All published articles of this journal are available on ScienceDirect.

A Novel Surgical Technique for Removing Buried Cannulated Screws Using a Guidewire and Countersink: A Report of Two Cases
Abstract
Removal of metal implants is a common procedure that is performed for a variety of indications. However, problems such as a buried screw head may occasionally arise and render hardware removal difficult or even impossible. The problem is further compounded when the initial screw was inserted percutaneously or via a minimally-invasive (MIS) technique. In the present paper, we introduce a novel, minimally invasive technique to remove buried cannulated screws which obviates the need for excessive extension of the skin incision, surgical exploration, soft tissue dissection or excess bone removal, which surgeons may otherwise have to undertake to uncover the buried screw head. This technique is especially useful in removing cannulated screws which have been inserted using small stab incisions and MIS techniques initially. This technique can be applied to the removal of buried cannulated screws which are placed into any bone in the body.
INTRODUCTION
Removal of metal implants is a common procedure that is performed for a variety of indications, including planned removal of position screws (e.g. syndesmotic screws), infection, prominent hardware, soft tissue irritation, cosmesis and patient preference [1-8].
However, problems such as a buried screw head may occasionally arise and render hardware removal difficult or even impossible [4, 9]. The problem is further compounded when the initial screw was inserted percutaneously or via a minimally-invasive (MIS) technique. Multiple failed attempts at buried screw removal cause undue skin and soft tissue trauma from repeated manipulation and require more extensive incisions and bone loss, all of which could have obvious impact on the risk of wound complications, hardware breakage, iatrogenic fractures [10, 11] and cosmesis [12-15].
There have been several publications in the literature which describe various techniques for removing broken implants [6, 16, 17], but only few have dealt specifically with the retrieval of buried screw heads. In 1992, Moran described a technique for the removal of cannulated screws with buried heads in the femoral neck in the setting of total hip arthroplasty in a patient who had undergone prior cannulated cancellous screw fixation. Screw removal is facilitated by retrograde drilling of the screw (i.e. in the direction of the screw tip towards the screw head). This technique requires the exposure of the screw tip, which is made possible by dislocating the femoral head (which fortunately is part of the hip replacement procedure). This requirement to expose the screw tip in order to enableretrograde drilling limits its application in other scenarios where screw tip exposure cannot be reasonably performed without causing undue morbidity. We hereby report a minimally invasive technique to remove buried or overgrown cannulated screws in almost any part of the body with the help of a cannulated guidewire and countersink under fluoroscopic guidance.
TECHNIQUE
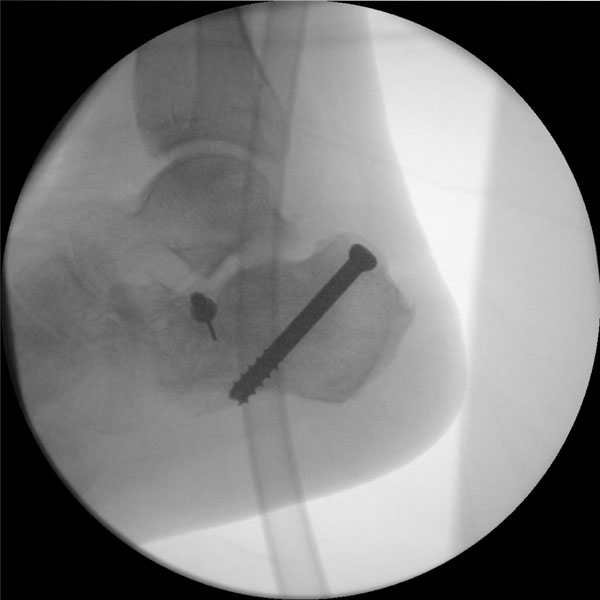
Under general or regional anaesthesia, the patient is cleaned and draped in the routine fashion on a radiolucent table. The cannulated screw to be removed is located under fluoroscopy and a stab incision made on the overlying skin over the original scar. The fluoroscopy unit is then adjusted until a perfect circle of the cannulated hole of the buried screw is clearly visible on the screen (Fig. 1). This step is familiar to surgeons who have experience in placing distal interlocking screws through cephallomedullary nails for the femur and tibia via percutaneous stab incisions.

The cannulated screw is located under fluoroscopic guidance and a corresponding skin incision is made. The fluoroscopy unit is then adjusted until a perfect circle of the cannulated hole of the buried screw is clearly visible on the screen.
A cannulated guidewire is accurately inserted into the cannulated hole of the screw under fluoroscopic guidance.

A cannulated countersink is passed through the guidewire and used to remove the excess bony and soft tissue overgrowth, until the buried screw head is fully uncovered.

X-rays prior to implant removal. The patient had undergone percutaneous screw fixation of intra-articular calcaneal fracture four months earlier. Unfortunately, two K-wires were broken at the index operation.
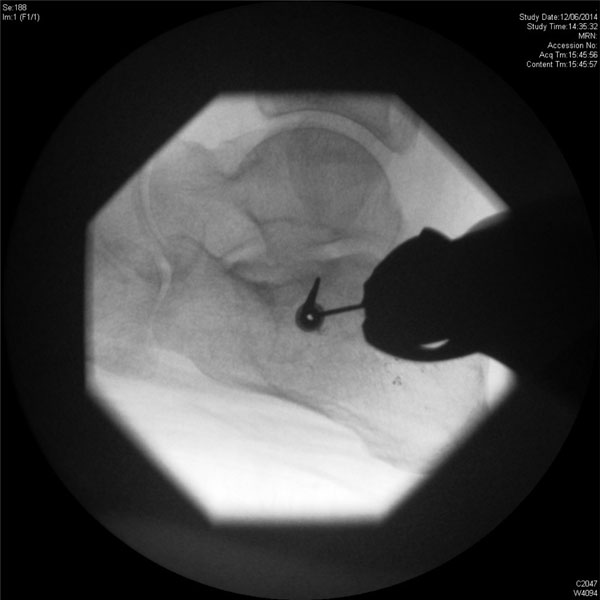
The fluoroscopy unit is adjusted until a perfect circle of the cannulated hole is clearly visible. An attempt is then made to insert the cannulated guidewire into the cannulated hole under fluoroscopic guidance.

The cannulated guidewire is now inserted into the cannulated hole of the buried screw.

Fluoroscopic image showing successful removal of the buried screw.
The tip of the cannulated guidewire is then placed in the centre of the circle and the wire is aligned along the direction of the x-ray beam. The cannulated guidewire is then driven into the cannulated hole of the screw under fluoroscopic guidance (Fig. 2). A cannulated countersink is subsequently passed through the guidewire and used to remove the excess bony and soft tissue overgrowth, until the buried screw head is fully uncovered, ensuring that corresponding cannulated screw driver can be properly seated onto the screw head (Fig. 3). The uncovered screw can now be removed in the usual manner.
Two cases where the technique proved valuable in removing buried cannulated screws in the sinus tarsi after calcaneal fracture fixation have been presented.
CASE SERIES
The first is a 56-year old patient with diabetes, peripheral vascular disease and end-stage renal failure on regular hemodialysis who had fractured his calcaneum following a motor vehicle accident and underwent percutaneous screw fixation of the fracture 4 months earlier. Following fracture union, he requested a removal of implants. Initial attempts at removing the sinus tarsi screw had failed as the screw head was buried under a layer of bone and callus. Using the present technique, the screw head was successfully cannulated with a K-wire and was removed (Figs. 1-3).
In the second case, a 24 year-old labourer had previously sustained an intra-articular calcaneal fracture following a fall from height 4 months earlier. This was again fixed using percutaneous cancellous screws (Fig. 4). Unfortunately, two K-wires were broken during the initial fixation and were left in situ. Following fracture union, the patient requested a removal of implants. The sinus tarsi screw removal was difficult due to buried screw head, but this was successfully salvaged using the present technique (Figs. 5-7).
DISCUSSION
Buried screw heads can occur when the screw head penetrates the outer cortex of the bone, especially in osteoporotic patients. In addition, screw heads may also be subsequently buried by overgrowth of cortical bone and soft tissue, especially in children or adolescents [9]. An earlier description of buried cannulated screw removal via a retrograde technique by Moran requires exposure of the screw tip, which is not feasible in many situations, thereby limiting its application. The method which we have described is a minimally invasive technique which obviates the need for excessive extension of the skin incision, surgical exploration, soft tissue dissection or excess bone removal, which surgeons may otherwise have to undertake to uncover the buried screw head. This technique is especially useful in removing cannulated screws which have been inserted using small stab incisions and MIS techniques initially.
In summary, we present a simple minimally invasive technique which simplifies the removal buried cannulated screws. The technique utilises standard instruments available in most cannulated screw systems. It involves the accurate placement of a guidewire into the cancellous screw hole, exposure of the buried screw head using the countersink and subsequent screw retrieval, all of which can be achieved relatively easily through a stab incision with minimal soft tissue trauma. This technique can be applied to the removal of buried cannulated screws which are placed into any bone in the body.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

