All published articles of this journal are available on ScienceDirect.

A Rare Case of Acute Carpal Tunnel Syndrome Secondary to Calcific Tendinitis: A Case Report
Abstract
Acute carpal tunnel syndrome secondary to acute calcific tendinitis is a rarely reported entity and poses a diagnostic dilemma for clinicians due to its non-specific presenting symptoms. Urgent decompression of the carpal tunnel is required to preserve the median nerve. We describe a case of acute carpal tunnel syndrome in the dominant hand of a 66-year-old female patient secondary to calcific tendinitis. Decompression was performed with good clinical result. We present this case report in order to further the knowledge bank regarding acute calcific tendinitis to help future clinicians to identify and manage it.
1. INTRODUCTION
Acute Calcific Tendinitis (ACT) is a well-known condition of the shoulder but a relatively uncommon disorder of the hand and wrist. It is an idiopathic inflammatory condition frequently affecting the small joints and tendons of the upper limb however it is infrequently noted to involve the carpal tunnel.
Acute Carpal Tunnel Syndrome (CTS) has been described secondary to multiple different aetiologies, however there are few reported cases of CTS secondary to ACT. These cases pose a diagnostic dilemma for clinicians due to the non-specific presenting symptoms of ACT and the sparsity of information about the condition. Whilst ACT is typically treated conservatively, acute CTS requires urgent decompression of the carpal tunnel to preserve the median nerve.
We describe a case of acute CTS in the dominant hand of a 66-year-old female secondary to ACT. We present this case report to add to the knowledge bank regarding ACT to help future clinicians identify and manage it appropriately without delay in diagnosis.
2. CASE REPORT
A 66-year-old female presented to the Emergency Department with a five-day history of increasing pain and swelling in her dominant hand. She described the pain as severe and stated that it had begun around the thenar eminence and progressed to include her entire hand and wrist. She also complained of “pins and needles” and altered sensation to the entire volar surface of her hand, but worst in her thumb, and index and middle fingers. She denied any trauma and was systemically well. She had no significant medical history other than an endoscopic carpal tunnel release performed many years prior with full resolution of symptoms. The patient worked as a “lollipop lady” at a school pedestrian crossing.
Upon examination, she was afebrile and did not appear unwell. There was gross swelling both to the dorsal and volar aspects of her wrist and hand, worst around the midpalmar space. There was no erythema and the skin was only mildly warm to touch. Her wrist and finger active range of movement were decreased but she was able to passively range her fingers. Tinel’s sign was not positive at this time.
A venous blood sample and plain radiographs of the hand were obtained. Routine laboratory blood test demonstrated a mild leucocytosis (WCC 12,800/mm3) with neutrophilia (9,390/mm3), ESR of 55 and a CRP of 123. Blood biochemistry was unremarkable. Plain x-ray demonstrated degenerative changes and subtle calcification in the midpalmar area (Fig. 1).
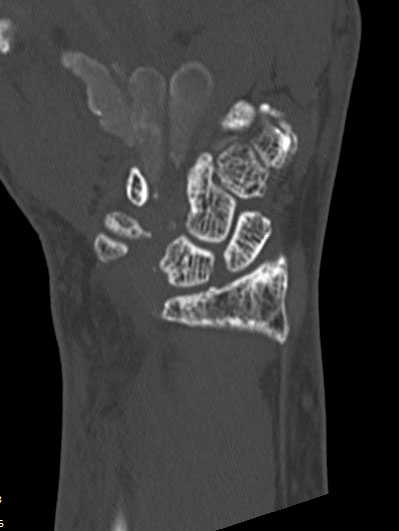
At the time of admission, infection could not be excluded as the cause of the patients' symptoms. She was commenced on intravenous antibiotics, Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), and the affected arm was elevated in gallows sling. Ultrasound of the region was performed the following day to assess for collection and/or flexor tenosynovitis. Ultrasound demonstrated generalised subcutaneous oedema with

fluid in the carpal tunnel; no discrete collections were observed. CT was performed and confirmed extensive calcification within all tendon sheaths of the carpal tunnel extending distally into the palm (Fig. 2). MRI was performed and demonstrated a T1 and T2 isointense rim enhancing collection measuring 10mm in depth, 31mm in transverse dimensions and tracking along the flexor tendons of the 1-4 fingers over a length of 30mm (Fig. 3).
The patient developed progression of sensory changes in the median nerve distribution and became Tinel’s and Phalen’s test positive within 48 hours of admission. Unfortunately, neurodiagnostic testing is not available at our hospital so we were not able to perform Nerve Conduction Studies (NCS) or Electromyography (EMG) to confirm our clinical diagnosis of acute CTS and assess the degree of median nerve involvement and level of function. The patient was taken to theatre for carpal tunnel release and exploration under general anaesthetic. Upon decompression, a large volume of viscous white liquid with hard fragments was expressed (Fig. (4). The fluid was sent for gram stain, culture and biochemistry. Extensive synovitis was noted within the carpal tunnel, which was debrided and sent for microbiology and histology sampling. The median nerve was noted to be extremely inflamed and compressed within the palm. The wound was thoroughly washed, haemostasis achieved, and the skin closed.
The fluid and tissue samples sent to pathology at the time of surgery all returned negative results for infection (negative gram stain, no growth on culture, negative 16s rRNA Gene NAA), and crystal arthropathy (no crystals). Fluid samples demonstrated calcium-rich inflammatory fluid. Histology of synovial tissue demonstrated significant dystrophic calcification with no evidence of neoplasm. The patient was placed in a thermoplastic resting splint postoperatively and commenced gentle active exercises with hand occupational therapy. She noted a significant improvement in pain and a slight improvement in sensation postoperatively and was discharged day three post surgery. Ongoing outpatient review has shown a marked improvement in pain and range of movement, however, the patient still has mildly altered sensation in the median nerve distribution (significantly better than prior to her open decompression and exploration). This is thought to be due to possible irreparable median nerve damage due to the delay in presentation and thus delay to decompression.


3. DISCUSSION
ACT of the wrist is an idiopathic inflammatory condition with a high rate of misdiagnosis due to both its rarity and its similar clinical presentation to infectious or inflammatory conditions. It has often been confused for fracture, septic arthritis, tenosynovitis and crystal deposition disorders [1-4]. ACT has been observed to occur at many of the small joints of the hand and wrist, to involve both the flexor and extensor tendons, and most commonly affect the insertion of Flexor Carpi Ulnaris at the pisiform [2].
The pathogenesis of ACT is poorly understood. It has been hypothesised that the calcification occurs as a result of local tissue hypoxia, chronic inflammation, or from repeated microtrauma [2]. Cooper hypothesised that ACT occurs in areas secondary to deficient blood supply; this hypothesis was supported by his observations of microscopic lesions and degenerative changes in the blood vessels demonstrating hypertrophy of the tunica media and narrowing of the lumen within the affected areas [5]. It has also been hypothesised that microtrauma may induce an area of tissue necrosis into which calcium is deposited [2, 5, 6].
Carroll et al. described a series of 100 consecutive cases of ACT of the hand and wrist. They noted that the condition was most prevalent in patients between the ages of 30 and 60. The main presenting complaint of patients in their series was a pain. None of their patients presented with acute CTS. Patients with ACT more commonly presented with involvement of the dominant hand [1, 3, 7, 8] possibly due to repeated subclinical trauma. Females are more frequently affected than males [1, 7, 8] and most patients are of an older age, which may be due to metabolic factors [2, 7].
ACT frequently presents suddenly without any precipitating incident in a single site, with associated localised severe pain and incapacitation [2, 9]. Patients usually have associated swelling, warmth and erythema to the area [1]. Patients presenting with ACT may be afebrile or have low-grade fevers [10]. The symptoms of ACT are thought not to be a result of the calcification itself but rather due to the rupture of a calcific deposit into the adjacent soft tissue resulting in an acute inflammatory response [2, 9].
Diagnosis of ACT in the hand and wrist is challenging due to its presentation which commonly resembles infection or inflammatory disease. Serologic testing is generally not helpful in making the diagnosis [9], however inflammatory markers mildly elevated but well below the levels associated with infection. Radiographic diagnosis is also difficult as calcium deposits may be extremely small, and special views may be necessary. Often the diagnosis is only made at the time of surgical exploration [2, 9].
ACT of the hand and wrist without median nerve compression may be treated with immobilisation in combination with aspirin or NSAIDs. This may shorten the duration of symptoms to 7-10 days [9]. Radiation and surgical evacuation were previously advocated for ACT management, however, are no longer recommended. Corticosteroid injection, colchicine, and prednisone have also been used for ACT treatment with some success [11]. Calcifications observed on radiographs will tend to reabsorb and disappear from repeat imaging over the course of several weeks [3]. As the symptoms of ACT are difficult to distinguish from infection, this may prompt unnecessary surgical exploration in the setting of symptoms not resolving with antibiotics [7]. Hence, there is a need for further awareness of this condition amongst clinicians.
Whilst CTS and calcific tendinitis of the wrist are both well recognised individual entities, only a few instances of acute CTS secondary to ACT have been described [7, 9, 12]. A gradual accumulation of calcium within the carpal tunnel typically leads to slow median nerve compression and progression of CTS, however acute presentation can occasionally occur. Whilst most authors describe ACT in the hand as a self-limiting disease with spontaneous resolution within weeks, when the condition presents with acute CTS, urgent decompression is required [2, 7, 13]. Decompression prevents irreparable intraneural fibrosis development secondary to prolonged median nerve compression [14]. Timely decompression of the median nerve results in good clinical recovery [14]. An extensive incision is required for complete median nerve decompression and better visualisation and debridement of flexor tendons and synovitis [7].
In the case of our patient, we suspect that the calcium deposition within the carpal tunnel was a gradual process over many years (as evidenced by the radiographic changes). The instigating factor for calcium deposition in that area may possibly have been the endoscopic carpal tunnel release, performed years prior to this presentation. We believe that a minor trauma to the area resulted in rupture of a previously contained calcium deposit and thus the rapid onset of symptoms and her acute presentation. We suspect that she now has a degree of residual median nerve intraneural fibrosis resulting in sensory symptoms; whilst these pathologic changes may be longstanding given her history of chronic CTS and endoscopic release, we hypothesise that it is from the ACT since she had been asymptomatic (in both median nerve sensory and motor function) following endoscopic surgery. Had decompression surgery been more expedient, we believe the patient may have returned to her previous full level of motor and sensory function.
CONCLUSION
We present this case to further the knowledge bank regarding ACT leading to acute CTS to hopefully assist future clinicians with this diagnostic dilemma. The authors concur with current evidence that management of uncomplicated ACT should be conservative symptomatic management (elevation, rest, NSAIDs), however, in a case such as ours, we advocate for early decompression of the compromised nerve to preserve function and minimise complications. We believe that the diagnosis had been made sooner, the patient would have had her median nerve decompressed faster and may have returned to full motor and sensory function.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Informed patients consent was obtained for this study.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

