All published articles of this journal are available on ScienceDirect.

The Pattern of Injury and Workload Associated with Managing Patients After Suicide Attempt by Jumping from a Height
Abstract
Purpose :
The aim of this study is to examine the pattern of injuries sustained and the hospital workload generated by patients who deliberately jump from height.
Method :
One regional trauma centre's admissions were scrutinized to find all patients who jumped, or were suspected of jumping from one storey or greater over a four year period. Patients who died prior to admission were excluded.
Results :
41 patients were included. Each patient suffered a mean of 3 injuries. The probability of calcaneal fracture was 0.32, of ankle injury 0.2, tibial fracture 0.2, femoral fracture 0.17, pelvic fracture 0.34, spinal injury 0.51, upper limb injury 0.26, head injury 0.2 and trunk injury 0.32. The mean length of inpatient stay was 7.9 days, rising to 17.9 for the 11 patients requiring intensive care. The average number of operations per patient was 1.5.
Conclusion :
Patients who jump from height generate large volumes of operative and inpatient workloads. Our data show that there may be a protective effect of limb trauma against lethal head, chest or pelvic injury. Injury to the upper limb is associated with a 4 times greater risk of head injury. The incidence of pelvic injury in this series is higher than in previous work. There was a high incidence of spinal fracture. Patients generated 64 surgical procedures and consumed a mean of 17.9 inpatient days, including prolonged stay in intensive care.
INTRODUCTION
Jumping from a height accounts for between 3 - 15% of the 140,000 suicide attempts in the UK each year [1-3]. Jumping requires little in the way of planning and skill to carry out and causes multiple severe injuries in those who survive [4].
According to the literature, those who attempt suicide by jumping from a height display common characteristics. They are predominantly male, middle aged, unemployed and single. 19- 97% of patients have a psychiatric diagnosis (most commonly schizophrenia) which is more severe than that suffered by those who employ other methods of suicide [2, 5-11]. The injuries sustained and the injury severity score is correlated to the height of the jump, the surface on which they land and position of the patient on landing [4, 6, 12-14].
The aim of this analysis of a retrospective case series is to examine the pattern of injuries sustained and the hospital workload generated by the management of patients who deliberately jump from height.
METHODS
The orthopaedic admission database (Bluespier, Bluespier International Ltd, Droitwich UK) of one regional centre was interrogated using keywords and injury descriptions from clinic letters and ward rounds combinedwith Boolean operators to find all patients who had either jumped or were suspected of jumping from any height between August 2008 and August 2012. No age limits were placed on the search (the unit was the regional adult and paediatric neurosurgical, orthopaedic and plastic surgical trauma centre). Where doubt existed as to whether the mechanism was a jump or fall of the patient was included as falls were more likely to have been in the presence of witnesses or be elucidated from the presentation or circumstance of the injury. Records were examined to identify those patients whose height of jump was one storey (equating to 10 feet, 3 metres) or greater. Case notes were utilised to collect the data shown in Table 1. Patients who died prior to admission were excluded. Records held at other acute and mental health trusts were not accessed. Blood toxicology reports were not sought in any cases as these are not routinely performed unless criminality is suspected.
RESULTS
Over the four year period 41 patients met the inclusion criteria for the study, of which 14 were female. The ages of patients was normally distributed about a mean of 32 years (Fig. 1). A previous psychiatric diagnosis had been established in 23 of the 41 patients, of which depression (10/41) was the commonest, followed by psychosis (6/41). Eighteen of the 41 patients had no documented diagnosis or evidence of a mental health condition prior to their jump. All patients landed on firm surfaces, 1 onto unpaved ground, the remainder onto road or paved surfaces.
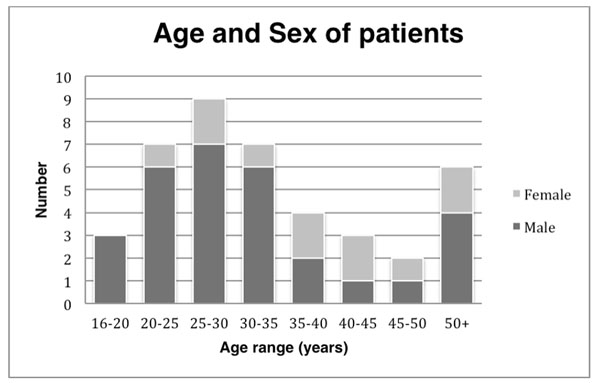
The age and sex of patients included in the retrospective case series of patients who jumped from a height greater than 3 metres between 2008 and 2012.
Data recorded from case notes and electronic records of each of 41 patients included in the retrospective case series
| Height of Jump | Treatment |
| Injuries sustained | Specialities involved |
| Number of theatre visits | Psychiatric diagnosis |
| Length of stay | Injury severity score (ISS) |
| Landing surface |
Data were interpreted using Microsoft Excel 2010 (Microsoft, Redmond, WA). Statistical tests were carried out using SPSS v.20 (SPSS Inc, Chicago, IL
The Frequency of injuries sustained to defined anatomical areas after a jump from height of greater than 3 metres seen in a retrospective case series of 41 patients.
| Injury | Closed | Open | Total |
|---|---|---|---|
| Foot | 8 | 1 | 9 |
| Calcaneum | 10 | 3 | 13 |
| Ankle | 9 | 0 | 9 |
| Tibia | 3 | 4 | 7 |
| Femur | 6 | 1 | 7 |
| Pelvis | 13 | 1 | 14 |
| Lumbar spine | 14 | - | 14 |
| Abdomen | 3 | - | 3 |
| Chest | 10 | - | 10 |
| Thoracic spine | 8 | - | 8 |
| Upper limb | 8 | 3 | 11 |
| Cervical spine | 5 | - | 5 |
| Head | 8 | 0 | 8 |
| Facial injury | 4 | 0 | 4 |
The probability of sustaining an injury to defined structures after a jump from height from greater than 3 meters
| Injury | Probability |
|---|---|
| Calcaneal fracture | 0.32 |
| Ankle fracture | 0.2 |
| Tibial fracture | 0.2 |
| Femoral fracture | 0.17 |
| Pelvic fracture | 0.34 |
| Spinal injury | 0.51 |
| Upper limb fracture | 0.26 |
| Chest/ abdo injury | 0.32 |
| Head injury | 0.2 |
When taken as a group, patients suffered a mean of three distinct injuries ranging from head injury to minor foot trauma. The incidence of specific injuries is shown in Table 2.
The median injury severity score (ISS) at presentation was 15 (range 4-50); 13 patients had an ISS less than 9, 8 patients an ISS of 9- 15 and 20 patients an ISS of 16 or greater. These scores showed no correlation of age. The mean height of jump was 30 feet (10 metres) with injury severity showing a positive correlation with respect to the height of jump (r= 0.651). The analysis did not take into account of those patients who died prior to arrival in the emergency department, however one patient died during admission.
Injury of feet was reported in 25% (excluding the os calcis). When taken as a separate entity, calcaneal injuries occurred in 13/41 patients (32%), which were open fractures in one quarter of cases [15]. No patient suffered an open ankle injury. Patients showed a 1 in 5 chance of sustaining a closed ankle injury. There was a 20% chance of patients sustaining a tibial fracture, of which 50% were open. Femoral fractures occurred in 7/41 patients; a single case was open.
Pelvic and acetabular fractures occurred in 14/41 patients (34%). H shaped sacral fractures were diagnosed in 4/14 cases [16]. One of these patients (1/4) showed a mixed H shaped and vertical shear (VS) pattern. Two patients sustained an acetabular injury in addition to the H shaped sacral fracture. Of the remaining 10 pelvic injuries, one sustained an open iliac wing fracture with an associated acetabular injury; two acetabular fractures only; five a lateral compression (LC) fracture; one anteroposterior compression (APC) fracture and one a vertical shear pattern. Overall, 1 in 5 patients with a pelvic ring injury sustained an acetabular fracture.
Upper limb injuries occurred in 11/41 cases. One third of these were open. No extremity fractures were associated with neurovascular compromise. Patients suffered abdominal injuries in 3/41 cases. A single patient required a laparotomy. Ten patients sustained chest injuries. The only treatment required in any patient was a chest drain.
Just over half of patients sustained spinal injuries (21/40). One third of these were lumbar spine injuries, four were confined to the thoracic spine and a single patient sustained an isolated cervical spine injury. Eight patients had multilevel spinal injuries; four sustained cervicothoracic and four thoracolumbar fractures. Eight patients required urgent surgery to manage their spinal injuries. Three patients were left with neurological deficits.
Neurosurgical intervention for severe head injury was required in four cases. Three patients suffered a major head injury not requiring urgent surgery. All patients with severe head injuries required treatment in intensive care (ITU). Five patients sustained minor head or facial injuries. The mean length of inpatient stay was 7.9 days (0- 97). 11 patients required treatment in intensive care for between 1 and 55 days (mean of 3.6 days). For those patients who required a stay in ITU, overall mean length of stay increased to 17.9 days (median 10 days). On average, patients required at least one surgical procedure. Orthopaedic surgery was required in 32 cases, neurosurgery in eight, plastic surgery in six, maxillofacial surgery in two, general surgery and ophthlalmology in one case each.
The calculated probability of sustaining an injury to a given region is shown in Table 3.
DISCUSSION
This work describes the injuries sustained by patients who jump from height and the resources necessary to treat them. In doing so, it helps the treating team to look for common injury patterns.
The characteristics of our study population are broadly similar to those described in the literature, the principle difference being that 44% of this cohort show no established psychiatric diagnosis prior to jumping [2, 5-7, 17]. In the UK, mental health trusts keep separate records to acute trusts, and these were not available during the study. Despite this, our study shows similar rates of injury to previously published work. 54% of our patients suffered spinal injuries, which concurs with figures of 38- 80% in the literature [2, 4-6, 18, 19]. 24% sustained chest injuries, 34% pelvic injuries and 20% head injuries, all within ranges previously published [2, 4-6, 19-21]. Data from this study show an incidence of limb fracture of 93% in contrast to published figures of 38 to 60% [2, 4, 6, 18, 19, 21]. However, the majority of previous work includes patients who died in their analyses; there may be an effect of limb trauma being protective against lethal head, chest or pelvic injury.
Our series, though small, shows that the probability of sustaining head, upper limb, chest and abdominal injury when lower limb and pelvic trauma has been sustained is 0.48, suggesting the possibility that injuries to these areas protect the head and torso. For those patients who sustained injuries to both the upper and lower body (where the division is the L5/S1 junction), 38% were predominantly left sided direct injuries, 23% were predominantly right-sided direct injuries and 38% were bilateral impact injuries, perhaps indicating patients where attitude on landing was in a lateral, supine or prone position.
Fractures to the lower limbs protected the pelvis from injury. The probability of pelvic injury when lower limb injuries occur is 0.74 when compared with pelvic injury in the absence of lower limb fractures. In contrast, injury to the upper limb is associated with a 4 times greater risk of injury to the head.
The incidence of pelvic injury in this series is higher than previous estimates (34% vs 25%). H shaped sacral fractures occurred in 10% of patients (16). Fang et al. showed an incidence of 29% simple pelvic fractures, 13.7% vertical shear and 28% lateral compression fractures in a series of 248 pelvic injuries due to falls from height in 2008 [20]. In comparison our series shows an incidence of 36% of lateral compression fractures, 14% of vertical shear pattern and 14% of anteroposterior compression injury.
Few patients in this series sustained severe head and cervical spine injuries. Dickinson et al. found that injuries in the head and chest were significant predictors of mortality (p< 0.005), and patients with these injuries died from a lower height of fall [22]. This is supported by Richter et al. who showed a 50% mortality of patients sustaining head injury a falling from a single storey [6]. Patients with these injuries have a reasonable probability of dying prior to admission, and so would be excluded from the study.
Managing these patients requires a multidisciplinary approach and consumes significant resource. In this series, orthopaedic opinion was required in every case, neurosurgical and intensive care input in eight each (20%). Reviewing the literature shows that orthopaedics is required in 71% of cases, neurosurgery in 21% and intensive care in 24% for patients who jump or fall from height [4]. These patients represent a substantial workload for operating theatres, with each patient requiring a mean of 1.5 theatre visits. The 32 patients requiring surgery visited theatre 64 times, though mostly only once. In one case a patient required 8 separate operations prior to discharge.
The average financial cost of managing these patients is difficult to calculate. Each patient requires a different number of operative procedures, with differing amounts of time and equipment resource allocated to each case. In the National Health Service, the mean cost of intensive care is between £1700- 2000 per twenty four hour period, with normal inpatient ward care costing £250 per day [23]. The mean cost of acute inpatient care, excluding prior or subsequent mental health care and operative procedures is approximately £10,925. In one case with prolonged intensive care and inpatient stay, this rose to at least £120,500, again excluding operative procedures (of which there were eight) and the implants and equipment associated with these.
There are limitations to this case series, including its retrospective methodology and the potential absence of patients who sustained isolated head, abdominal and thoracic injuries. Any patient who died prior to admission was excluded and although the number of patients in the cohort is small, it is likely to represent the majority of patients who jumped from height within our region during the time period examined.
CONCLUSION
Patients sustained multiple injuries following a jump from height that required the input of the majority of surgical specialties. The typical patient is male, middle aged and has pelvic, spinal and limb injuries. Patients generate large volumes of operative and inpatient workloads. It seems that limb injuries protect the trunk and pelvis.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

