in the past year [24]. Panel on Prevention of Falls in Older Persons and Society (2011) [24] has recommended that all older individuals should be asked whether they had fallen in the past year. The history of falls was assessed by asking participants if they had had a fall in the past year. The history of falls needs to include a detailed description of the circumstances of the fall(s), frequency, symptoms at the time of fall, injuries, and other consequences.
Fear of falling was assessed using the Falls Efficacy Scale -International (FES-I). The FES-I was used to evaluate the degree of confidence in performing activities of daily living without falling [25, 26]. The FES-I is a 16-item questionnaire of falls-related self-efficacy (self-perceived confidence in performing daily physical activities) based on the Falls Efficacy Scale (10 items). The 16 items of the FES-I are rated on a 4-point Likert scale for 16 different activities according to “how concerned you are about the possibility of falling”, using the following responses (score in parentheses): not at all (1), somewhat (2), fairly (3), and very concerned (4). The questionnaire is published in full elsewhere [25]. The reason for selecting the FES-I questionnaire was due to the suitability of this test for ambulatory older participants.
To assess participant satisfaction, there are several questionnaires have been designed to assess participant satisfaction. The satisfaction of the educational booklet questionnaire proposed by Kandasamy has been validated for low back pain patients [27]. Satisfaction with the educational booklet was assessed using an adaptation of the satisfaction questionnaire. The items included in this survey evaluated the general impression, information, presentation, ease of use, and satisfaction with using the postural educational booklet provided. This questionnaire is a validated tool, an 8-item scale with five-point Likert scales ranging from strongly disagree (1) to strongly agree (5) or very bad (1) to very good (5) [27] (Appendix A).
2.3.1. Exercise Programme Adherence and Safety
Adherence to the study was monitored throughout the study for compliance and was obtained by recording the number of exercise sessions attended (out of a maximum number of 48). Adherence to the study was expressed as a percentage. Participants in the exercise group were asked to record their compliance with the exercises in a logbook. The participants in the control group were also asked to record their physical activity in a logbook.
Adverse events refer to any untoward medical occurrences and problems that are possibly related to study participation and that are serious or unexpected. Serious adverse events, including death, life-threatening experiences, and related inpatient hospitalisation were reported during participation in the current study. Participants were asked to report adverse events to the researcher and the safety logs for every exercise session.
2.4. Intervention
The exercise group received an individualised home-based exercise programme and an educational booklet to guide participants in self-performance at home. The participants in the exercise group were taught a hyperkyphosis-specific exercise programme by an experienced physiotherapist who is certified as a Schroth therapist and a Schroth Best Practise therapist. The exercise programme included the physio-logic® exercise, 3D exercise made easy, sitting exercise in a doorway, standing exercise in a doorway, and hand behind neck exercise (Table 1) [28]. In addition, the exercises were implemented in activities of daily living. The exercise programme was modified depending on the participant’s symptoms and tolerance. Exercise group participants, for example, reported discomfort when performing exercises that required lifting the arms above the level. The exercise program was altered by reducing the number of repetitions. The educational booklet is given to each participant at the first session of the exercise programme. The educational booklet presented information about hyperkyphosis, posture correction, and all of the exercise-related information, together with an illustration of each exercise (Appendix B).
| Exercises | Details of Exercises | Figures |
|---|---|---|
| Symmetrical exercises (The physio-logic® programme) | Symmetrical exercises for sagittal profile correction. Exercises for the mobility of lumbar lordosis and thoracic kyphosis improvement. | Standing position Sitting position  Walking  Repetitions: 10 repetitions × 5 sets; practice once a day. |
| Three-dimensional trunk correction (3D exercise made easy) | The participants were instructed on how to achieve 3D trunk and pelvic correction while a specific breathing technique focused on improving the collapsed area (anterior chest). |
 Repetitions: 10 repetitions × 5 sets; practice once a day. |
| Isometric muscle tension (New Power Schroth) | The correction of body posture, elongation of the spine, corrective breathing technique, as well as a correction with isometric muscle tension. The position exercises were focused on sitting and standing positions. |
 Repetitions: 10 repetitions × 5 sets; practice once a day. |
| Patient education (ADLs) | Patient education to maintain the corrected posture while performing ADLs. The participants were taught to take corrective positions in everyday activities whilst walking, sitting, and standing. | The exercises are adapted to ADLs
|
For the start-up of the exercise programme, the exercise group learned to properly perform the exercise programme. Participants were instructed to perform a minimum of 5 sets of 10 repetitions of each exercise once a day, three days a week. The exercise training sessions lasted between 20 and 30 minutes. The initial level of the participant was decided through information from the participant on their exercise habits over the last 6 months and their medical conditions (e.g., shoulder pain, neck pain). After the first week, training intensity was progressively and individually increased over 16 weeks exercise programme by increasing the number of sets for each exercise depending on the participants’ symptoms and tolerance. Participants were asked to record their exercises in a log documenting and were requested to refrain from participating in other forms of exercise during the study.
For follow-up visits, the participants returned for the researcher consultation every week for the first 4 weeks to monitor their adherence to the study. This monitoring was to ensure that the exercises were being performed correctly as well as to motivate and or encourage participants to continue doing their exercises. After week 4, the participants were contacted by the researcher every week through email or phone to discuss the progression of the exercises.
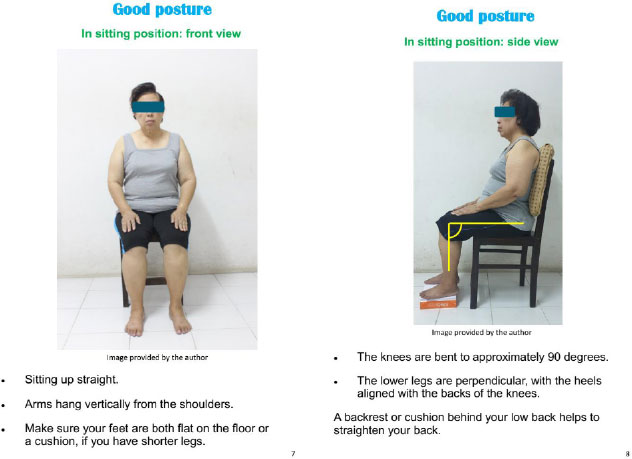
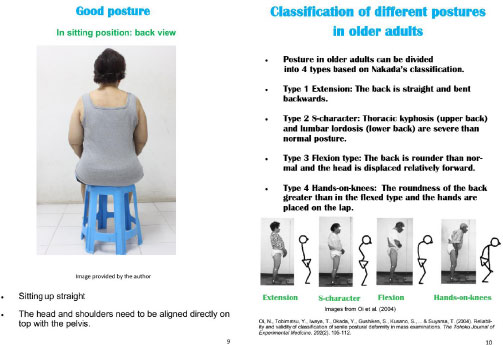
The control group did not participate in the exercise programme but received an educational booklet made for the control group. This comprised a description of the characteristics and caused as well as the consequences of having thoracic hyperkyphosis, ideal posture in sitting and standing, as well as classification of postural deformity in older adults on the first visit. Further, the control group was asked not to participate in any other activities or formal exercises during the study period.
2.5. Statistical Analysis
The data analysis was performed using the IBM SPSS statistical software version 26.0 for Windows (IBM Corp., Armonk, NY, USA), and the level of statistical significance was set at p < 0.05.
The Mann-Whitney U test was chosen to determine if there were any differences in the characteristics of participants at baseline between the exercise group and the control group.
With regard to the history of falls and fear of falling, a 2×2 mixed analysis of variance (ANOVA) with a time factor (pre-test and post-test) and a group factor (exercise group and control group), was carried out to identify the main effect of the intervention and time as well as the interaction effect on the history of falls and fear of falling. To control confounding factors in comparing data between groups, an ANCOVA was conducted for falls and fear of falling to identify post-intervention differences between the two groups, using the baseline value and age as a covariate. Satisfaction with the educational booklet was analysed by using descriptive statistics (percentage and frequency distribution) to describe the sample.
A power analysis was performed for the calculation of the sample size using G*power version 3.1.9.2 based on the study of Jang et al. [29] (similar study). The groups specified were a test power of 0.80 with a significance level of 0.05, calculated with a sample size of 14. To adjust for a dropout rate of 20%, the total required sample size was 18.
3. RESULTS
3.1. Participant Characteristics
Thirteen participants completed the study and were randomly assigned to the exercise group and the control group. There were no statistically significant differences in demographic characteristics between the groups at baseline Table 2.
| Baseline Characteristics |
Exercise Group (n=6) |
Control Group (n=7) | P-value | U | z |
r (Cohen’s d) |
|---|---|---|---|---|---|---|
| Age (year) | 71.50 ± 7.84 | 67.29 ± 9.76 | 0.430 | 15.50 | -.79 | .22 |
| Height (cm) | 168.00 ± 14.96 | 163.29 ± 6.54 | 0.721 | 18.50 | -.36 | .10 |
| Weight (kg) | 65.83 ± 20.19 | 69.86 ± 11.26 | 0.152 | 11.00 | -1.43 | .40 |
| Body mass index | 22.86 ± 2.81 | 26.15 ± 3.54 | 0.063 | 8.00 | -1.86 | .52 |
| Thoracic kyphosis (°) | 62.56 ± 6.07 | 58.67 ± 7.38 | 0.223 | 12.50 | -1.22 | .34 |
| History of falls (falls/person-years) |
0.50 ± 1.22 | 0.57 ± 0.79 | 0.081 | 12.00 | -1.74 | .48 |
| Fear of falling (score) | 19.33 ± 2.58 | 18.29 ± 2.21 | 0.823 | 19.5 | -.22 | .60 |
| Gender (M: F), (n) | 2:4 | 3:4 |
3.2. Changes in the History of Falls and Fear of Falling
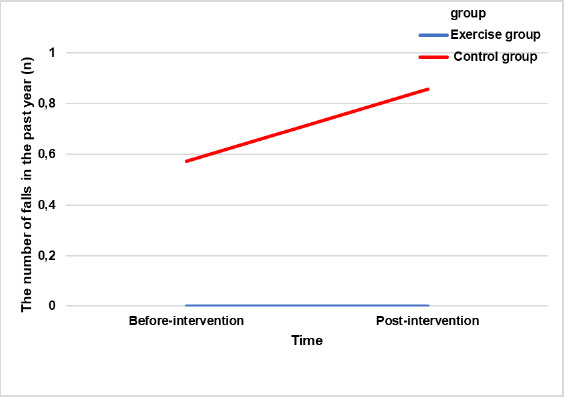
There was no statistically significant interaction of group and time, indicating that there was no difference in the number of falls in the past year over time in favour of either group [F (1,11) = 2.031, p = .182, effect size = .156]. However, even though the result was not significant, the effect size was large (Figure 2). There was no statistically significant main effect of time; this indicates that there was no change in the number of falls in the past year after the intervention [F (1,11) = 2.031, p = .182, effect size = .156]. However, even though the result was not statistically significant, the effect size was large. The main effect of the group was also not significant, F (1,11) = .122, p = .734, effect size = .011, suggesting no difference in the effectiveness of the exercise programme between the exercise and the control groups.
The analysis of covariance showed that after controlling for age, gender, and falls at baseline, there was no statistically significant difference in the number of falls in the past year between the exercise and the control groups [F (1,13) = 0.238, p=0.639, effect size = 0.029].
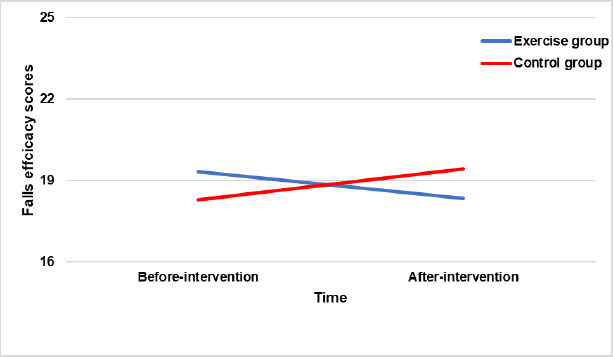
For fear of falling, there was no statistically significant interaction between group and time. It shows no difference in fear of falling score over time in favour of either group [F (1,11) = 1.72, p = .216, effect size = .135]. However, even though the result was not statistically significant, the effect size was large (there was a possibility that significant changes would be observed if the sample size increased). This indicates that the fear of falling decreased in the exercise group but increased in the control group after 16 weeks (Fig. 3). In other words, hyperkyphosis-specific exercises can help to decrease the fear of falling.
The main effect of time was not statistically significant, F (1,11) = 0.008, p = .932, effect size = .001. This indicates that there was no change in the FES-I scores after the intervention. The main effect of the group was also not statistically significant, F (1,11) = .000, p = .987, effect size = .000, suggesting no difference in the effectiveness of the exercise programme between the exercise and the control groups.
The analysis of covariance showed that after controlling for age, gender, and fear of falling at baseline, there was no statistically significant difference in fear of falling between the exercise and the control groups (F (1,13) = 0.028, p = 0.871, effect size = 0.003).
3.3. Satisfaction with The Educational Booklet
Thirteen participants (100%) completed the survey on their satisfaction with the educational booklet. Please note that the groups (a) used different booklets and (b) took part in different study conditions. Therefore, presumably, it is not meaningful to compare the two booklets. This is because booklet type and study condition are confounding variables.
Overall, participants in both groups reported positive comments about their experiences with the educational booklet (the exercise group = 100% and the control group = 100%). Participants in both groups reported that they were satisfied with the educational booklet. In addition, they also reported that the booklets were easy to understand with well-presented images of correct body posture in sitting and standing (the exercise group = 100% and the control group = 100%). The exercise group was more positive about the benefits of managing their self-care (the exercise group = 83.4% and the control group = 67.2%) and ease of use (the exercise group = 100% and the control group = 85.7%) and stated that they intended to continue the exercise programme after the research study ended (the exercise group = 83.3% and the control group = 57.1%). Participants in both groups preferred to receive an educational booklet in printed form rather than electronic form (the exercise group = 100% preferred the booklet version, and the control group = 85.7% preferred the booklet version). The summary of satisfaction with the educational booklet for both groups is presented in Appendix C.
3.4. Adherence to Study and Safety
Adherence to the study was excellent. Five of the 6 participants (83.3%) in the exercise group attended all 48 exercise sessions (3 sessions per week for 16 weeks), with one attending 47 exercise sessions. The reason for non-attendance was being unwell. After the first four weeks, the researcher contacted the participants by phone, email, and message every week during the study to determine if any problems were encountered with the exercises and to check their progress with the exercise programme. The current study suggests that the exercise intervention is acceptable based on the number of exercise sessions attended by the participants.
No serious adverse events were reported relating to the exercises during the study period. However, it should be noted that four of six participants in the exercise group initially reported some discomfort when a new exercise was introduced. However, those symptoms eased when they continued the exercises or were resolved by a slight modification of the exercise by the researcher. Therefore, the current study suggests that the intervention is safe for older adults with hyperkyphosis.
4. DISCUSSION
The results of the study suggested that the number of falls in the past year and fear of falling showed no significant interaction between group and time, but the effect size of the interaction effect was large. This means that the number of falls in the past year did not change over time in the exercise group but increased in the control group, and fear of falling decreased in the exercise group but increased in the control group after 16 weeks. Moreover, participants in both groups were satisfied with the educational booklet provided (e.g., easy to understand and use, and well-presented images of correct body posture in sitting and standing were beneficial in managing their spinal self-care).
The number of studies conducted on the effectiveness of exercise interventions for age-related hyperkyphosis has increased in recent years [11, 29]. However, there are no published the effect of a hyperkyphosis-specific exercise programme on falling fear of falling and satisfaction with the booklet in older adults with hyperkyphosis. To the best of the author’s knowledge, this study is the first to focus on the effect of a hyperkyphosis-specific exercise programme on falling, fear of falling, and participants' satisfaction with the educational booklet.
The current study found that the history of falls in the past year indicated no statistically significant interaction between group and time, but the effect size of the interaction effect was large. This means that the history of falls did not change over time in the exercise group but increased in the control group. In other words, the evidence shows the exercise programme can help prevent falls.
There is a dearth of literature on the effect of exercise interventions on the number of falls in older adults with thoracic hyperkyphosis. Although, the result of the current study conflicts with a previous study by Shahrjerdi et al. [30], who found that the number of people at risk of falling was reduced from 7 to 2 cases after an 8-week (3 sessions/week) corrective exercise programme.
In addition, Madureira et al. [31] conducted a study to investigate the effect of 12 months of balance training on the number of falls in the year before the study. They demonstrated that the balance training programme was able to reduce the number of falls in older women with osteoporosis.
A possible explanation is a difference in the characteristics of the participants. The current study recruited both genders (n = 13), whereas a study by Madureira et al. [31] recruited only elderly women with osteoporosis (n = 60), and Shahrjerdi et al. [30] recruited elderly women with thoracic hyperkyphosis (n = 30). The current study did not find a significant difference in the history of falls between groups after 16 weeks of the exercises programme, this could be due to the number of participants being very small, thereby generating a type II error. Age-related postural alterations that differ according to gender could also be another explanation. Whereas the cervical alterations in men that would be reflected by the block measure of kyphosis are far more obvious, the hyperkyphosis changes in older women mostly occur in the thoracic region. It is conceivable that thoracic hyperkyphosis could raise the risk of falling more than cervically visible hyperkyphosis [32].
The current study found that fear of falling showed no statistically significant interaction between the group and time, but the effect size of the interaction effect was large. This means that the fear of falling was reduced in the exercise group but increased in the control group over time. In other words, the exercise programme can help reduce the fear of falling.
The findings of the current study contrast with the findings of Sinaki et al. [14] reported that a 4-week back extension exercise combined with a gait programme and a spinal orthosis improved the fall-efficacy scores (improved confidence in their ability to perform activities of daily living without falling) in women with osteoporosis-kyphosis.
In addition, a study by Sh et al. [15] reported that a corrective exercise programme decreased the fear of falling in older adults with hyperkyphosis. Sedaghati et al. [33] investigated the effectiveness of the Alexander-based corrective technique on fear of falling, thoracic kyphosis angle, and forward head posture in older adults with idiopathic Parkinson's disease. They demonstrated that the FES-I scores, thoracic kyphosis angle, and head forward posture improved after 8 weeks (3 times/week). The Alexander-based corrective technique is a method to improve posture and movement for chronic musculoskeletal pain. With the Alexander-based corrective technique, patients are taught to alter their positional and tensional patterns and elongation along the spine during activities of daily living and throughout the movement [34, 35].
A possible explanation for the inconsistent results may be the differences in the measuring instruments used for fear of falling (e.g., the visual analogue scale for fear of falling, the modified Fall efficacy scale, the Activities-specific Balance Confidence Scale, and the Fall efficacy scale-International) and the differences between the types of intervention. Additionally, the classification of fear of falling can be divided into 3 groups: 1. Low fear of falling (FES-I score 16-19), 2. Moderate fear of falling (FES-I score 20-27), 3. High fear of falling (FES-I score 28-64). Participants in both groups in the present study had a low fear of falling scores at baseline (mean of FES-I score: 19.33 ± 2.58 for the exercise group and 18.29 ± 2.21 for the control group). Therefore, the lack of improvement in fear of falling could be explained by a floor effect in the FES-I scores. The current study did not find a significant difference in fear of falling score between groups after 16 weeks of the exercises programme; this could be due to the limited numbers of participants, thereby generating a type II error.
Participants for both groups received an educational booklet. The educational booklet for the exercise group consisted of general knowledge of hyperkyphosis and good posture in standing and sitting positions together with a hyperkyphosis-specific exercise programme, whereas the educational booklet for the control group comprised only the general knowledge of hyperkyphosis and good posture in standing and sitting position. Participants in both groups reported consistently positive experiences regarding their satisfaction with the educational booklet, including a good impression, ease of understanding, usefulness, and of benefit in managing their self-care. Similar results were demonstrated by McGregor et al. [36], who explored participants’ points of view regarding the educational booklet after spinal surgery. The authors found that a number of participants commented that the educational booklet that had been given to them was easy to follow, the content was interesting and helpful, and they would recommend it to others. Nonetheless, the current study did not find any negative comments from participants, while participants in McGregor et al.’s [36] study reported a number of negative comments, such as the booklet having deficiencies because it lacked exercise details.
In the current study, participants in both groups displayed high satisfaction with the educational booklet. However, the current study did not compare the satisfaction with the educational booklets between the exercise and the control groups because both groups used different booklets and took part in different study conditions. Therefore, it is not meaningful to compare the two booklets. This is because the booklet type and study condition were confounded. It is important to note that, to the author’s knowledge, this is one of the very first studies to investigate the satisfaction with an educational booklet in older adults with hyperkyphosis.
The findings from this study suggest that subjects who participated in a hyperkyphosis-specific exercise programme had high adherence to the exercise programme (83.3%). There were no serious adverse events reported by participants taking part in the exercise group when performing the exercise. The results of the current study demonstrated that a hyperkyphosis-specific exercise programme is highly adhered to and safe for older adults with thoracic hyperkyphosis. It also included follow-up visits for continuity. Additionally, the participants were contacted by the researcher every week for consultation whilst monitoring their adherence to the study and encouraging subjects to continue their exercises.
The number of limitations of the current study warrants consideration. Firstly, the number of participants was small. The researcher had to stop the recruitment process because of the coronavirus pandemic. Secondly, the findings of this study were obtained from older adults with an active lifestyle. Therefore, the findings of the current study may not be generalised to other populations of older adults with a sedentary lifestyle. Finally, a problem with changed scores and mixed ANOVA is ceiling and floor effects. In the current study, a change score of a history of falls and fear of falling was small because the pretest score is very near the end of the scale, and no treatment effect can change it very much, or it may be small because the effect of treatment is small.
The author's recommendation for future research would be to further examine the effectiveness of the hyperkyphosis-specific exercises on 3D back shape and posture as well as static and dynamic balance in older adults with hyperkyphosis. Additionally, a larger RCT is needed to clarify the effectiveness of the hyperkyphosis-specific exercise programme on the number of falls and the fear of falling in this population. It would also be beneficial for future qualitative studies to use in-depth interviews yielding rich data to understand the experiences of living with hyperkyphosis and participating in a hyperkyphosis-specific programme.
CONCLUSION
In conclusion, the effect of the hyperkyphosis-specific exercise on the history and the fear of falling was not statistically significant after completing 16 weeks of the exercise program, even though the effect sizes were large. This indicates that the exercise programme can help to prevent falls and decrease the fear of falling in older adults with thoracic hyperkyphosis. Furthermore, a large effect size means that there was a probability that significantly improved in the history of falls and the fear of falling would be observed with a larger sample size.
In the present study, older adults with thoracic hyperkyphosis were satisfied with an educational booklet with a positive experience overall the exercises programme (as patients enjoyed the exercises programme, received clear and informative information, and had the confidence to perform the exercises and improved their body posture as well as balance).
The hyperkyphosis-specific exercise programme was delivered by a fully qualified physiotherapist; older adults with hyperkyphosis adhered to (high adherence rate) and safely (no serious adverse events during participated in the study) participated in the exercise intervention. Additionally, the results of the current study support the implementation of a definitive large-scale RCT to clarify the effectiveness of a hyperkyphosis-specific exercise programme in reducing the number of falls and fear of falling within this population.
LIST OF ABBREVIATIONS
| ADLs | = Activities of Daily Living |
| FES-I | = Falls Efficacy Scale -International |
| RCT | = Randomised Controlled Trial |
| SBP | = Schroth Best Practice |
| 3D | = Three-Dimensional |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study protocol was approved by Teesside University, School of Health and Life Sciences, Ethics Committee (study number: 263/18).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures were followed in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Verbal and written informed consent was obtained from all participants before testing.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in the Effect of a hyperkyphosis-specific exercise programme on the history of falls, fear of falling and satisfaction in older people with hyperkyphosis: a pilot studyat DOI:10.5281/zenodo.7945194 or https://doi.org/10.5281/zenodo.7945194, reference number [7945194].
FUNDING
This study was funded by Thammasat University, Thailand.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the participants for participating in the study. This work was supported by the School of Health and Life Sciences, Teesside University, UK.
SUPPLEMENTARY MATERIAL
Supplementary material is available on the publisher's website along with the published article.
APPENDIX A
The educational booklet satisfaction questionnaire
1. What is your general impression of the booklet?
Very Bad Bad Neutral Good Very good
2. The information in the booklet is easy to understand
Strongly Disagree Disagree Neutral Agree Strongly Agree
3. Advice in the booklet is beneficial in managing my self-care.
Strongly Disagree Disagree Neutral Agree Strongly Agree
4. The Photos in the booklet added value
Strongly Disagree Disagree Neutral Agree Strongly Agree
5. I found that the booklet was easy to use
Strongly Disagree Disagree Neutral Agree Strongly Agree
6. All this considered are you satisfied with the educational booklet provided?
Strongly Disagree Disagree Neutral Agree Strongly Agree
7. Will you continue to use it for your self-care management?
Strongly Disagree Disagree Neutral Agree Strongly Agree
8.What is your preferred format of receiving the back care programme?
Electronic or Booklet
9.Any other comments
APPENDIX B
 |
 |
 |
 |
 |
 |
 |
 |
 |
APPENDIX C
| Question | Responses | |
| Exercise group (n=6) | Control group (n=7) | |
| 1. What is your general impression of the booklet? | • 66.7% (4) good • 33.3% (2) very good |
• 71.4% (5) good • 28.6% (2) very good |
| 2. The information in the booklet is easy to understand | • 83.3% (5) agree • 16.7% (1) strongly agree |
• 57.1% (4) agree • 42.9% (3) strongly agree |
| 3. Advice in the booklet is beneficial in managing my self-care | • 16.7% (1) neutral • 66.7% (4) agree • 16.7% (1) strongly agree |
• 42.9% (3) neutral • 42.9% (3) agree • 14.3% (1) strongly agree |
| 4. The Photos in the booklet added value. | • 83.3% (5) agree • 16.7% (1) strongly agree |
• 71.4% (5) agree • 28.6% (2) strongly agree |
| 5. I found that the booklet was easy to use. | • 66.7% (4) agree • 33.3% (2) strongly agree |
• 14.3% (1) neutral • 57.1% (4) agree • 28.6% (2) strongly agree |
| 6. All this considered are you satisfied with the educational booklet provided? | • 66.7% (4) agree • 33.3% (2) strongly agree |
• 71.4% (5) agree • 28.6% (2) strongly agree |
| 7. Will you continue to use it for your self-care management? | • 16.7% (1) neutral • 50.0% (3) agree • 33.3% (2) strongly agree |
• 42.9% (3) neutral • 57.1% (4) agree |
| 8. What is your preferred format for receiving the back care programme? | • 100% (6) preferred the booklet version | • 14.3% (1) preferred the electronic version • 85.7% (6) preferred booklet version |
| 9. Any other comments | • The pictures in the booklet were a little misleading as I was advised to lower my hand to lower my ribs, but this is just a minor observation. • All the movements and exercises were easy to follow and understand how to do them. |
• It would be useful to show which angle you are measuring on the diagram. • Photos are useful. • The booklet is a convenient size to hold (A5), and not too long (20 pages including front and back). It is laid out in an accessible easy-to-follow, easy-to-understand language, large print, graphics, and photos enhance the text while encouraging the reader to follow the booklet and the cute "Thank you " at the end is a nice touch. • I found it easy to understand and follow in the booklet. |

