All published articles of this journal are available on ScienceDirect.

A New Case of Fracture of a Modular Femoral Neck Device After a Total Hip Arthroplasty
Abstract
This report addresses a new case of a modular femoral neck fracture after total hip arthroplasty. A now seventy-three-year- old overweight female underwent total hip replacement of the right hip because of osteoarthritis in the year 2002. Then, years later, the head and the polyethylene were changed due to wear. In October 2014, the patient was transferred from the trauma department of her hometown to our department after she had slipped and fallen directly on her right hip. The x-rays done at the trauma department have shown no periprosthetic fracture but a fracture of the modular neck. Therefore, the patient was transferred to our department in order to undergo a revision arthroplasty with change of the stem and head after splitting the femur.
INTRODUCTION
Since the introduction of the first modern total hip replacement by Sir John Charnley, various prosthesis designs have undergone many modifications. Recently, the number of implanted modular femoral neck implants has increased. The advantage of this system is to include the right combination of limb length, offset, anteversion and easier revision. Taken together, these devices provide more flexibility for the surgeon. However, there remain concerns about corrosion, stability, fretting of the modular junction, and cold welding. There is little literature available regarding catastrophic failure in modular hip implants. This report addresses a new case of a modular femoral neck fracture after total hip arthroplasty.
CASE REPORT
A now seventy-three-year- old overweight (90kg, 1,67m, BMI 32,27) retired female underwent a total hip replacement of the right hip because of osteoarthritis in the year 2002. Then, years later, the head and the polyethylene were changed due to wear. In October 2014, the patient was transferred from the trauma department of her hometown to our department after she had slipped and fallen directly on her right hip. After her fall, she reported severe pain and weight bearing was immediately impossible. She could not even move her left lower extremity. The x-rays done at the trauma department have shown a correct positioning of the acetabular and femoral components and no periprosthetic fracture but a fracture of the modular neck. The breakage represents a new mechanism because failure was not in the neck or on its basis.
The breakage was proximal ant. the neck head junction, which has thus far not been described in the relevant literature (Fig. 1a, b). Therefore, the patient was transferred to our department in order to undergo a revision arthroplasty. The blood samples, which were taken preoperative, have not identified any infection. Also, the microbiological examination of the intraoperative smears and the biopsies which were taken have not shown any evidence of a bacterial joint inflammation.
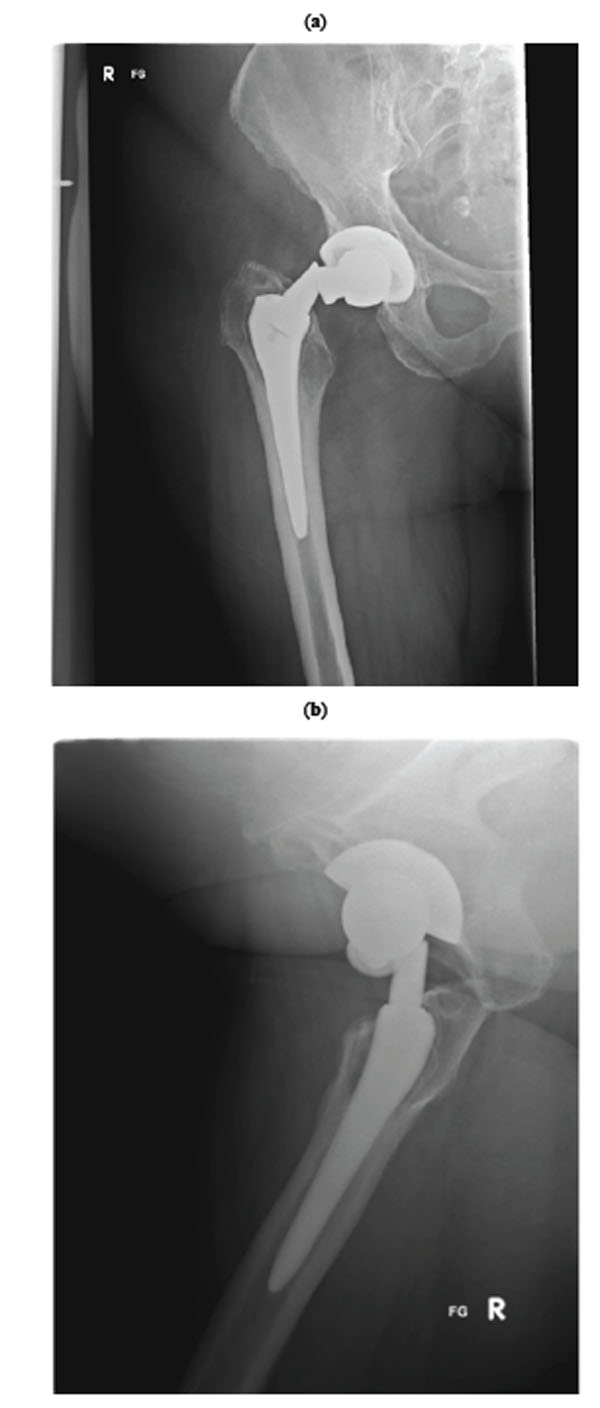
(a) preoperative X-ray a.p. (b) preoperative X-ray axial.
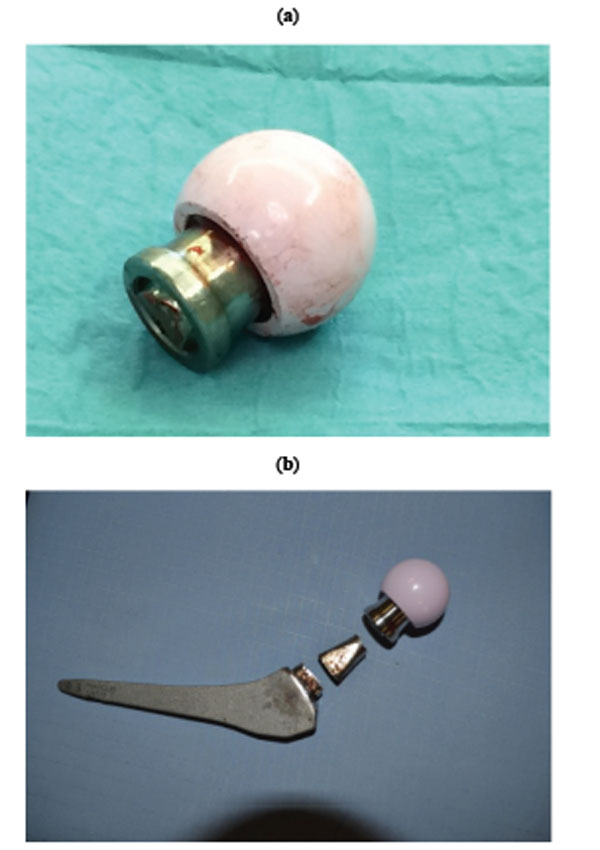
(a) Explanted head: breakage proximal anterior the neck head junction, (b) Explanted

Postoperative X-ray.

Intraoperative picture of the soft tissue.
After having used an antero-lateral approach to the hip, the head and the proximal aspect of the neck were removed. We could not remove the distal aspect of the neck, which remained in the bore of the femoral stem (Fig. 2a, b). Therefore it was impossible to use a stem extractor. The intraoperative situs is shown in Fig. (4) presenting metallosis and inflammation. Our universal stem extractor was also unable to remove the implant, which is why an extended osteotomy was necessary to remove the femoral stem and the distal fragment of the modular neck. The patient received a cementless Alloclassic Zweymüller® SLL Revision Stem and BioBall® 3XL head. The extended osteotomy was fixed with the use of compression cerclage Gundolf (CCG). The patient received blood supply through a haemoglobin drop. Postoperatively, she was allowed to bear weight of 15 kg (Fig. 3).
DISCUSSION
Although modular hip systems gain more and more popularity because of the possibility of restoring the normal hip biomechanics by adjusting a correct limb length, offset and femoral anteversion, more and more severe complications are reported.
A fracture of a femoral component is a rare but severe complication in total hip arthroplasty. In 1975, Chanley presented a clinical study of 17 fractures of Charnley femoral prostheses, occurring over a period of about ten years. The overall fracture rate was only 0.23 percent. However, the rate for males over 196 lb (88 kg) was 6.0 per cent [1].
In the 1980s, Aspenberg et al. presented technical analyses which showed that inadequate welds were responsible for five prostheses fractured through the neck after 5-12 years [2].
In 2010, the first fracture of a modular femoral neck after a THA was reported by Commander Geoffrey Wright, MD. The examination of the distal fragment of the modular neck with the use of light microscopy showed marked fretting and corrosion damage and black fretting with corrosion debris. The damage was concentrated on the lateral and anterior surfaces where they mated with the stem [3].
Fretting by micro-motion between the modular components are blamed for particle and ion release into the surrounding and this may attack the alloy and lead to implant failure [4-7].
Recently, there was the first case reported on a fracture of a cobalt-chromium modular femoral neck component (all earlier reported cases occurred with titanium components), which was meant to prevent weakness [8].
Our case represents a new mechanism because failure was not in the neck or on its basis. The breakage was proximal ant. the neck head junction, which has not yet been described in the literature.
Moreover, cobalt-chromium modular necks can produce severe soft-tissue damage [9].
In conclusion, modular hip systems provide an excellent opportunity to restore the normal hip biomechanics, but the surgeon must be aware of the possible complications. Furthermore, there must be more preclinical testing undertaken before new materials and new modular hip designs are implanted.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

