All published articles of this journal are available on ScienceDirect.

Early Failures of Total Knee Patients with Nickel Allergies Secondary to Carbon Fiber Debris
Authors Info & Affiliations
Abstract
Aim:
Currently, there are not many studies on the long-term outcomes of the specific implants used in patients with metal hypersensitivities. The purpose of this study is to report a significant number of TKA revision failures with the CFR-PEEK prosthetic knee implant with an anatomic hinge.
Background:
Patients can experience multiple issues following a primary Total Knee Arthroplasty (TKA). A growing body of research is finding a correlation between primary TKA failure and metal hypersensitivity, most commonly with nickel and cobalt. Because of this, knee prosthetics are being made from hypoallergenic metals, such as zirconium nitride (ZrN), to minimize the number of failures due to metal allergy. Given the relatively new development of the hypoallergenic prostheses, there is sparse data about their overall success.
Objective:
The purpose of this study is to report a significant number of TKA revision failures with the CFR-PEEK prosthetic knee implant with an anatomic hinge.
Methods:
In this study, we analyzed the sequelae of 84 patients between May 2015 to June 2020 who received a total knee revision due to a failed primary TKA with metal hypersensitivity. These patients were revised with the rotating anatomic hinge knee system, which consisted of Carbon Fiber Reinforced Poly-Ether-Ether-Ketone (CFR-PEEK implant) coated with a ZrN, Zirconium, and Chrome Nitride multi-layer surface coating with 30% polyacrylonitrile fiber content. The patients requiring an additional revision operation presented with increasing pain that showed evidence of osteolysis on plain radiographs, CT imaging, positive indium labeled WBC scans and increased uptake on bone scan. Intraoperatively, an open incisional biopsy of the surgical bed was obtained, followed by radical debridement and implantation of porex knee prosthesis. In addition, intraoperative findings included black debris that grossly stained the surrounding synovial tissue black, indicative of wear and debris from carbon fiber bearings and the anatomic hinge. Histology of the intraoperative biopsy showed the accumulation of black debris in the histiocyte, fibrosis, and perivascular cuffing of lymphocytes and multinucleated giant cells stained with black debris.
Results:
Of the 84 patients, 22 failed, requiring an additional revision procedure, equating to a 26 percent failure rate of the CFR-PEEK implant, averaging 25 months to failure.
Conclusion:
This study was meant to report the extremely high failure rate of the anatomic hinge secondary to carbon fiber debris. Perhaps carbon fiber-laden implants are not as good an option for total knee revision prosthesis because of the high failure rate compared to those with polyethylene in their hinge mechanism.
1. INTRODUCTION
As the number of annual primary total knee arthroplasty (TKA) procedures grows, so will the number of TKA revision cases [1]. Current data suggest an overall patient satisfaction of 80-85% with their primary TKA, and although this leaves roughly 1 in 5 patients dissatisfied with their primary, only 5% of all primary TKAs will require a revision for failure [2, 3]. Some attribute the discrepancy between patient disappointment with primary TKA and revision rate to unreal patient expectations preoperatively, while others report inadequate post-operative management, leading to suboptimization of the implant function [4, 5]. Regardless of the etiology of primary TKA dissatisfaction rates, current guidelines exist to improve long term patient outcomes post-operatively [6]. For example, the American Association of Hip and Knee Surgeons (AAHKS) recommends annual clinical and radiographic follow-up on asymptomatic patients, assuming patients with problematic symptoms will present earlier [6]. Optimization and patient satisfaction with the primary TKA is vitally important because TKA revision procedures yield less than ideal results [7]. In comparison to a primary TKA, the survivorship of TKA revisions is as low as 60%, in addition to lower satisfaction rates and worse functional scores [7]. Although patient dissatisfaction alone is not an indication for TKA revision, indications for such revision can be classified based on acute and chronic factors [2]. Acute factors include infection, fracture, and traumatic implant failure, whereas chronic factors include indolent infection, osteolysis, significant pain, and late component loosening secondary to wear and debris [2]. Infections occur on average in 1.9% of primary knees, with that figure jumping up to 10% or more for revision TKA [19]. Incidence rates of osteolysis have been reported to be up to 21% for total knees post revision [21]. In addition to the burden of the failed TKA on patients, TKA revisions cause significant financial strain on the healthcare system [6]. The average cost of a TKA revision is 40% greater than the primary and more complex revisions cost even more [6].
There is a growing body of literature correlating patient metal hypersensitivity and problems associated with primary TKAs [8, 9]. It is estimated that 10-15% of the population has metal allergies, and of that subpopulation, nickel and cobalt are the most common sensitizers [8]. In the patient with a metal hypersensitivity, problems associated with the primary TKA appear to present similar to a periprosthetic joint infection (PJI) [10]. The problems include joint erythema, effusion, and pain with movement [10]. However, these patients will be aseptic, shown by negative joint aspirate or blood sample culture and sensitivity [8]. Opportunely, Lymphocyte Transformation Testing (LTT), an in vitro test that measures the activated T-lymphocyte response to various metal allergens, serves as a valuable resource to accurately identify patients with metal allergies [11]. As a result of the increased incidence of metal allergies attributing to implant failure, medical device companies are starting to manufacture implants tailored to the metal allergic population in order to avoid the necessity of revision based on metal hypersensitivity [12]. In a study by Ajwani and Charalambous (2016), they identified 15 hypoallergenic TKA systems from 13 different manufacturers. 10 of the 15 hypoallergenic TKA systems are made from cobalt chrome with a hypoallergenic coating and the other 5 are made with a combination of titanium and zirconium [20]. In order to make 10 cobalt chrome hypoallergenic systems, since cobalt is a common sensitizer, both articulating and non-articulating surfaces are superficially coated with zirconium nitride or titanium nitride with 30% polyacrylonitrile fiber content [20]. Of the 15 hypoallergenic TKA systems, 4 include a hinge component [20]. Table 1 highlights the hypoallergenic TKA systems with hinge components and the composition of the femoral and tibial components. In addition, only the CFR-PEEK implant is manufactured with carbon fiber.
Currently, there are not many studies on the long-term outcomes of the specific implants used in patients with metal hypersensitivities. The purpose of this study is to report a significant number of TKA revision failures with the CFR-PEEK prosthetic knee implant with an anatomic hinge.
2. METHODS
2.1. Study Design and Participants
This study was retrospective and case-controlled. All patients who underwent a primary TKA revision with the CFR-PEEK implant between May 2015 and June 2020 due to metal allergies were included in the study population. All patients in the study presented with nickel allergies. One of these patients also had mild reactions to aluminum, molybdenum, zirconium, and iron. Any patient presenting with problems related to the CFR-PEEK implant underwent subsequent lab testing and imaging. Patients with a clinical indication for additional revision were considered to have failed the CFR-PEEK implant. This study evaluated multiple variables. These included the overall failure rate with the CFR-PEEK implant, the reason for failure, time to failure of each implant, gender distribution, and incidence of osteolysis in cases that failed.
2.2. Description of Experiment, Treatment or Surgery
Diagnosis: Patients with the CFR-PEEK implant presented to the clinic on routine post-operative follow-up. All patients, symptomatic or not, received a thorough physical exam and x-ray imaging of the revised joint. The physical exam consisted of visualization, range of motion (ROM), and checking for an effusion testing for any abnormal ranges of motion or prosthetic defects. For those with increasing levels of pain or acute impairment in joint function, further testing with x-ray (XR), indium labeled white blood cell (WBC) scan, triple-phase bone scan, and CT imaging were ordered to evaluate for etiology. Indications for an additional revision operation included significant pain, osteolysis, component loosening, MDI, or infection. Furthermore, the intraoperative biopsy and culture and sensitivity helped guide the final diagnosis for the etiology of failure.
Surgical Procedure: Patients got an intraoperative open incisional biopsy of the knee followed by radical debridement, including debridement of skin, subcutaneous tissue, deep tendon, muscle belly, periosteum, bone, and resection of the capsule with mobilization of the popliteal vessels and sciatic nerve, followed by definitive reconstruction with a hinge.
3. RESULTS
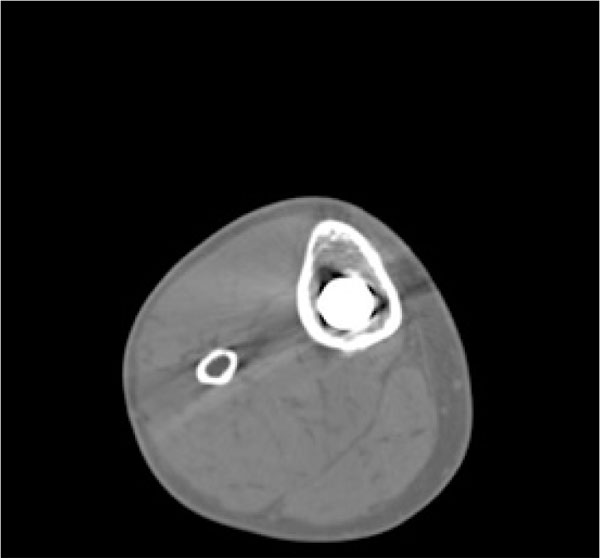
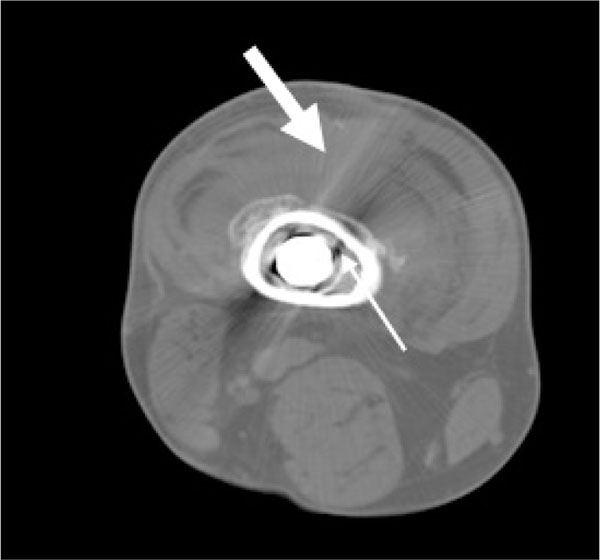
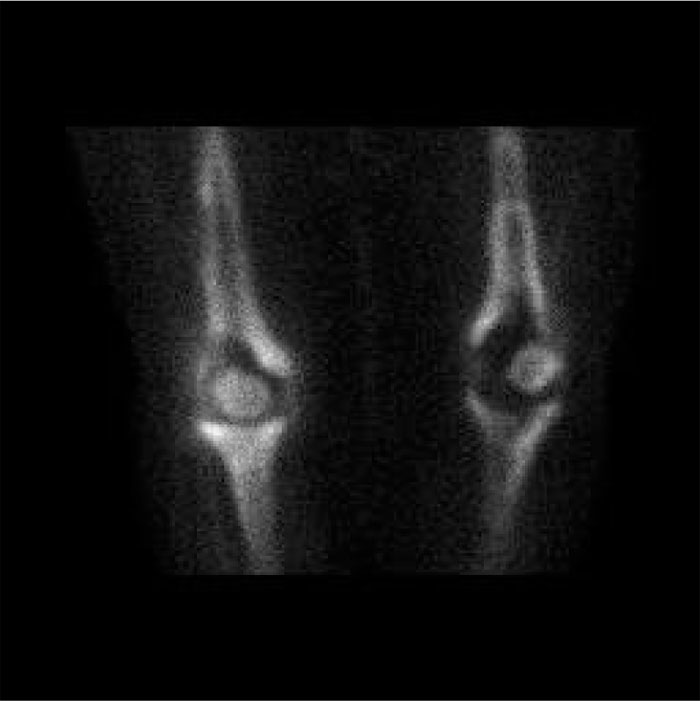
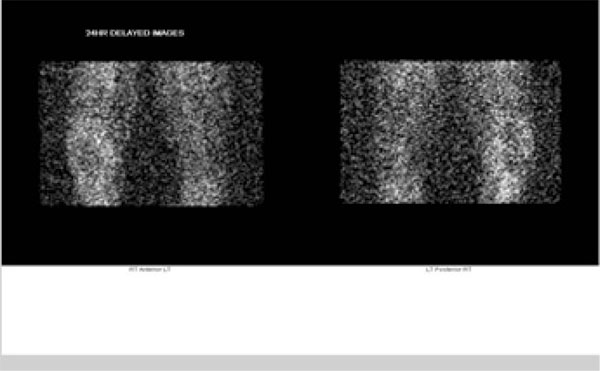
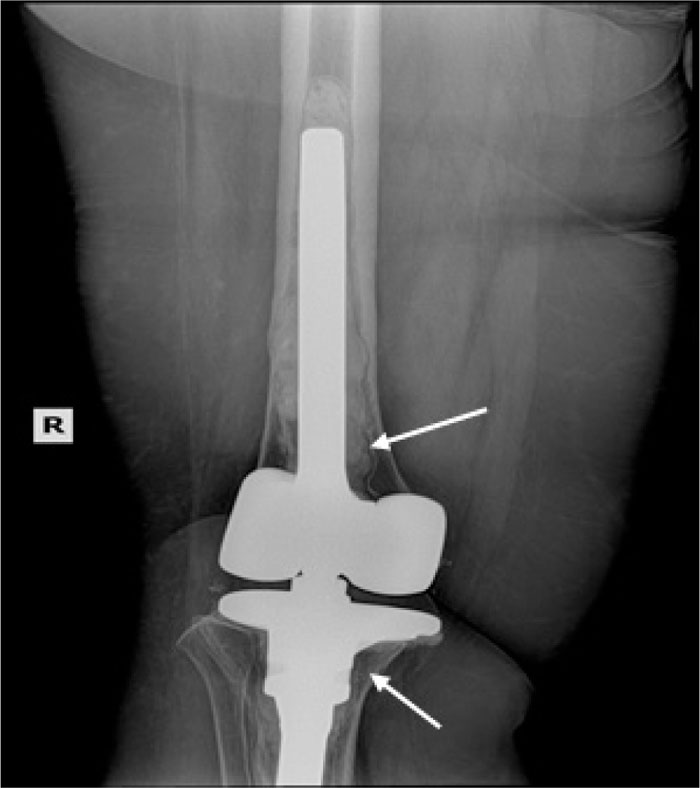
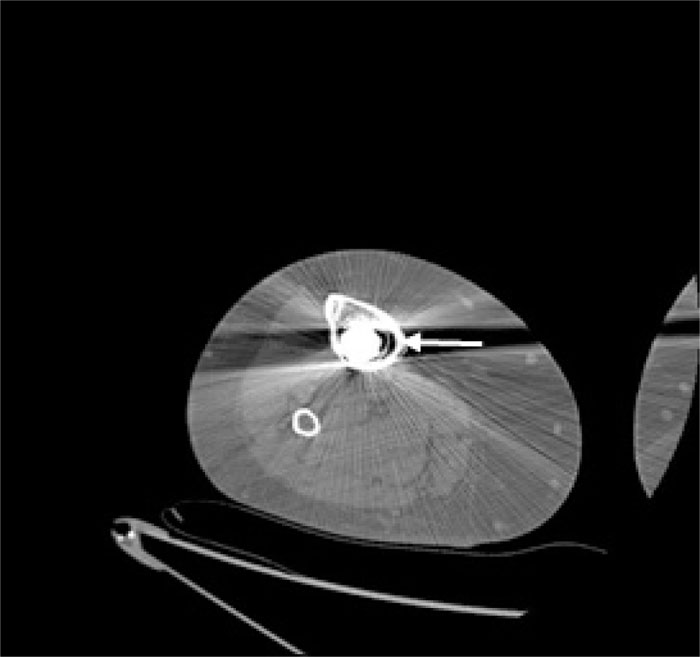
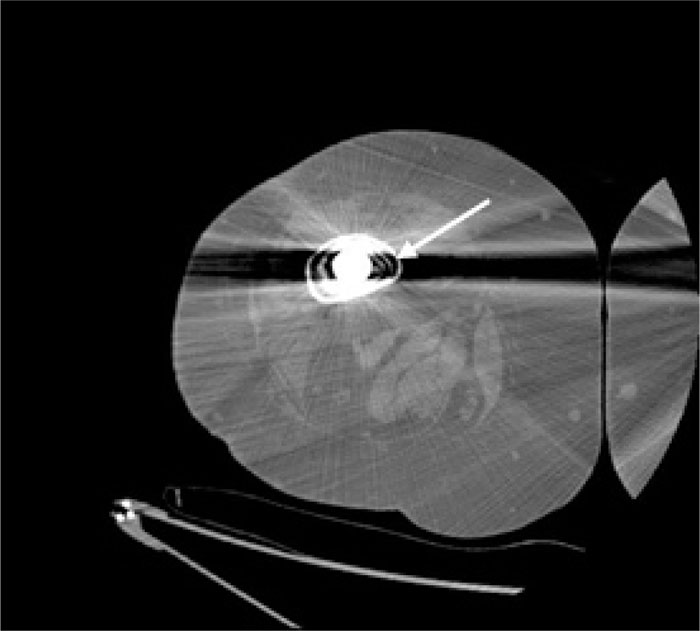
In the patients with failed CFR-PEEK implants, XR and CT showed evidence of osteolysis at bone adjacent to the implant and cement and often, heterotopic bone in the metaphyseal areas. Figs. (1 and 5) showed pre-operative x-rays for patients A and B, respectively. Figs. (2 and 6) show CTs for patients A and B, respectively. The bone scan shows a focal increased blood flow activity on the early and late blood pool phases of the surrounding synovium and increased uptake around the prostheses on the delayed bone phase (Fig. 3). Additionally, the WBC scan showed some increased uptake in the areas adjacent to the implant (Fig. 4). Intraoperative findings included a gross black staining, reactive hypertrophic synovium, and surrounding periosteal tissue. If there was evidence of component loosening in the tissue surrounding the implant, the bone was also stained black (Fig. 7). The black debris pigmented the synovial tissue and periosteal tissue. Pathology slides of the open biopsy of synovial and periosteal tissues were stained with hematoxylin and eosin. These demonstrated soft tissue fibrosis and mild non-specific chronic inflammation was negative for significant acute inflammation, except for the three patients with infection. The black debris was seen within histiocytes and giant cells, and there was lymphocytic perivascular cuffing in the soft tissue (Fig. 8). Figs. (9 and 10) show post-operative fixation with a hypoallergenic revision prosthetic for patients A and B, respectively.
| Manufacturer | TKA System | Femoral Component | Tibial Component |
|---|---|---|---|
| B. Braun & Aesculap | Enduro | ZrN, Zirconium, CrN multi-layer alloy reinforced with Carbon Fiber Poly Ether Ether Ketone (CFR-PEEK) | ZrN, Zirconium, CrN multi-layer alloy reinforced with Carbon Fiber Poly Ether Ether Ketone (CFR-PEEK) |
| Smith and Nephew | Legion HK | Oxinium oxidized Zirconium alloy | Titanium alloy |
| Stanmore | Smiles-Hinged Prosthesis | CoCr alloy with Titanium Nitride coating | CoCr alloy with Titanium Nitride coating |
| Waldemar-Link | Porex | CoCrMo alloy with Titanium Niobium Nitride coating | CoCrMo alloy with Titanium Niobium Nitride coating |
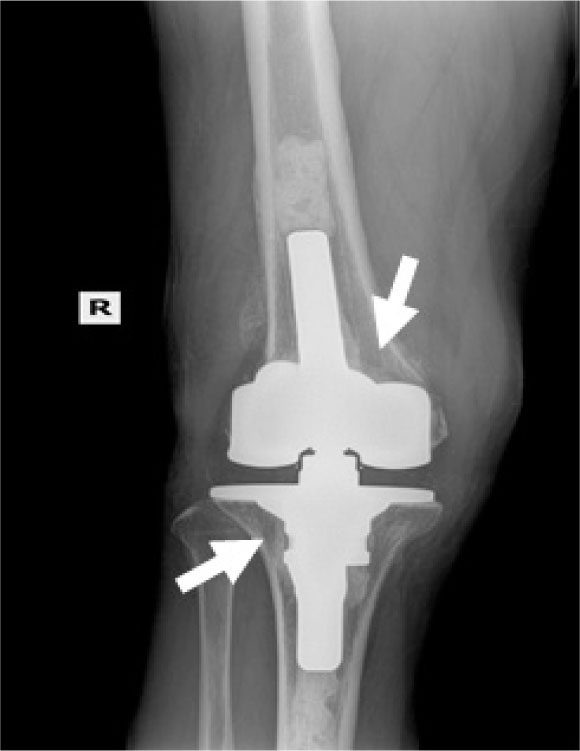

Pre-operative Staging of Patient A

Pre-operative Staging of Patient B.
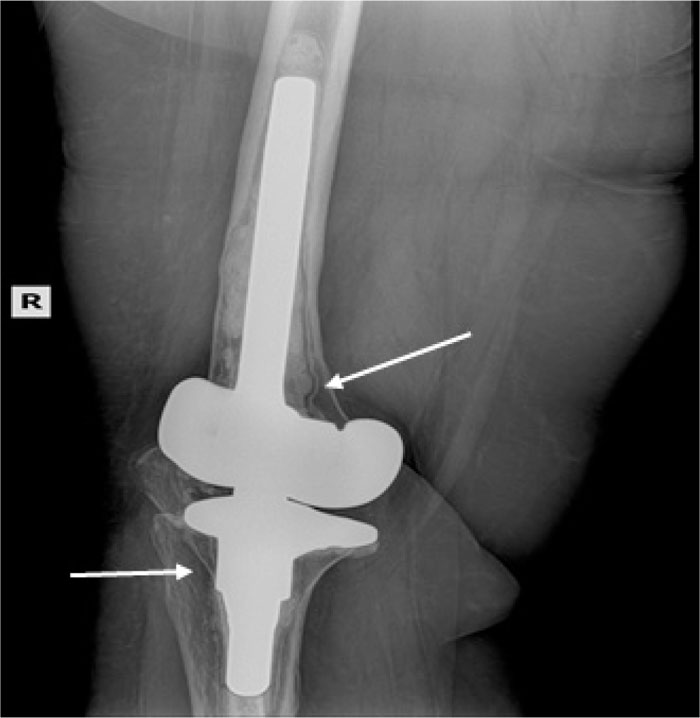
Note: WBC and Tri-Phase Bone scan not shown for patient B


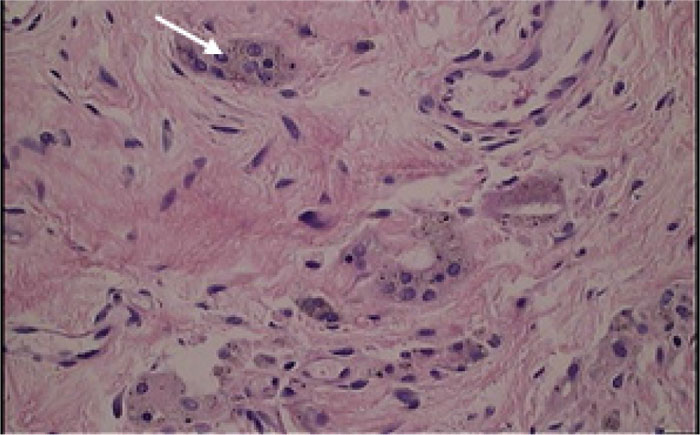
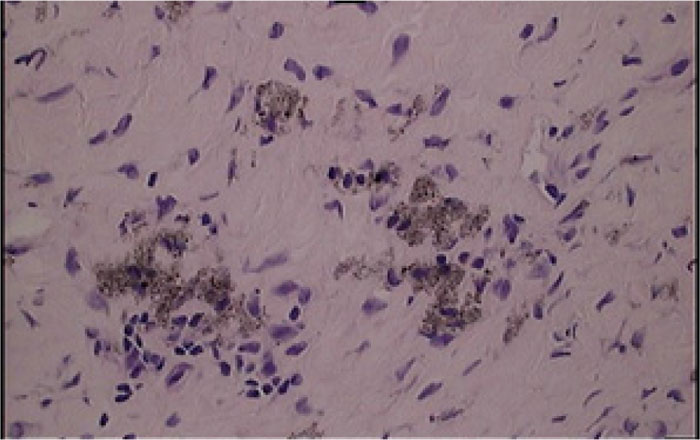
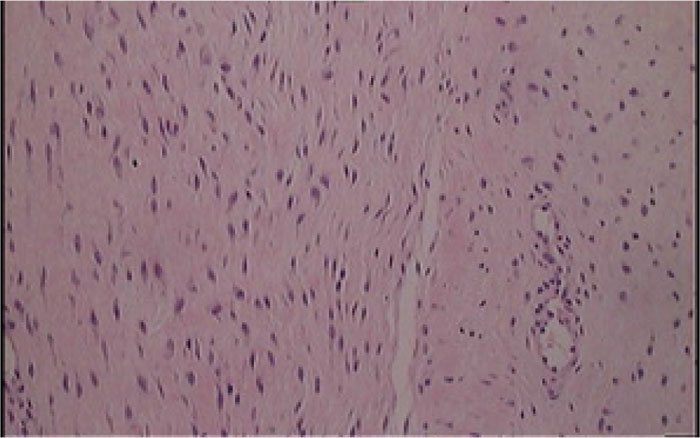
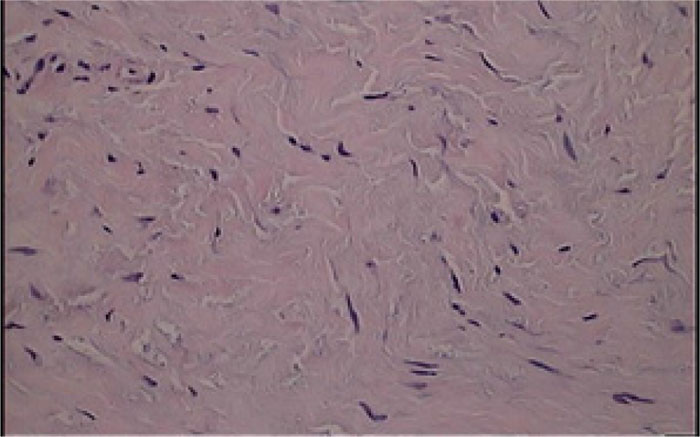
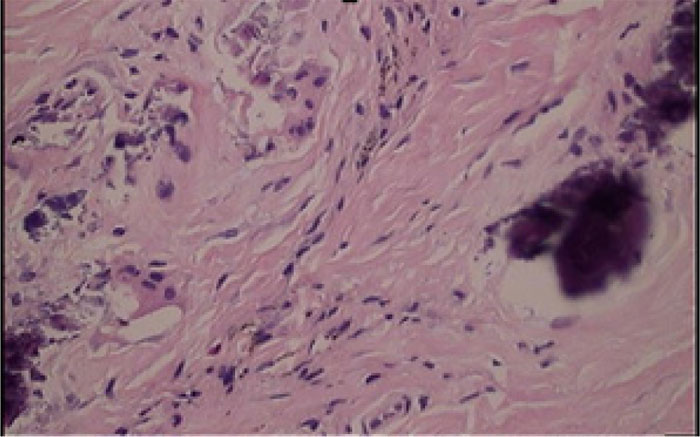
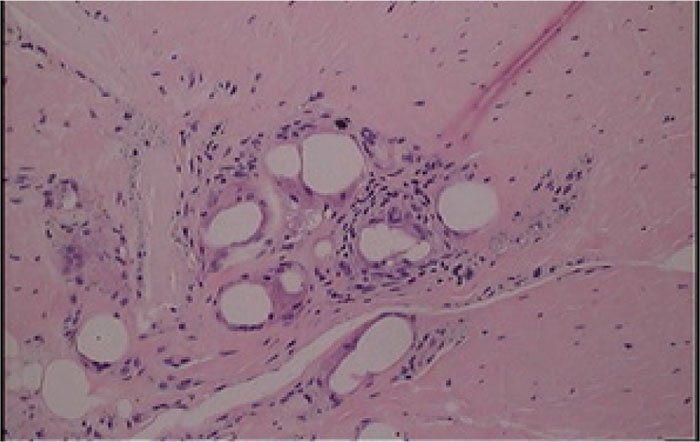
*Tissues stained with hematoxylin and eosin




The total number of patients with a CFR-PEEK implant from May 2015 to June 2020 was 84. The patient population age ranged from 41 years to 80 years, with an average age of 61 years at the time of revision. The average time to implant failure was 25 months, with a range between 5 and 65 months. Of the 84 patients, 22 returned to us as failures, requiring an additional revision procedure, equating to a 26% failure rate of the CFR-PEEK implant. Using the primary knee revision rate in Khan et al., which quoted a 5% rate of failure, Fisher's exact test of significance comparing the CFR-PEEK failure rate and the control was performed and yielded p<0.0001. 19 of the 22 failed implants had evidence of osteolysis on plain XR and CT imaging. This, compared to a previously published osteolysis rate of 14.7% in a population of 68 patients with total knee revisions, was used for statistical analysis [22]. A Fisher's exact test of significance comparing the rate of osteolysis in our cohort versus 14.7% from Griffin et al. is 0.2994. Among the 19 implants with osteolysis, 7 had isolated femoral osteolysis and 12 had combined femoral and tibial osteolysis. Of the 22 failed implants, 19 patients were female and 3 were male. Comparing the gender distribution of the number of failed CFR-PEEK implants to the number of non-failed CFR-PEEK implants, Fisher's exact test of significance is 0.1615. Three of the 22 patients had an infection at the time of revision, as documented by histology, culture, and sensitivity. One of these patients required amputation for recurrent infection. Additionally, one of the patients was revised at another center and histology was not available to us.
4. DISCUSSION
The failure rate of the CFR-PEEK implant in patients with revision TKAs is almost 20 times this number, with a p-value of <0.0001 [1-3]. This statistical significance is alarming considering the average time to failure of 25 months with the CFR-PEEK implant, given that the average lifetime of a knee implant is between 10-15 years with an annual 1% failure rate [2, 3]. During data analysis, it was also noted that the time to failure became progressively shorter as time continued after revision with another CFR-PEEK implant. This may be from the sensitivity of the patient to the CFR-PEEK, and as a result, we were quicker to recommend additional revision. However, it is also possible that the quality of the implant itself may have worsened with time. Though on a smaller scale than our study, biotriboligic studies of the CFR-PEEK implant acknowledged that histological examination revealed black wear particles and grey synovium, coupled with an elevated inflammatory response, when subjected to in vitro wear simulation using a four-station servo-hydraulic knee-wear simulator [25]. Additionally, histology taken from patients with CFR-PEEK implants has demonstrated an inflammatory pattern and hypervascularity, revealing small black particles with sharp edges, larger black particles identified as carbon, and colorless grains [26]. The osteolysis rates in our population are similar to the rates seen in other published data on total knee revisions given the p-value being greater than 0.01. This shows that our particular cohort who presented with metal allergies were not predisposed to osteolysis more than other published cohorts. Although the incidence of osteolysis is similar to other published data, our average time to failure was much shorter [23]. The gender distribution of failed implants skewed towards females. When compared to the overall gender distribution of CFR-PEEK cases, the p-value is statistically insignificant. This means that the failures of the CFR-PEEK cases are following the same gender-specific distribution as the prevalence of metal allergy necessitating a hypoallergenic implant (the total number of CFR-PEEK cases). This is in concordance with previous literature showing that implant failure due to metal allergy is female predominant [8, 13]. However, the CFR-PEEK implant was made to be hypoallergenic. It is unlikely the symptoms are from metal hypersensitivity, but due to the wear and debris of the CFR-PEEK bearings and bushings of the implant.
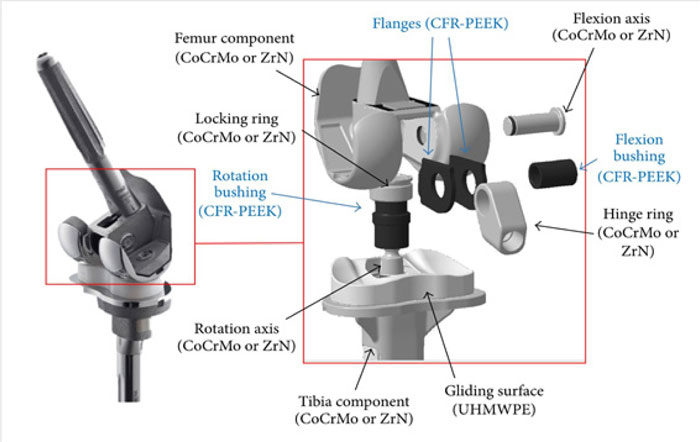
The patients present with problems related to their CFR-PEEK revision implant in a variety of ways. Some patients presented with complications like erythema and edema, mimicking infection, while others presented with impaired function, indicative of joint component loosening. Most of the patients in our cohort presented with MDI. All patients requiring revision reported significant pain at rest. Furthermore, the XR, CT imaging, triple-phase bone scans, and indium labeled WBC scans all showed evidence of osteolysis, component loosening, and inflammation in the tissues adjacent to the implant. Current literature has shown pain, inflammation, and component loosening as common reasons for implant failure [13-15]. The intraoperative findings of black debris in the tissue, from degraded carbon fiber of the CFR-PEEK implant bearing system, have also been reported in previous literature [16]. The CFR-PEEK design is included in Figure 11 for reference [27]. The carbon fiber debris of the implant has been found to lead to the component loosening and inflammation, correlating to the issues with joint function and pain/swelling experienced by the patients [1, 16]. Three cases presented with infection, however, in the researchers opinion, it is believed that bacteremia paired increased vascularity that predisposed these patients.
Although this study reports a clear clinical significance related to the abnormally high incidence of CFR-PEEK failures, it has limitations. Firstly, there is a potential for prevalence bias [17]. Although post-operative follow-up was the same for all patients, we were not aware of the problems with the implant early on. Patients with pain or swelling were treated conservatively instead of with additional revision. It was not until years into using the CFR-PEEK implant, when the first revision was done, where the carbon fiber debris was apparent intraoperatively. As a result, the failure rate may be higher than found because more symptomatic patients who received the implant earlier on were not revised. Secondly, this study may have an attrition bias [18]. Some patients who received the implant earlier stopped attending their annual follow-ups, so if their implants also started to fail, but they did not show up, this would change the failure rate. Thirdly, three of the patients who failed with the CFR-PEEK implant also experienced a patella avulsion or problems with the patella tracking mechanism. It is unknown if the patella issues are due to the implant or not. Fourthly, three of our patients presented with a PJI, in addition to the aforementioned symptoms associated with the CFR-PEEK.
CONCLUSION
This study is meant to report the extremely high failure rate of the CFR-PEEK implant (26%), therefore physicians and patients are aware of its potential sequelae. The use of a hypoallergenic implant in patients with metal allergies is important to help patients needing a revision TKA experience the best quality of life. However, the CFR-PEEK implant, although hypoallergenic, is failing at a higher rate than reported with other implants, in a shorter amount of time.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The Ethics Committee or institutional review board (IRB) of Medical City Plano approved this study with the approval No. 373.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
All patients participated on a voluntary basis and gave their informed consent.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
All other authors do not have conflicts of interest to disclose.
ACKNOWLEDGEMENTS
Declared none.

