All published articles of this journal are available on ScienceDirect.

Factors Affecting Stability of the Reverse Total Shoulder Arthroplasty: A Cadaveric Biomechanical Study
Authors Info & Affiliations
Abstract
Background:
The overall objective of this study was to investigate whether a reverse shoulder arthroplasty could provide adequate stability to a shoulder even with extreme soft tissue loss. The specific objectives of this study were: to determine if just the deltoid, conjoined tendon, and triceps are sufficient soft tissues to allow a Reverse Shoulder Arthroplasty (RSA) to provide shoulder stability and to determine the influence of load direction, rotation, shoulder position, and polyethylene thickness on RSA stability in this soft-tissue deficient model.
Methods:
This study utilized six cadaveric shoulders that had all soft tissue removed, with the exception of the deltoid, conjoint tendon, and long head of triceps. A reverse shoulder arthroplasty was then performed (Delta III, DePuy Inc., Warsaw, IN) and an increasing dislocation force was applied perpendicular to the humeral socket centerline until dislocation occurred, or a maximum load of 100 N was reached. This was repeated to measure the effect of four factors: load direction, arm position, polyethylene thickness, and arm rotation on force to dislocation.
Results:
For load direction, there was an increase in force to dislocate an inferior load direction (p=0.01). There was a lower not dislocated percentage and lower survival for a posterior load direction (p=0.02). For arm position, there was a decrease in force for dislocation and lower survival for both abduction and extension arm positions. There was a higher not dislocated percentage for a flexion arm position (p=0.01). For arm rotation, there was a lower not dislocated percentage and lower survival for an external rotation arm position (p=0.03). There was no statistically significant influence of polyethylene thickness (p=0.26).
Conclusion:
The deltoid, conjoined tendon, and triceps are sufficient to stabilize an RSA. Load direction, arm position, and arm rotation were all shown to significantly affect stability. Finally, polyethylene thickness may not affect overall RSA stability in this soft-tissue deficient model.
Level of Evidence:
Basic science study, Biomechanical study.
1. INTRODUCTION
Reverse Shoulder Arthroplasty (RSA) is an effective treatment in providing pain relief and improved function in the arthritic, rotator cuff-deficient shoulder [1-4]. RSA is an increasingly common procedure despite complication rates that remain high [5-10]. In contrast to conventional shoulder arthroplasty, RSA utilizes a semi-constrained design, which provides increased stability despite the loss of most soft tissue stabilizers [4, 11] Despite this, instability remains a significant problem, with published rates ranging from 0-30% [2, 3, 12, 13]. This is particularly concerning as surgical indications for this procedure continue to expand. Factors suggested to be associated with instability include inadequate soft tissue tension, mal-positioning of components, component loosening, pre-operative osseous deformity, abutment of the humeral component against the glenoid, trauma, and revision of a previous arthroplasty [7, 8, 14-18]. However, soft tissue contributions to stability in RSA have not been thoroughly investigated.
Previous biomechanical studies have looked at variables contributing to stability. Henninger et al. have shown that humeral component version and implant thickness did not affect stability, but the centre of rotation lateralization did improve stability in a cadaveric model [19, 20]. Clouthier et al. have shown that increased glenohumeral abduction, a more constrained humeral socket and the use of an inferior-offset glenosphere increased stability of reverse shoulder arthroplasty, but that glenosphere diameter had no effect [15]. While several studies state that the direction of dislocation is exclusively anterior, there is a relative paucity of evidence in the literature indicating the most common direction(s) of dislocation [12, 14].
This study arose out of our observation that a reverse shoulder arthroplasty can provide stability to a shoulder, despite often severe soft tissue loss. Our hypothesis was that even with an extreme amount of soft tissue loss, the inherent stability provided by the reverse shoulder arthroplasty design would be adequate to provide a stable shoulder with only the deltoid, conjoined tendon, and triceps muscles intact. These three muscles were chosen as they are infrequently deficient in our experience and each cross the glenohumeral joint in a direction that remains somewhat perpendicular to the joint and, therefore, provide joint compression throughout most shoulder motions. Therefore, the overall objective of this study was to investigate whether a reverse shoulder arthroplasty could provide adequate stability to a shoulder even with extreme soft tissue loss. The specific objectives of this study were twofold. The first objective was to determine if just the deltoid, conjoined tendon, and triceps are sufficient soft tissues to allow an RSA to provide shoulder stability. The second objective was to determine the influence of load direction, rotation, shoulder position, and polyethylene thickness on the stability of an RSA in this soft-tissue deficient model.
2. MATERIALS AND METHODS
This study utilized six fresh-frozen cadaveric fore-quarters amputated at the mid-forearm level with a mean age of 89 years (range, 79-102 years). Each cadaveric specimen had not undergone any previous surgeries or visible trauma and was verified to be completely intact prior to inclusion in the study. Each scapula was mounted on a rigid frame using a bone clamp placed underneath the scapular spine. The glenohumeral joint capsule, rotator cuff, and scapulohumeral muscles were removed, with the exception of the deltoid, conjoint tendon (coracobrachialis, the short head of biceps), and long head of triceps, which were left intact. These three structures were verified to be completely intact prior to the inclusion of each specimen in the study. These muscles were not actively loaded in this model but instead provided only passive soft tissue constraint. A reverse shoulder arthroplasty was then performed by the senior author (Delta III, DePuy Inc., Warsaw, IN). This utilized a 36 mm glenosphere in neutral inclination and rotation and centered along the glenoid superior-inferior axis and a humeral component in neutral rotation, according to the manufacturer recommendations. The arm was held in each arm position and rotation by an examiner holding at the mid-forearm level with the elbow flexed to 90 degrees and measured using a goniometer.
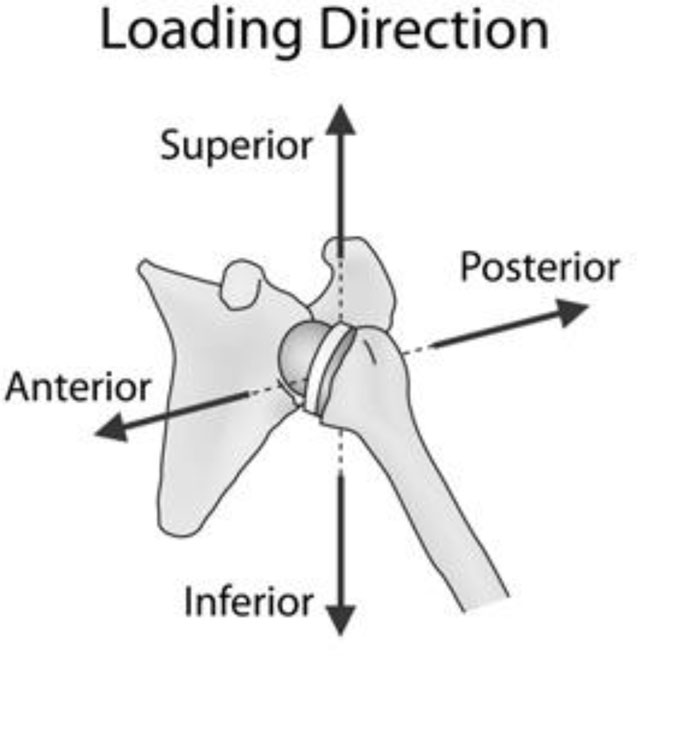
A displacing force was then applied perpendicular to the humeral socket centerline using an Instron MTS machine attached via cables at the epiphysis of the humeral component (Fig. 1). The force was increased until dislocation occurred, or a maximum load of 100 N was reached. A maximum load of 100 N was chosen as loading beyond this value quickly led to instability. Displacements were applied at 100 mm/min. This was repeated to measure the effect of four factors: load direction (anterior, posterior, superior, and inferior), arm position (0 degrees abduction, 60 degrees abduction, 60 degrees flexion, 60 degrees extension), polyethylene thickness (3, 6, 9 mm), and arm rotation (neutral, 20 degrees anteversion, 20 degrees retroversion). A block randomized loading protocol was used.
Outcome measures used as measures of stability included mean force to dislocation in those trials that dislocated (i.e. with a higher value indicating increased stability), as well as the percentage of the specimen that did not dislocate at a maximal dislocation force of 100N (i.e. with a lower value indicating decreased stability). For each trial, five measurements were performed and the average value was reported. Statistical analysis utilized a one-way ANOVA with post-hoc Tukey tests for multiple comparisons (p < 0.05).
3. RESULTS
For load direction, there was an increased force to dislocate an inferior load direction (p=0.01) and a lower percentage not dislocated for a posterior load direction (Fig. 2a) (p=0.02). For arm position, there was a decreased force of dislocation for both an abduction and extension arm position and a higher percentage not dislocated for a flexion arm position (Fig. 2b) (p=0.01). For arm rotation, there was a lower percentage, not dislocated for an external rotation arm position (Fig. 2c) (p=0.03). For polyethylene thickness, there was no statistically significant difference between any parameters (Fig. 2d) (p=0.26).

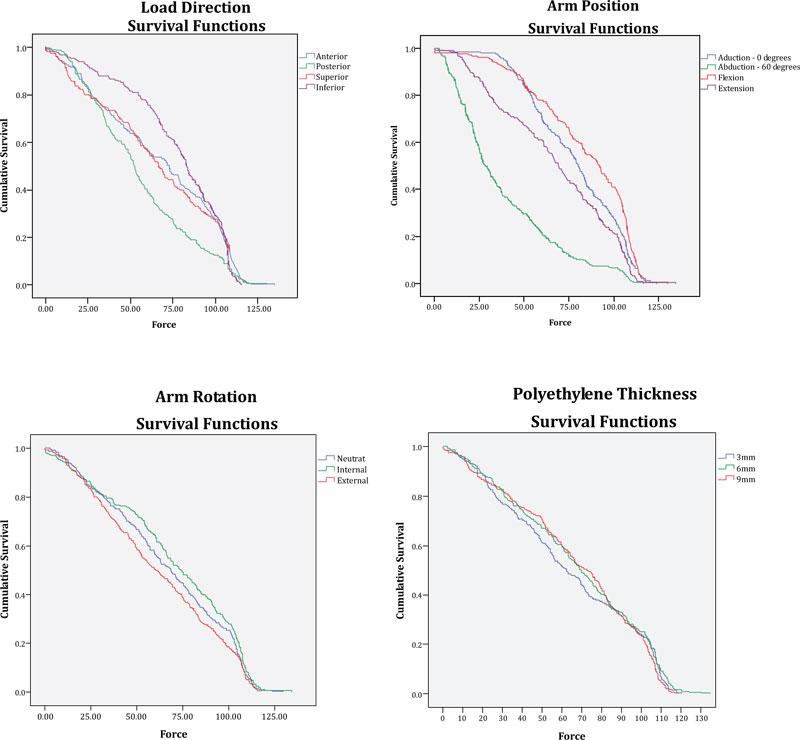
Survival curves are shown for each factor (Fig. 3). For load direction, a posterior load direction had lower survival than all other directions (Fig. 3a) (p=0.03). For arm position, both an abduction and an extension position had lower survival than all other positions (Fig. 3b) (p=0.03). For arm rotation, external rotation had lower survival than internal rotation (p=0.003) but not neutral rotation (p=0.14) (Fig. 3c). For polyethylene thickness, there was no difference in survival between different thicknesses (Fig. 3d) (p=0.71).
4. DISCUSSION
Instability is a common complication of reverse shoulder arthroplasty and although several studies have investigated the factors upon which stability is dependent, these have yet to be completely defined [7, 12, 14-18]. This study has shown that an RSA can be stable despite extreme soft tissue loss. Specifically, this study has shown that the deltoid, conjoined tendon, and triceps are sufficient in stabilizing the RSA joint from dislocating forces. These three muscles were
chosen for several reasons. First, they are infrequently deficient, in our experience, shoulders that undergo reverse shoulder arthroplasty often have quite severe soft tissue deficiency. However, a deltoid deficiency is a contraindication to reverse shoulder arthroplasty, as a functioning deltoid is required to provide movement [4]. The conjoined tendon and triceps have never been found to be deficient in our experience. Second, each of these muscles crosses the glenohumeral joint in a direction that remains somewhat perpendicular to the joint and therefore, provides joint compression throughout most shoulder motions (Fig. 4). The authors also recognize that while it is uncommon for this amount of soft tissue loss to occur, it is our opinion that this information is valuable, in that it indicates that other soft tissues, specifically those that do not directly provide a compressive force across the joint, maybe expendable. This indicates that other muscles may not be required if they are deficient or can be sacrificed if necessary to use for other indications such as associated tendon transfers. The fact that stability can still be achieved with such extreme soft tissue loss may not be surprising given that an RSA utilizes a constrained design and specifically is meant to account for soft tissue loss. However, this is the first biomechanical study to suggest that only such a minimal amount of tissue is sufficient to stabilize an RSA.
The RSA shoulder was most stable when an inferiorly directed force was applied. This is perhaps not surprising, as this mode of dislocation has not been commonly described clinically. In contrast, dislocation occurred most frequently and at the lowest mean force, when a posteriorly directed force was applied. This is in contrast to several clinical studies, which have demonstrated anterior instability occurring most commonly [12]. Arm position had a significant impact on the

propensity for the RSA shoulder to dislocate with shoulder flexion being most stable and abduction, followed by extension, resulting in dislocation at a lower mean displacing force. This is in contrast to most clinical experience and a previous study, which has shown that shoulder abduction is a more stable position [15]. However, a more recent meta-analysis of RSA instability from Bohsali et al. 2017, suggests that both abduction and extension are at-risk positions for a post RSA shoulder [21]. In fact, it is often suggested that RSA shoulders at risk for instability can be immobilized in abduction. This discrepancy, with clinical experience and the study by Clouthier et al. 2013 [15], may be explained by the lack of active muscle loading in this model. Active muscle loading, to achieve an abducted position, would increase the compressive force across the joint, consequently leading to increased stability. It is also possible that the diameter of the glenosphere had an impact on the results. While Clouthier et al. reported that the diameter of the glenosphere has no effect on stability, the Bohsali et al. meta-analysis claims the opposite. Since there is contention into the overall effect of the glenosphere’s diameter, it is safest to list this as a possible contributing factor. Arm rotation was found to affect stability, with a position of external rotation being least stable. This arm rotation could lead to a propensity for anterior instability, which is clinically relevant. Polyethylene thickness was not found to have any effect on shoulder stability. This is a bit surprising given that an increased polyethylene thickness should increase overall tension, thereby improving stability. However, previous studies have also found no influence of polyethylene thickness on stability [20].
This study has several strengths. This was the first study to investigate the effects of soft tissue loss, to the point of the most basic musculature, on the stability of reverse shoulder arthroplasty. We utilized a cadaveric model with a physiologically applied dislocation force. A cadaveric model allows for differences or variabilities among specimens, however, these were minimized as each cadaveric specimen had not undergone any previous surgeries or trauma and was verified to be completely intact prior to inclusion in the study. Furthermore, the soft tissue structures of interest, the deltoid, conjoint tendon (coracobrachialis, short head of biceps), and long head of triceps were verified to be completely intact prior to the inclusion of each specimen in the study. However, there are some limitations associated with this study. Although this study uses a cadaveric specimen, which allows the inclusion of the effect of soft tissue bulk, active muscle loading is still not accounted for and likely influences stability as well. However, we believe the findings of this study are beneficial as they provide information related to inherent stability in reverse shoulder arthroplasty based on a worst-case scenario of only static soft tissue tensions. Moreover, this study investigated the combined effect on RSA stability of the three soft tissue structures of interest. Therefore, this study cannot make any comments regarding the individual contribution of each of these structures. Additionally, these experiments utilized a Grammont-style implant design and it is possible that different results could be found with other implant designs. Future directions could include investigation of other implant designs, as well as investigation of the individual contributions of each of the deltoid, conjoined tendon, and triceps to reverse shoulder arthroplasty stability.
CONCLUSION
In conclusion, this study has shown that RSA stability can be achieved despite extreme soft tissue loss. The deltoid, conjoined tendon, and triceps are sufficient to stabilize the RSA. Furthermore, certain loading directions, arm positions, and arm rotations lead to an increased risk of instability. Finally, polyethylene thickness may not affect overall RSA stability in this soft tissue loss model.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

