All published articles of this journal are available on ScienceDirect.

Femoral Component Rotation in Patellofemoral Joint Replacement: A Study Protocol for a Prospective Observational Study
Authors Info & Affiliations
Abstract
Patellofemoral joint replacement is a successful treatment option for isolated patellofemoral osteoarthritis. The short and mid-term outcomes are related to malposition and unexplained pain. Whether external rotation of the femoral component in isolated patellofemoral joint replacement is required is unclear. The primary aim of this study is to determine the CT-measured femoral component rotation of patellofemoral joint replacement relative to the transepicondylar axis. The secondary aim is to correlate the CT-measured femoral component rotation with the clinical outcomes at 1-year follow-up as assessed with the KOOS questionnaire.
We designed a prospective observational study with medical research ethics committee and institutional review board approval. A total of 40 patients who will be treated with patellofemoral joint replacement for isolated patellofemoral osteoarthritis will be included. Intra-operatively, rotation of the femoral component will be assessed using anatomical landmarks including the epicondylar axis, Whiteside’s line, and lower leg axis. The aim is to insert the femoral component between 3 and 6 degrees external rotation relative to the transepicondylar axis. Two experienced musculoskeletal radiologists will measure the angle between the transepicondylar axis and the femoral component, two to three days after surgery. The primary outcome is the CT-based femoral component rotation of the prosthesis relative to the transepicondylar axis. The secondary outcome is the patient reported KOOS questionnaire at 1-year follow-up.
Successful completion of this study will provide data on the actual amount of femoral component rotation in patellofemoral joint replacement, and its relationship with clinical results. (Netherlands Trial Register NTR4175).
INTRODUCTION
Patellofemoral joint replacement is a successful treatment option for isolated patellofemoral osteoarthritis. The short and mid-term outcomes are related to malposition and unexplained pain [1, 2]. In recent years improvements in prosthetic design have resulted in a more reproducible surgical technique, however, certain aspects of optimal placement remain unclear.
In total knee replacement, external rotation of the femoral component helps to control the flexion and extension gap [3]. Furthermore, external rotation facilitates patellofemoral tracking. Whether external rotation of the femoral component in isolated patellofemoral joint replacement is required is unclear [4]. Only one previous retrospective case-series related the amount of femoral component rotation to clinical results, and reported more patellofemoral complications with internal rotation of the femoral component [5]. Surgical experience suggests that internal rotation probably results in lateral overstuffing, while too much external rotation may lead to patellofemoral instability or dislocation. Ackroyd and Chir recommended between 3 and 6 degrees of external rotation relative to the epicondylar axis [6]. However, the exact amount of external rotation is difficult to assess during surgery. Erosion of the trochlea makes visual orientation using Whiteside’s line unreliable. Although rotational guidance may be obtained from the epicondyles or the posterior femoral condyles, both require an extensive surgical exposure. Some surgeons advocate the use of the lower leg axis [7, 8].
At present, no studies have been performed that demonstrate the actual amount of rotation achieved with patellofemoral prosthetic designs. Considering the above stated importance of avoiding malposition (and more specific: internal rotation), further study is needed.
We hypothesize that with the technique described by Clark et al. [8] the CT-based (actual) femoral component rotation is 3 to 6 degrees external relative to the transepicondylar axis, and that the short-term clinical outcome of patello-femoral joint replacement is related to the actual amount of femoral component rotation.
Therefore the primary objective is to determine the CT-based femoral component rotation of patellofemoral joint replacement relative to the transepicondylar axis. The secondary objective is to correlate the CT-based femoral component rotation of the patellofemoral joint replacement with the clinical outcomes at 1-year follow-up as assessed with the patient reported KOOS questionnaire (Knee injury and Osteoarthritis Outcome Score) [9].
METHODS
Study Design
Single-center, prospective, consecutive case series, invasive observational, without intervention.
Study Population
All mentally competent adult male and female patients who will be treated with patellofemoral joint replacement for isolated patellofemoral osteoarthritis will be considered for inclusion.
In order to be eligible to participate in this study, a subject must meet all of the following criteria:
(1) Isolated patellofemoral osteoarthritis;
(2) Informed consent for the surgical procedure;
(3) Signed informed consent for the study.
A potential subject who meets any of the following criteria will be excluded from participation in this study:
(1) Contra-indication for joint replacement surgery in general (pregnancy, active infection, severe cardiac and respiratory comorbidities);
(2) Previous distal femoral fracture resulting in an altered anatomy.
Sample Size Calculation
Calculation of the required sample size for the primary analysis is based on the assumption that the optimal rotation is between 3 and 6 degrees of external rotation relative to the epicondylar axis [6]. If 90% of patients will have optimal rotation with the lower limit of the 95% confidence interval of the proportion set at 75%, a total sample size of 40 will be required.
Study Parameters
The primary outcome measure is the CT-based femoral component rotation expressed in degrees of rotation relative to the transepicondylar axis (where a positive value denotes external rotation). Secondary outcome measures are the clinical outcomes at 1-year postoperatively as assessed with the patient reported KOOS questionnaire (Knee injury and Osteoarthritis Outcome Score) [9].
Study Procedures
After informed consent for the surgical procedure, patients will be asked to complete the KOOS questionnaire. All patellofemoral joint replacements will be performed by the same experienced orthopaedic surgeon (40 procedures per year), and according to the manufacturer’s instructions. During surgery, photographs will document the degree and extent of degenerative changes in the patellofemoral joint. The Zimmer Gender-Solutions Patello-Femoral prosthesis (Zimmer, Warsaw, Indiana) will be used in all patients. Intra-operatively, rotation will be assessed using the lower leg axis (which is perpendicular to the transepicondylar axis). The aim is to insert the femoral component between 3 and 6 degrees external rotation relative to the transepicondylar axis using the technique described by Clark et al. [8]. At the end of the procedure, the skin will be closed with non-metal sutures.
One to three days after surgery (during the hospital stay) all patients will have a CT assessment of component rotation. Low-dose CT with metal suppression protocol will be used in all cases. The patient will be placed supine on the CT scanning table with the involved extremity in full extension and adjusted to allow the scans to be perpendicular to the mechanical axis of the knee. The Effective Dose (ED) based on previous clinical CT studies of patellofemoral joint replacement at our institution is approximately 0.12 mSv (Dose Length Product (DLP) in 2 patients 15.59 and 14.36; 0.008 x 15.59 = 0.124mSv). Two experienced musculoskeletal radiologists will measure the angle between the transepi-condylar axis and the femoral component on two separate occasions, one month apart, and will be blinded to earlier measurements (Fig. 1). The first of the two measurements will be used for calculation of the main study endpoint. The transepicondylar axis is a line drawn between the spike of the lateral epicondyle and the sulcus of the medial epicondyle [10]. The patient and the surgeon will not be informed about the actual amount of rotation until after the study has been completed.
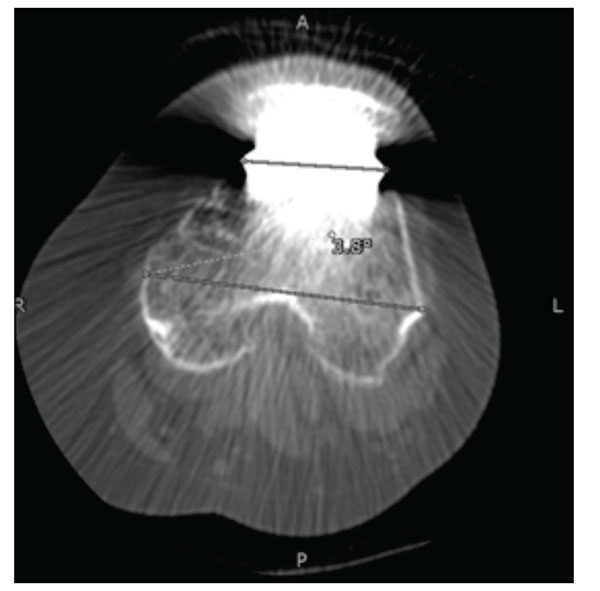
The angle between the transepicondylar axis and the femoral component is shown on a CT following patellofemoral joint replacement (in this example 3.8 degrees of internal rotation).
Three to five days after surgery, patients will be discharged, with regular follow-up visits at 2 weeks, 8 weeks, and 1 year. Regular X-rays (knee anteroposterior and lateral) at 8 weeks and 1 year. All patients will be asked to complete the KOOS questionnaire at 1 year.
Ethical Considerations
The study will be conducted according to the principles of the Declaration of Helsinki (59th World Medical Association General Assembly, Seoul, October 2008) and in accordance with the Medical Research Involving Human Subjects Act (WMO) and Good Clinical Practice guidelines.
Approval for this study has been obtained from the METC Zwolle ethics committee (reference number NL42639.075.13) and the local hospital board. Following review of the protocol, the METC concluded that patients will have no direct benefit from this study, and a radiation dose (approximately 0.12 mSv) is associated with CT.
Subjects can leave the study at any time for any reason if they wish to do so without any consequences. The investigator can decide to withdraw a subject from the study for urgent medical reasons.
The trial is registered at the Netherlands Trial Register (NTR4175).
Data Analysis
Categorical data will be summarized using frequencies and percentages, continuous data will be summarized using the number of observations and mean with range. The following patient demographic data will be presented in a table: number of patients, right or left knee (right/left), sex (male/female), age (year), height (cm), weight (kg), and BMI (kg/m2). The following surgery-related data will be recorded: number and type of previous surgeries, degree and extent of degenerative changes, size of prosthetic components, additional surgical procedures performed (e.g. tibial tubercle osteotomy, lateral release), number and type of complications.
For the primary study parameter (CT-based femoral component rotation expressed in degrees of rotation relative to the transepicondylar axis), the following data will be presented:
(1) The percentage of patients with optimal femoral component rotation (between 3 and 6 degrees of external rotation relative to the transepicondylar axis);
(2) Mean (range) femoral component rotation in degrees relative to the transepicondylar axis;
(3) The 95% confidence interval of the mean;
(4) A histogram depicting the distribution of rotation angles.
Furthermore, the intra- and interobserver reliability of the measurements will be assessed by calculating Kappa and creating a Bland-Altman plot.
(1) For the secondary study parameter (clinical outcomes at 1-year follow-up as assessed using the patient reported KOOS questionnaire), the following data will be presented:
(2) For each of the 5 subscales, and for each of the 2 points in time (preoperative and at 1-year follow-up): the normalized KOOS score (mean with range);
The change from baseline total KOOS for the 1-year follow-up (mean with range).
The correlation between the CT-based femoral component rotation and the change from baseline total KOOS for the 1-year follow-up will be assessed by calculating Pearson’s correlation coefficient.
All statistical tests will be two-sided, with a significance level of 0.05.
DISCUSSION
The current study will provide data on the actual amount of femoral component rotation in patellofemoral joint replacement, and the relationship of femoral component rotation with clinical results. With inclusion starting in 2014, and a follow-up of one year, we expect the presentation of data in the beginning of 2016.
AUTHORS’ CONTRIBUTIONS
HPWvJ initiated the study. REW, RPD and BJZ participated in the design of the study and developed the CT scanning protocol. REW and HPWvJ wrote the manuscript. All authors read and approved the final manuscript.
ABBREVIATIONS
| BMI | = Body Mass Index |
| CT | = Computed Tomography |
| DLP | = Dose Length Product |
| ED | = Effective Dose |
| KOOS | = Knee Injury and Osteoarthritis Outcome Score |
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

