All published articles of this journal are available on ScienceDirect.

Full Endoscopic Discectomy Using Transforaminal Endoscopic Spine System Technique: A Mini Review of Complications
Authors Info & Affiliations
Abstract
Background:
Full Endoscopic Discectomy (FED) is a minimally invasive technique for the treatment of Lumbar Disk Herniation (LDH) with increasing popularity among surgeons in the recent years. This alternative to conventional procedures surgical approach is generally a safe and efficient technique possessing many advantages such as less soft tissue trauma, preservation of dorsal musculature, and reduced perioperative morbidity and rapid recovery. However, FED is associated with a number of complications such as postoperative dysesthesia, nerve root injury, and dural tears.
Methods:
Α search of PubMed, Google Scholar and Scopus electronic databases was used to revised the literature on complications of full endoscopic discectomy using transforaminal endoscopic spine system technique
Conclusion:
In this review complications associated with FED are analyzed, emphasizing on the potential beneficial role of Transforaminal Endoscopic Spine System (TESSYS) technique in reducing their frequency.
1. INTRODUCTION
Lumbar Disc Herniation (LDH) is one of the most common spine pathologies with a worldwide distribution [1] characterized mainly by low back pain (LBP) and sciatica. First line therapeutic approach includes conservative treatment with analgesics and physical therapy. Refractory cases may warrant surgical intervention [2]. The main indication for surgical treatment is persistent symptomatology over 3 months of conservative therapy. Surgical intervention offers more rapid pain relief, compared to conservative management [3].
Microdiscectomy is considered to be the gold standard method for the treatment of LDH. However, the evolution in spine surgery has led to more minimally invasive techniques such as full endoscopic discectomy (FED). This is a fairly new minimally invasive technique, introduced in the recent years, that gains ground among spine surgeons universally [4]. According to medical literature, FED using Transforaminal Endoscopic Spine System (TESSYS) technique is associated with less soft tissue trauma and paraspinal muscles injury, reduced blood loss, shorter hospital stay, less cost of hospitalization and earlier return to daily activities [5, 6]. In a recent study Kapetanakis et al. investigated health-related quality of life after FED using TESSYS technique, showing a significant postoperative improvement [4].
It has been proposed that FED using TESSYS technique presents fewer complications compared to other minimal invasive techniques [7]. More specifically, the rate of complications ranges from 2,7-3,5% in the published literature [8]. These complications include incomplete decompression and recurrent disc herniation, postoperative dysesthesia, nerve root injury and dural tears, hematoma, infection and abdominal visceral injury [9-11].
The aim of this article is to analyze complications associated with FED, emphasizing on the potential beneficial role of TESSYS technique in reducing their frequency. Spine surgeons should be familiar with and capable of promptly recognizing these complications, in order to improve outcomes.
2. MATERIALS AND METHODS
In this review a research of the existing medical literature during last 20 years in the English language about complications following FED for LDH was carried out. More specifically for the purpose of this mini review, a literature search of PubMed, Google Scholar and Scopus electronic databases was performed using the Medical Subject Headings (MeSH) «full endoscopic discectomy», «microdiscectomy», «minimally invasive spine surgery», «low back pain», and «lumbar disc herniation» alone or in combination with the others as keywords. All Randomized Control Trials (RCTs) including more than 20 adult patients who underwent FED or microdiscectomy for lumbar disc herniation and adequate data provided in term of complications. Experimental studies, case reports and case series as well as manuscripts in language other than English, were not included in this study. Search results yielded 15 RCTs which met the inclusion criteria set for the purpose of the present study.
3. RESULTS
Full endoscopic discectomy is considered as a safe and efficient minimally invasive technique for the treatment of lumbar disk herniation. However, this modern technique is accompanied with a number of complications such as postoperative dysesthesia, nerve root injury, dural tears, postoperative hematoma, infection, vascular damage, abdominal visceral injury and recurrence of intevertebral disc herniation (Table 1).
Liu X et al. conducted a study including a total of 60 patients who underwent FED for far-lateral and foraminal disc herniations and found the recurrence rate to be as high as 5,5% and the persistent strong LBP to range up to 3,7% [15]. In another study Gu et al. evaluated the safety of FED in elderly patients over 65 years old. Complications were presented only in 3 patients and included dural tear, postoperative dysesthesia due to nerve root injury and recurrence disc herniation [16]. Chen et al. accomplished an ongoing randomized controlled trial in 153 participants who suffered from lumbar disk herniation. These patients were randomly allocated in two groups who received FED and microendoscopic discectomy (MED) respectively. During 1 year of follow up, the total complication rate of FED was 13.75%. Dural tear, nerve root injury, transient dysesthesia and re-herniation were the most common complications with a percentage of 1.25%, 3.75%, 2.5% and 6.25% respectively. In this study, risk factors that led to reoperation after discectomy were also noted. These included old age, high- grade lumbar degeneration, modic changes and adjacent segment degeneration [13].
In 209 patients, FED was performed by Gu et al. who recorded postoperative complications in 5 of them. Three patients complained of increased weakness of quadriceps or foot extensor. Eight months after surgery, recurrence occurred in one patient [17]. Gotecha et al. investigated the morbidity and was found in one other patient. Re-herniation of the intervertebral disc was also noted in 6 cases [18]. Wu et al. emphasized on the difficulty of approach of L5-S1 level using FED. They stated that the presence of a high iliac crest, large L5 transverse process, large face joints and narrow foramen pose anatomic restrictions to this surgical approach. In fact at L5-S1 level, the rate of complications is increased [19].
The favorable outcomes of FED using TESSYS technique, at levels of L2- L3, L3- L4, L4- L5, especially for beginner spine surgeons were mentioned by Kapetanakis et al. The authors of this study underline that transforaminal approach at L5-S1 level remains controversial due to deep and steep iliac crests along with the narrow interlaminal space [2]. Ahn et al. investigated the clinical data of 45 patients, who underwent FED. A total of 9 patients presented with complications after FED such as poor outcome and the need for urgent open surgery, incomplete decompression, recurrent herniation, dural tear and transient dysesthesia [20]. Complications following FED mentioned in 295 cases in a RCT by Kim et al. In this study, the rate of recurrent intervertebral disc was recorded equal to 6.44%. More specifically, five patients appeared with incomplete decompression, two patients experienced spondylodiscitis and three patients developed a dural tear. In order to decrease the risk of these complications a detailed assessment of preoperative CT images and the knowledge of anatomical relationships and several variations is recommended [21].
Schubert and Hoogland analyzed the benefits of FED in a study with two years follow- up. This research included a total number of 558 patients and the recurrence rate was 3.6% [22]. In a study including 100 patients, Mahesha reported the advantages of FED and investigated postoperative complications. In this study the rate of recurrent disc herniation was calculated at almost 2% [6]. Interestingly, a quite rare case of a symptomatic post-discectomy pseudocyst after FED was mentioned in the literature, diagnosed at a two-months’ postoperative period12. Finally, postoperative seizures attributed to the increased epidural pressure which can lead to increased intracranial pressure, is another rare complication reported after FED [23].
The variety of complications associated with FED for LDH reported in the medical literature as is collectively presented in Table 2. A short description, as well, of complications of microdiscectomy reported in papers published last years, is analyzed in Table 3 in order to emphasize the superiority of FED using TESSYS technique.
4. DISCUSSION
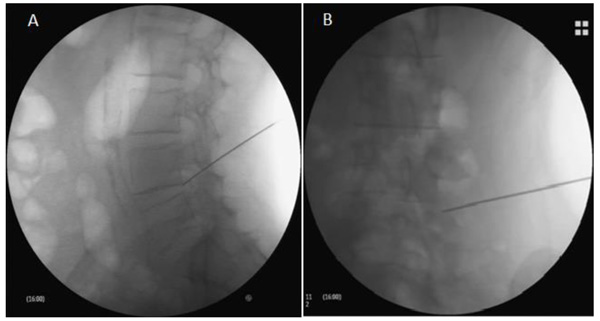
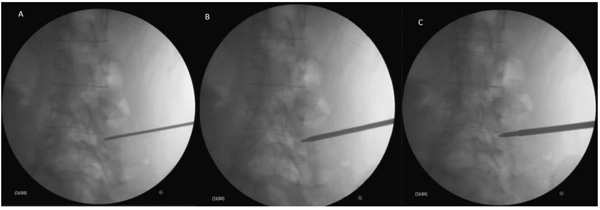
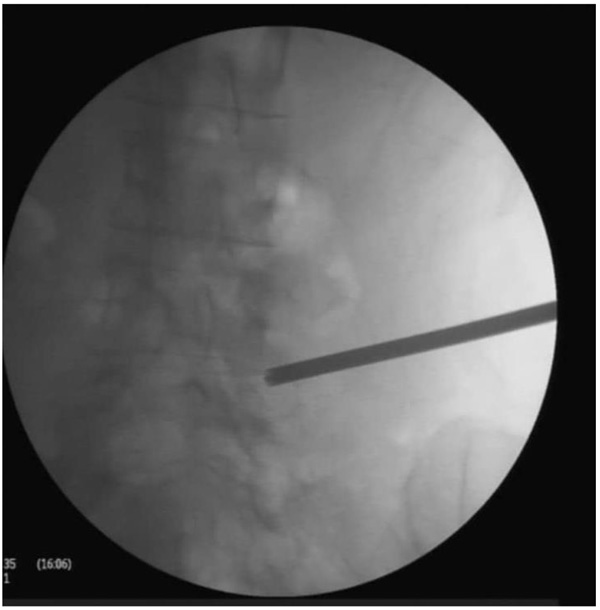
FED using TESSYS is a minimally invasive technique in spine surgery that is performed under local anesthesia and mild sedation [29]. Patients are positioned in the lateral decubitus position, lying down on the opposite side, in order to achieve the optimal enlargement of the foraminal space. The next step is the disinfection of the surgical field. Subsequently, local anesthetic is applied at the point of entrance of the needle, which provided access to the foramen. Needle is initially 11cm laterally of the midline introduced, with the transit corridor leading to Kambin’s triangle. Fluoroscopic guidance is uninterruptedly performed during needle promotion, so that correct position can be validated (Fig. 1) Analgesia using fentanyl ampule and mild sedation are subsequently provided, followed by the sequential passage of specific reamers (Fig. 2). Reamers diameters 5.5, 6.5 and 7.5 respectively (Joimax System) are utilized. Cannula and endoscope are finally introduced (Fig. 3), and herniated disc material is removed by graspers (Fig. 4).
According to the literature, FED is a safe surgical procedure with low rate of complications, that range from 2,7% to 3,5% [8]. Complications of FED include postoperative dysesthesia, nerve root injury, dural tears, postoperative hematoma, infection, vascular damage, abdominal visceral injury and recurrence disc herniation [7, 8, 12, 30-34] (Table 1). It is worth mentioning that although patients are discharged on the first postoperative day, the presence of complications may prolong the rehabilitating period.
The most common complication of FED is the injury of the nerve root and the dorsal root ganglion, with an estimated incidence of 1-8,9% [32]. Postoperative dysesthesia constitutes the main clinical sign of this nerve damage. Nerve impairment is considered to be caused by two potential mechanisms [33, 35]. Firstly, the exiting nerve root can be compressed by the cannula of the endoscope during its entrance through the intervertebral foramen. In order to overcome this obstacle, foraminoplasty may aid to enlarge the intervertebral foramen [36]. This method was successfully performed in order to insert the cannula safely, securing the nerve root. A second proposed mechanism is the direct injury by the cannula, during lidocaine infiltration of the exiting nerve root. In that case, dysesthesia or motor paresis occur early in the postoperative period [36]. Generally, the clinical sign of postoperative dysesthesia constitutes a key point to recognize any damage of nerve root [37].
Durotomy is another serious complication associated with FED [13, 38]. Inappropriate usage of surgical tools may cause dural tears33. In addition to this, thermal injury can similarly cause dural lesions. Dural traumatic lesions are associated with serious neurological complications [32]. These symptoms include nausea, vomiting, postural headache, photophobia and back pain [11]. Especially, dural tears can cause cerebrospinal fluid (CSF) leakage, leading to serious problems such as CSF fistula formation, meningitis, arachnoiditis, pseudomeningocele and epidural abscess [39]. Fortunately in the last decades, the prevalence of dural tears was decreased due to the increasing experience of spine surgeons, when performing minimal invasive techniques such as FED. All authors conclude that the key point is the prevention and the immediate recognition and treatment, in order to avoid the long-term sequelae of dural tears [40].

| Authors | Year | No of patients | Comments |
|---|---|---|---|
| Liu X et al. [15] | 2018 | 60 | Recurrence rate: 5,5% Persistent strong LBP: 3,7% |
| Gu et al. [16] | 2018 | 25 | Patients over 65 years old Dural [tear: 1 patient Postoperative dysesthesia: 1 patient Recurrence: 1 patient |
| Chen et al. [13] | 2018 | 153 | Complication rate: 13,75% Dural tear: 1,25% Nerve root injury: 3,75% Transient dysesthesia: 2,5% Recurrence rate: 6,25% |
| Gu et al. [17] | 2017 | 209 | Increased weakness of quadriceps or foot/toe extensor strength: 1,4% Low toxicity infection of disc: 0,5% Recurrence rate: 0,5% |
| Kapetanakis et al. [2] | 2017 | 76 | Without complications |
| Mahesha K [6]. | 2017 | 100 | Recurrence rate: 2% |
| Gotecha et al. [18] | 2016 | 120 | Spondylodiscitis: 2 patients Dysesthesia: 1 patient Recurrence: 6 patients |
| Ahn et al. [20] | 2009 | 45 | Poor outcome and reoperation: 4 patients Incomplete decompression: 2 patients Dural tear with motor weakness: 1 patient Transient Dysesthesia: 3 patients Recurrence: 1 patient |
| Kim et al. [21] | 2007 | 295 | Spondylodiscitis: 2 patients Incomplete decompression: 5 patients Dural tear: 3 patients Recurrence rate: 6,44% |
| Schubert M. and Hoogland T [22]. | 2005 | 558 | Recurrence rate: 3,6% |
| Authors | Year | No of patients | Follow up (months) | Comments |
|---|---|---|---|---|
| Ahmadi et al. [24] | 2018 | 320 | 48 | • Dural tear: 3,2% • Surgical site infection: 1,64% • Hemorrhage: 0.66% • Required additional surgery: 26,7% • Recurrence rate: 18,9% |
| Schmid et al. [25] | 2016 | 275 | 12/54 | • Reoperation rate at 12 months: 8,7% • Reoperation rate at 54 months: 11,3% • Dural tear: 4,4% • Wound infection: 3,3% |
| Tsutsumimoto et al. [26] | 2014 | 555 | 6 | • Dural tears: 5,05% |
| Wang et al. [27] | 2012 | 151 | 120 | • Recurrence rate: 3,5% • Intraoperative dural lacerations: 3,5% • Spondylodiscitis: 2,1% |
| Casal - Moro et al. [28] | 2011 | 120 | 60 | • Durotomy: 4,1% • 9 patients underwent subsequent lumbar surgery • L5 paresis: 3 patients • Discitis: 1patient • Deep vein thrombosis: 1 patient |
Incomplete decompression occurs due to the appearance of a missed fragment of herniated disc or the presence of a lateral recess stenosis compressing the nerve root [10]. The intrinsic difficulties of FED as a method, in relation to the absence of experience by spine surgeons can lead to incomplete decompression [41]. Most cases concern a migrated disc herniation or a large central disc herniation that occupies a significant part of the spinal canal [33]. The appropriate way to avoid this complication is the sufficient knowledge of clinical anatomy, especially for the inexperienced spine surgeon. After a pain-free period, the main problem is the re-herniation of the intervertebral disc [18]. The recurrence rate is similar to that of microdiscectomy and it ranges from 3 to 7% [12]. The period of recurrence ranges from 3 to 18 months after the performance of spine surgery [10, 18, 42] The complete and careful removal of the hernia mass constitutes the optimum condition to reduce the probability of recurrence [33].
Infection following microdiscectomy is one of the most common complications. On the contrary, postoperative spondylodiscitis is a relatively rare complication in FED compared to traditional open procedures [33]. The clinical presentation of spondylodiscitis includes back pain and leg pain several days after the surgical procedure. Furthermore, inflammatory markers such as C- reactive protein, erythrocyte sedimentation rate and leucocyte count are elevated. Magnetic Resonance Imaging (MRI) is the most specific method for radiological diagnosis of spondylodiscitis [43]. Disc punctures and tissue culture may prove necessary for the definitive bacteriological diagnosis. In case of this undesirable event, treatment of spondylodiscitis aims to eradicate the focus of infection, restore spinal functionality and relieve pain. Pharmaceutical therapy with combined antibiotics and analgesics is the gold standard therapeutic approach [44].
A rare complication of FED is the injury of vascular structures anterior to the disc, which can lead to creation of hematoma [45]. The radicular lumbar artery or its branches are the most vulnerable points during the transforaminal approach [46]. Usually, the postoperative hemorrhage is less than 5 ml (<1-5 ml) [11]. In rare cases of major hemorrhage, radicular symptoms can be present. When a large retroperitoneal hematoma (>500 ml) is present, an urgent surgical evacuation is of paramount importance in order to avoid unpleasant consequences [34]. Another possible vascular event, the postoperative epidural hematoma is subclinical and self- limiting in the majority of cases and may also be noticed after FED [47]. Intraoperative angiography is a valuable invasive method, depicting and locating a possible damage of vascular system which can be treated by coil embolization [33].
Abdominal visceral injury due to FED is another relatively rare complication. Nevertheless, during the entrance of the needle, an inappropriate approach can cause the injury of the visceral peritoneum or the bowel [32]. Finally a rare albeit serious complication of FED is the traumatization of kidneys during the passage of the reamers and the cannula [31, 33]. This adverse outcome is associated with high level LDHs such as T12-L1, L1-L2 and L2-L3. In order to avoid such serious complications novice spine surgeons need to know and recognize the anatomical relationships and abnormal variations [41].
CONCLUSION
FED is a safe minimally invasive technique in spine surgery. Advantages of FED comprise the integrity of paraspinal muscles, less soft tissue trauma, reduced perioperative blood loss, short hospital stay, less cost of hospitalization and early return to work and daily activities. Despite the existence of several advantages, a number of complications are mentioned in the published literature. The most common complications include incomplete decompression, re-herniation of intervertebral disc, postoperative dysesthesia, nerve root injury and durotomy, hematoma or hemorrhage, infection (spondylodiscitis) and abdominal visceral injury. Nevertheless, the overall rate of complications associated with FED is relatively low. The usage of TESSYS technique can lead to the reduction of devastating complications. Prevention is the key point to restrict the frequency of complications. In addition to this, the knowledge of anatomical relationships and the immediate recognition of complications aids to the optimal surgical management.
LIST OF ABBREVIATIONS
| FED | = Full Endoscopic Dictectomy |
| LDH | = Lumbar Disc Herniation |
| TESSYS | = Transforaminal Endoscopic Spine System |
CONSENT FOR PUBLICATION
Not applicable.
CONFLICT OF INTEREST
Dr. Kapetanakis is a reference doctor for joimax® GmbH and receives payments for teaching. The other authors declare that they have no conflict of interests.
ACKNOWLEDGEMENTS
Declared none.

