All published articles of this journal are available on ScienceDirect.

Clinical and Ultrasound Features of Constrained Extensor Carpi Ulnaris Tendinopathy; Stenosing Tendovaginitis and Tendinosis in the Patients with Dorsal Ulnar-sided Wrist Pain
Abstract
Aims:
To investigate the ultrasound and clinical features of constrained Extensor Carpi Ulnaris (ECU) tendinopathy to have a better understanding of ulnar-sided wrist pain.
Background:
The cause of dorsal ulnar-sided wrist pain tends to be vague and unclear due to too many closely adjacent small structures. Constrained ECU tendinopathy has been scarcely reported, and it is unknown how often this disorder is found among the wrists with such pain.
Objective:
The purpose of this study was to compare the patients’ backgrounds between two groups; the wrists diagnosed as constrained ECU tendinopathy by using ultrasonography and the other dorsal ulnar-sided painful wrists.
Methods:
Totally 103 wrists from 103 consecutive patients (45 men and 58 women; age 13-78 years; mean age 43.7 years) who visited our clinic with dorsal ulnar-sided wrist pain were examined by physical test and sonography. We separated them into two groups of wrists with or without constrained ECU tendinopathy and compared patients’ data between them.
Results:
Twenty-six wrists (25%) were diagnosed as constrained ECU tendinopathy mainly located in the distal area than the ulnar osseous groove. All of them were ECU tendovaginitis and 15 wrists were concomitant with ECU tendinosis. The results of the comparison showed the proportion of females was higher, that of patients who have relevant sports activity was lower, and patients’ age was slightly higher in the wrists with constrained ECU tendinopathy (p<0.05).
Conclusion:
Among the wrists with dorsal ulnar-sided pain, constrained ECU tendinopathy occurs more frequently in middle-aged to elderly women and less frequently in sports-related patients, These tendencies are similar to other stenosing synovitis such as de Quervain`s disease.
Others:
For vague dorsal ulnar-sided wrist pain, physician should be aware of these tendencies and the advantage of ultrasonography given that constrained ECU tendinopathy might be frequently encountered more than expected.
1. INTRODUCTION
The sixth dorsal extensor compartment of the wrist has unique anatomical features compared with the other dorsal extensor compartments. The extensor carpi ulnaris (ECU) runs through a dorsal fibro-osseous tunnel formed by the ulnar groove and tendon sub-sheath, which is an independent layer composed of mixed tight and loose collagen fibers, clearly differentiated from the extensor retinaculum [1-4]. The ECU tendon sub-sheath contributes to preventing ECU dislocation and allowing it to move adequately by neutralizing the dislocation force in the pronosupination movement [1-3, 5].
If a patient has dorsal ulnar-sided wrist pain, the sixth dorsal extensor compartment is one of several possibilities as a causal location physicians should be aware of, as well as the triangular fibrocartilage complex (TFCC), distal radioulnar joint (DRUJ), lunotriquetral and other extrinsic ligaments. Garcia-Elias recently proposed classifying ECU tendinopathy [6], a term that has been used to designate painful dysfunctions of the ECU tendon [7], into two types in his review article. He described the situation where ECU becomes entrapped in the compartment as “constrained ECU tendinopathy,” which has been previously called stenosing tenovaginitis [8, 9] or stenosing tenosynovitis [10, 11]. On the other hand, the ECU tendon subluxation and dislocation, which occurs when a disrupted ECU sub-sheath is not able to retain the ECU, was described as “unconstrained ECU tendinopathy”. Unconstrained tendinopathy would be detectable by a distinctive history of recent trauma frequently associated with racket or stick sports such as tennis if a physician can sense the ECU luxating from the compartment [12, 13]. Lacking such distinctive features, constrained ECU tendinopathy may be hardly distinguished from other dorsal ulnar-sided wrist painful diseases, and its diagnosis should mainly rely on imaging modalities [6] and careful physical examination. The ECU synergy test is one of the previously reported provocative maneuvers, and it is unique in that it detects ECU tendon synovitis using the static contraction of the ECU and flexor carpi ulnaris (FCU) [14].
Ultrasonography is non-invasive, user-friendly, and easily available even at patients’ first visit. Although the sonographic examination does not suffice to fully understand the dorsal ulnar-sided wrist pain, not having the ability to give us the image inside the joints and bone marrow, its strength of sharply showing the superficial structures such as nerves, muscles, tendons, and dorsal extensor compartments including the ECU sometimes allows physicians to find a diagnostic clue [13, 15, 16].
In this study, we aimed to investigate if we could see any difference between two groups in dorsal ulnar-sided painful wrists; the wrists diagnosed as constrained ECU tendinopathy and the other wrists to have a better understanding of such pain. Ultrasonography was used for the differentiation of these two groups. A couple of X-ray measurements and the results of the ECU synergy test were also compared between them.
2. MATERIALS AND METHODS
This study was conducted in accordance with the principles embodied in the Declaration of Helsinki and was approved by the institutional review board and ethics committee in our clinic (the Research Board of Healthcare Corporation Ashinokai, Gyoda, Saitama, Japan [ID number: 2015-5]). Consecutive patients who visited our clinic for dorsal ulnar-sided wrist pain during a five-year period from 2016 to 2021 were enrolled. They were informed about the aim and process of the study and gave written informed consent to participate. Excluding criteria includes acute and old fractures, gout, rheumatoid arthritis, calcium deposit, and bone tumor. In their initial visit, all patients underwent plain radiographs so that we could find any abnormal findings led to such exclusive diagnoses. Some patients had blood test as necessary and were excluded if the result indicated gout or rheumatoid arthritis. Immediately after plain radiographs, we studied their wrists with ultrasonography following a physical examination in the consultation room. The patients were diagnosed as constrained ECU tendinopathy if they met the following findings; 1) pain at dorsal ulnar side of the wrist with forcefully ulnar deviation against resistance and with the forearm in supination, the best way to test the power of the ECU muscle; ECU becomes more angular in an ulnar direction immediately distal to the ECU sub-sheath as well as the strain on the tendon increase [13, 17-19], 2) the examined wrist sonographically showed ECU tendinosis and/or ECU stenosing tendovaginitis [6].
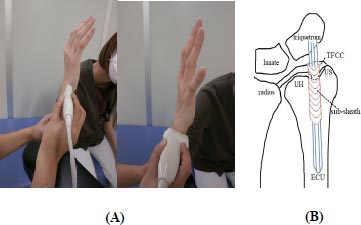
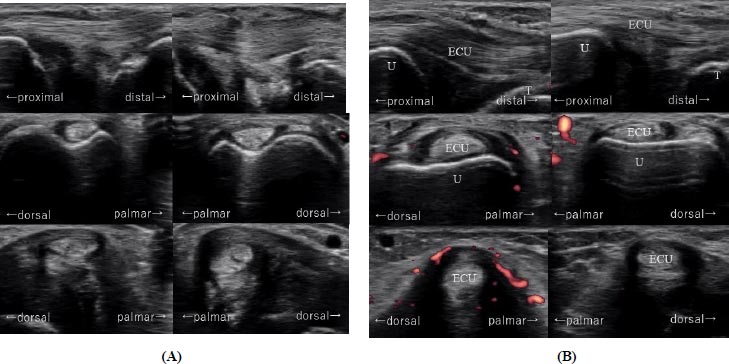
With regard to the sonographic assessment, we observed ECU through the sixth dorsal extensor compartment from the dorsal sulcus of the distal ulna to its enthesis to the fifth metacarpal base with longitudinal and transverse images using the Avius ultrasound system (Hitachi Medical Corporation, Tokyo, Japan) or the SONIMAGE HS1 ultrasound system (Konica Minolta, INC., Tokyo, Japan). A linear array 17-MHz transducer (EUP-L75, contact area; 9mm × 43mm) or 18-MHz transducer (L18-4, contact area; 10mm × 44mm) was used. Patients’ hands were positioned with the wrist and forearm in a neutral position, and the elbow flexed 90° by an examiner holding them (Fig. 1). Images were created on display showing a side-by-side comparison of the right and left wrist for better diagnosis. For the diagnosis of constrained ECU tendinopathy, we referred to the sonographic findings such as ECU thickening, intratendinous hypoechogenicity, irregular fibrillar pattern for ECU tendinosis, tendon sheath distension, blood flow detected on color and/or power Doppler imaging for ECU stenosing tendovaginitis (Fig. 2).
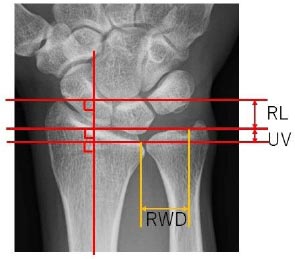
In total, 103 affected wrists from 103 patients (45 men and 58 women; age 13-78 years; mean age 43.7 [SD 17.0] years) were included in this study. We separated them into two groups of dorsal ulnar-sided painful wrists with or without constrained ECU tendinopathy according to the diagnostic criteria mentioned above and compared the patients’ data between them. The compared items in patients’ backgrounds included patients’ gender, age, body mass index (BMI), hand dominance, previous trauma, previous overloaded manual work, and relevant sports activities. In addition, three radiographic measurements, radial length [20], ulnar plus variant [21], and rotational width of DRUJ, and the results of the ECU synergy test were also compared. With regard to the ulnar plus variant, we measured it using the line which crossed the volar-ulnar edge of the radiocarpal joint. The rotational width of DRUJ was measured on this line as the distance between the radius and the crossing point on its perpendicular line from the ulnar fovea (Fig. 3). On the radiographic examination, the radiological technologist in our clinic took a posteroanterior image of the wrist joint with the patients’ shoulder abducted 90°, elbow flexed 90°, and forearm and wrist in a neutral position. All radiographic measurements were measured three times for each wrist by using software from SYNAPUS Wz (FUJIFILM Co., Japan), and the mean value [mm] was adopted. The ECU synergy test was performed before the sonographic examination. In the test, the examiner grasps the patient’s thumb and long finger, and the pain along the ECU induced by the patient radially deviating the thumb against resistance was deemed positive [14]. All physical and sonographic examinations, radiographic evaluation, and measurements were carried out by a senior hand surgeon with 17 years of experience in surgery and 6 years of experience in ultrasound.
| - |
Wrists with Constrained ECU Tendinopathy (n=26, BMI: n=24) |
Wrists without Constrained ECU Tendinopathy (n=77, BMI: n=63) |
P-value |
| Gender (male/female) | 7/19 | 38/39 | <0.05 |
| Age (years) | 52.8 (SD 13.7) | 40.6 (SD 16.9) | <0.01 |
| (21 - 76) | (13 - 78) | - | |
| Body Mass Index (BMI) | 23.5 (SD 3.8) | 23.9 (SD 4.6) | 0.64 |
| (19.6 - 26.7) | (17.3 - 33.9) | - | |
| Hand dominance | 18/8 | 51/26 | 0.78 |
| (Dominant side/nondominant side) | - | ||
| Previous trauma (present/absent) | 3/23 | 12/65 | 0.61 |
| Previous overloaded manual work | - | ||
| (Present/absent) | 13/13 | 31/46 | 0.39 |
| Relevant Sports activity | 1/25 | 21/56 | <0.05 |
| (Present/absent) | - | ||
| Radiographic measurement (mm) | - | ||
| Radial length | 10.2 (SD 2.0) | 11.0 (SD 1.9) | 0.11 |
| - | (6.8 - 15.6) | (5.5 - 14.8) | - |
| Ulnar variant | 1.7 (SD 1.3) | 1.5 (SD 1.4) | 0.6 |
| - | (-2.5 - 3.5) | (-2.0 - 4.5) | - |
| Rotational width of | 12.6 (SD 1.3) | 13.1 (SD 1.7) | 0.19 |
| Distal radioulnar joint | (9.6 - 14.5) | (8.8 - 17.0) | - |
| ECU synergy test (positive/negative) | 14/12 | 8/69 | <0.01 |
In the statistical analyses, comparisons were performed using the Student t-test for age, BMI, and radiographic measurement and using the Mann-Whitney U test for gender, hand dominance, previous trauma, previous overloaded manual work, sports activity, and results of the ECU synergy test. Results were deemed significant if P<.05.
3. RESULTS
Twenty-six (25%) of the 103 examined wrists were diagnosed with constrained ECU tendinopathy. All of them sonographically showed ECU stenosing tendovaginitis, and 15 out of 26 wrists showed ECU tendinosis, concomitant with ECU stenosing tendovaginitis. In all these 26 wrists, constrained ECU tendinopathy appeared at the distal area than the ulnar osseous groove, 10 of which showed it ranged proximally through the groove.
We had no patient with traumatic ECU tendon subluxation or dislocation, which is referred to as unconstrained ECU tendinopathy by Garcia-Elias [6]. Table 1 represents the patients’ information and the results of statistical analyses. Since reports of weight and height by patients were not mandatory, we made comparisons using only obtained data for BMI.
As a result, the comparison of gender, age, sports activity, and the result of the ECU synergy test showed significant differences. In the wrists with constrained ECU tendinopathy, the proportion of females was higher, and that of patients who have relevant sports activity was lower with significance than in the wrists without constrained ECU tendinopathy, respectively. The mean age of the patients in the wrist with constrained ECU tendinopathy was significantly higher than that of the other patients by 12.2 years. The ECU synergy test tended to be positive in the wrists with constrained ECU tendinopathy. Its sensitivity, specificity, positive, and negative predictive values were 63.6%, 85.2%, 53.8%, and 89.6%, respectively.
4. DISCUSSION
As a summary of this study results, constrained ECU tendinopathy tended to occur more frequently in women and have lower relevance to sports activity compared with other dorsal ulnar-sided wrist painful conditions when no decisive abnormalities for diagnosis were found in radiography. Although the patients diagnosed with constrained ECU tendinopathy tended to be older, the difference in patients’ age was slight. The specificity and negative predictive value of the ECU synergy test were higher than 80%, whereas the sensitivity and positive predictive value were not reliably high.
Narrowing down the cause of ulnar-sided wrist pain has still been challenging. Too many closely adjacent small structures make precise identification of the anatomy responsible for the patient’s pain difficult. Even though we saw the rigid development of imaging modalities such as high-resolution magnetic resonance imaging (MRI), there are quite a few cases where image findings are not decisive for diagnosis [22]. If so, one option for the next step would be arthroscopy, enabling physicians to gain detailed information about the wrist joint [18, 23]. However, if patients’ symptoms are not recalcitrant and severe or they are not highly demanding as in elite athletes, costly, time-consuming, and invasive examinations such as computed tomography, MRI, and arthroscopy tend to be omitted. At the patient’s first visit, some provocative maneuvers to reproduce symptoms and easily available modalities such as ultrasonography could be used as feasible firsthand examinations apart from plain radiographs. Ultrasonography would be worth trying as it can provide decisive information for diagnosis in such cases as ECU tendinopathy [13, 15, 16]. In addition, relief of symptoms by a selective local injection helps to confirm the diagnosis [14].
Garcia-Elias [6] described the details of ECU pathology by differentiating between two major types of ECU tendinopathies: constrained and unconstrained tendinopathy. He mentioned in both types of tendinopathy; it is frequent to find associated pathology to the ulnocarpal joint and/or DRUJ. Unconstrained ECU tendinopathy has been reported in relation to trauma or sports activity [12, 24]. MacLennan et al. [13], who assessed the results of ECU tendon sheath reconstruction for ECU subluxation, inferred the combination of ECU tendon motion during hyper supination and ulnar deviation, a flattened distal ulnar groove, and repetitive stress or overuse injury that weakens the tendon sheath as a cause of subluxation. They also underlined the importance of dynamic ultrasonography as a diagnostic tool for this condition. However, we had no opportunity to encounter it among the patients enrolled in this study.
In the article of Garcia-Elias [6], constrained ECU tendinopathy was further classified into ECU tendinosis and ECU stenosing tendovagititis. The former is supposed to be tendon thickness with obvious alterations in its inner blood supply as a result of repetitive stress or other chronic inflammatories such as gout and chondrocalcinosis, whereas the tendon sub-sheath becomes thick in the latter for most often unknown reasons. The pathology of constrained ECU tendinopathy has been considered a disturbance of tendon excursion caused by degenerative thickening of the tendon sheath and tendon as in de Quervain’s disease and has been previously reported as names of stenosing tenovaginitis [8, 9], stenosing tenosynovitis [10, 11] or ECU syndrome [25] by other authors. Local trauma immediately before the onset of symptoms [9, 10] and radiographic abnormalities such as a displaced non-union or degenerative change of the ulnar styloid [10], which were excluded from our study in the process of patients’ selection, were described as patients’ background for those who underwent surgery following failed conservative treatments. On the other hand, Futami and Itoman [25] reported 43 ECU tenoviginitis patients out of 155 patients with dorsal wrist pain (28%) whose radiographs were normal and who had no history of wrist trauma. They emphasized that all patients had repetitive overuse before the onset of symptoms instead, and two of three operated cases had an anomalous accessory ECU tendon. In this series of patients with constrained ECU tendinopathy, only three of 26 patients had a history of previous trauma, and 13 of 26 had a history of overloaded manual work. The disease tended to be prevalent in female and middle-aged patients and less relevant with sports activity. In light of these similarities with other stenosing synovitis such as de Quervain’s disease, we assume constrained ECU tendinopathy should be recognized as a degenerative and inflammatory disease rather than a traumatic one. As Crimmins and Jones [10] pointed out in previous articles, physicians should be aware that there might be quite many cases of constrained ECU tendinopathy among patients with dorsal ulnar-sided wrist pain; the number of 25% shown in this current study would be more than we expected considering the paucity of the previous report regarding the disorder. Although assessing the treatment outcome is beyond the scope of our aim, our patients generally responded well to conservative treatments, including rest, immobilization, non-steroidal anti-inflammatory drugs, and local corticosteroid injection, except for only one patient who underwent ECU tendon sheath release following a failure of four times of corticosteroid injections.
The best positions to reproduce pain of constrained ECU tendinopathy are controversial. In previous cadaver studies, the ECU synergy test was reported to yield high ECU tendon strain but no higher pressure in the fibro-osseous tunnel than in the neutral wrist position, whereas both measurements were highest in simultaneous supination of the forearm and carpus [26]. However, following research pointed out that stenosing ECU tenosynovitis may occur in the more distal area than in the ulnar groove because of thicker collagen fibers in the distal extension of the ECU subsheath and that it is believed to be painful during the patient’s forearm pronation [5]. We strongly agree the main position of the stenosis would be located at the distal area. All sonographic findings of ECU tendinopathy in our study covered the area without an osseous floor under the ECU. The current study results showed lower sensitivity and positive predictive values of the ECU synergy test in contrast with the previous study, where they were 74% and 82%, respectively, in patients with dorsal ulnar-sided wrist pain lasting more than two weeks [16]. We speculate this might be due to the difference in diagnostic and patients inclusion criteria. We did not consider the patient had a constrained ECU tendinopathy if sonography showed sole ECU tendon sheath distension without blood flow, and the test might be falsely positive in many patients because we included acute phase patients whose pain was severe.
Ulnar variance and radial length have been mainly reported in line with the assessment of Kienbock disease and distal radius fracture [20, 21, 27-30]. Given that the ECU tendon runs on the surface of the ulnar head, we investigated if there was any hint in the radiographic measurements representing a distal radio-ulnar relationship for constrained ECU tendinopathy. Although the results did not show any significant difference between the two groups of dorsal ulnar-sided wrist pain, the mean values for radial length and rotational width of DRUJ were slightly lower in the group with constrained tendinopathy. We infer that this might be due to the dominant number of female patients.
This study has several limitations. First, we only assessed the sixth dorsal extensor compartment and did not precisely examine the deep ulnar-sided wrist anatomy. Considering ECU tendinopathy frequently has concomitant pathology in the ulnocarpal joint and/or DRUJ as previous authors describe [6, 31], it is ideal that our patients’ symptoms should be comprehensively understood combined with the results of wrist arthroscopy and MRI. Second, the presence or absence of a sixth compartment septum and accessory ECU tendon slip were not taken into consideration in this study because of the difficulty in confirming them by sonography, although these findings have been pointed out as potential causes of ECU tendinopathy [5, 25]. Third, the same person performed all sonographic and physical examinations and radiographic measurements. We did not blind the sonographer and radiographic measurer to the result of the ECU synergy test or ultrasonography. The result of this study contains substantial bias arising from this limitation.
CONCLUSION
In conclusion, the results of our investigation showed that more middle-aged to elderly women and fewer sports-related patients tend to contract constrained ECU tendinopathy. Those tendencies might imply that constrained ECU tendinopathy should be considered degenerative stenosing synovitis similarly to such as de Quervain`s disease. Physicians should be aware that we can encounter this disease more often than we may expect if we face vague ulnar-sided wrist pain as well as that ultrasonography is a mandatory and easily available imaging modality to confirm this condition.
LIST OF ABBREVIATIONS
| ECU | = Extensor carpi ulnaris |
| TFCC | = Triangular fibrocartilage complex |
| DRUJ | = Distal radioulnar joint |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by Institutional Review Board and Ethics committee in our clinic (the Research Board of Healthcare Corporation Ashinokai, Gyoda, Saitama, Japan (ID number: 2015-5).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants of this study.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
STANDARDS OF REPORTING
STROBE guidelines were used.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

