All published articles of this journal are available on ScienceDirect.

Highly Cross-linked Polyethylene Liner Dissociation from a Cement-less Modular Acetabular Shell: Two Case Reports
Abstract
Liner dissociation of polyethylene from a cementless acetabular socket following total hip arthroplasty (THA) is a rare complication. Cross-linked polyethylene liner dissociation from AMS-HA shell (KYOCERA Med, Osaka, Japan) occurred in 2 out of the 4153 (0.04%) cases approximately 10 years after undergoing surgery at our institute. First case was an 80-year-old female who underwent right THA along with subtrochanteric femoral shortening osteotomy due to complete dislocation hip, and second case was a 72-year-old male, who underwent right THA due to coxarthrosis. A 26 mm femoral head and CPE liner were used in both cases and the inclination degree of the acetabular socket was within 50°.There was no implant loosening in both cases. There was partial damage in the elevated rim on the alternative side and scratches on the back side in the both extracted CPE liner. It was surmised that liner dissociation was caused due to a problem in the liner fixing format of the push in type of the present model.
INTRODUCTION
Complications of total hip arthroplasty (THA) include dislocation, infection, nerve/vascular injury, thrombus, embolisms, damage, loosening, etc. Although polyethylene (PE) liner dissociation from a cementless acetabular socket is not a highly frequently observed complication, it has been reported in particular models such as Harris-Galante cementless prostheses (Zimmer, Warsaw, Ind), etc. [1 - 7]. Further, liner dissociation from the acetabular socket is also observed in Hard-on-hard THA using a sandwich-type liner [8 - 14]. Particularly regarding AMS-HA acetabular shells with an Alumina-Bearing-Surface (ABS) liner (KYOCERA Med, Osaka, Japan), there have been several reports on dissociation of the sandwich-type ceramic liner [10, 11, 14], and according to post-marketing surveillance, dissociation of ABS liners has occurred in 649 among 3933 hips (16.5%). PE liners may be selected for AMS-HA acetabular shells; however, there are no reports on liner dissociation when PE liner is used in combination with an AMS-HA acetabular shell.
To our knowledge, this is the first reported case of dissociation of the PE liner from an AMS-HA shell. This report concerns the mechanism of dissociation of PE liner from AMS-HA shell.
The study protocol adhered to the ethical guidelines of the 1975 Declaration of Helsinki, and the institutional review board of the Faculty of Medicine, Saga University at Saga, approved this study. The patients were informed that this case study would be submitted for publication, and they gave their informed consent.
CASES
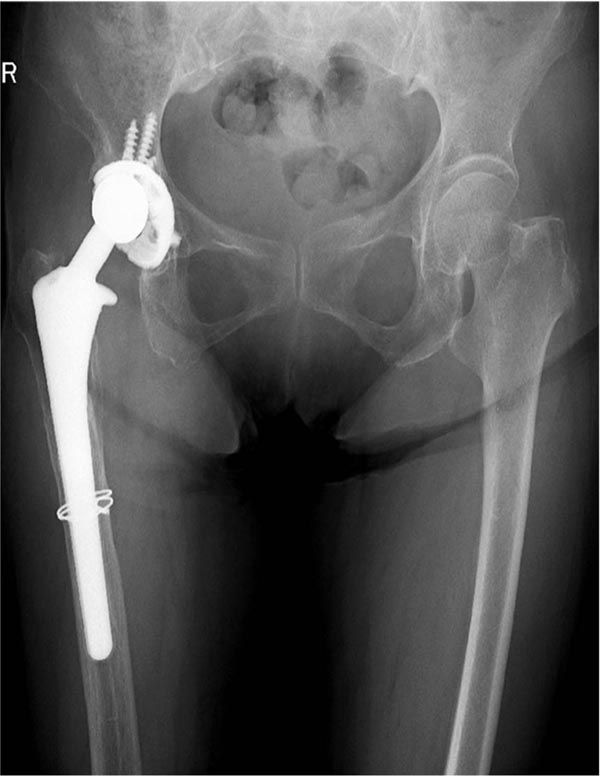
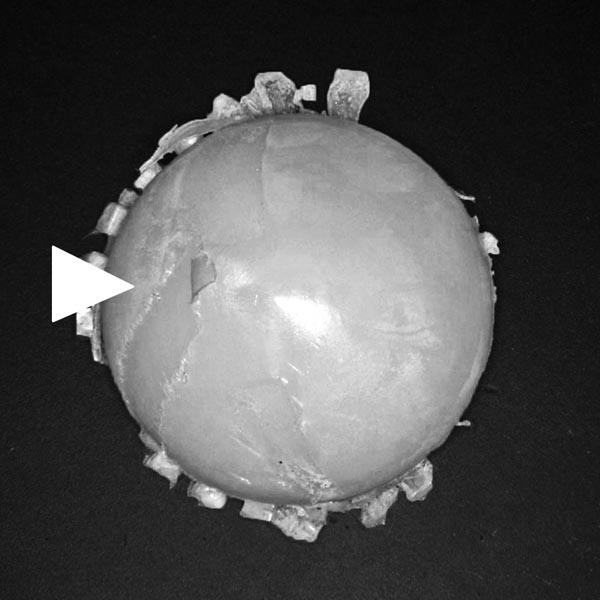
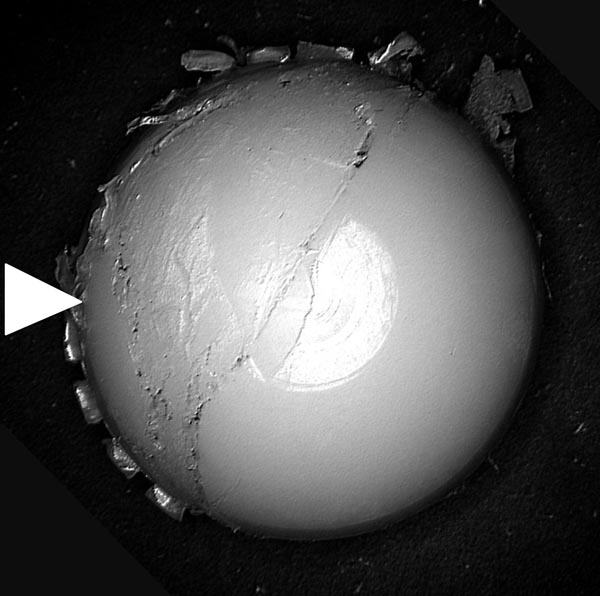
Case 1 pertains to an 80-year-old woman. She underwent right THA along with subtrochanteric femoral shortening osteotomy taking a posterolateral approach using methods by Hotokebuchi et al. [15] under a diagnosis of complete dislocation hip. An AMS-HA acetabular shell (outer diameter 44mm, inner diameter 38mm) with a cross-linked polyethylene (XLPE) liner was set in the acetabulum with four screws and a cementless proximal-hydroxyappatite-coated femoral component (a PerFix-HA #13-M stem) was used along with a 26 mm zirconia ball (Kyocera Medical, Osaka, Japan). An AMS-HA acetabular shell is a push in type liner fixing format for gripping the groove of a liner with four clicks, having a structure whereby rotatable fixation contributes to one section (Fig. 1). Regarding the XLPE liner, a calcium-stearate-free GUR 1050 ultra-high-molecular-weight PE resin was used to create a compression-molded sheet stock, which was then machined into the final implant geometry. Prior to machining, the compression-molded sheet was subjected to a process consisting of gamma-ray irradiation of 35 kGy in air to achieve the desired level of cross-linking and then annealed at 110 °C for 12 h in nitrogen to reduce the concentration of free radicals. After machining, the liners were sterilized with 25-kGy gamma-ray irradiation in nitrogen (total 60 kGy) and prepared [16, 17]. The gamma-ray irradiation amount of 60 kGy in total is similar to that reported in most previous studies using XLPE [18]. The inclination angle of the socket was 48 degrees, the anteversion angle was 26 degrees, the vertical distance from the tear drop to the center of the femoral head was 17 mm, and the horizontal distance was 22 mm. No problems were observed until 9 years following surgery (Fig. 2a); however, an aching pain and abnormal sound occurred in the right hip joint after 9 years and 8 months. A plain X-ray revealed that the right femoral head had deviated to the outer upper side of the acetabular socket; however, osteolysis was not observed in the vicinity of the acetabulum and femoral implant (Fig. 2b). Upon Surgery, the XLPE liner had dissociated inwards and downwards from the acetabular socket; however, no problems were observed in the four clicks, which is the liner gripping mechanism of the acetabular socket, with no looseness. Fixation of the femoral component was good with no macroscopic observation of the trunnion, and so revision surgery on the liner was conducted and the ball was exchanged. The extracted XLPE liner was observed with partial damage in the elevated rim on the alternative side and end section surface along with scratches on the back side (Figs. 2c and 2d, Table 1).

| Alternative side | Back side | |||
|---|---|---|---|---|
| Anterior side | Posterior side | Anterior side | Posterior side | |
| Case 1 | Surface of the end face is crushed due to friction with the stem neck following dissociation, which is believed to have caused exfoliation in some areas | Partial damage to the elevate rim and end face surface | Partial scratches from the click of the shell in the upper center | Belt-like scratch marks caused by the click of the shell occurring in the process leading to dissociation |
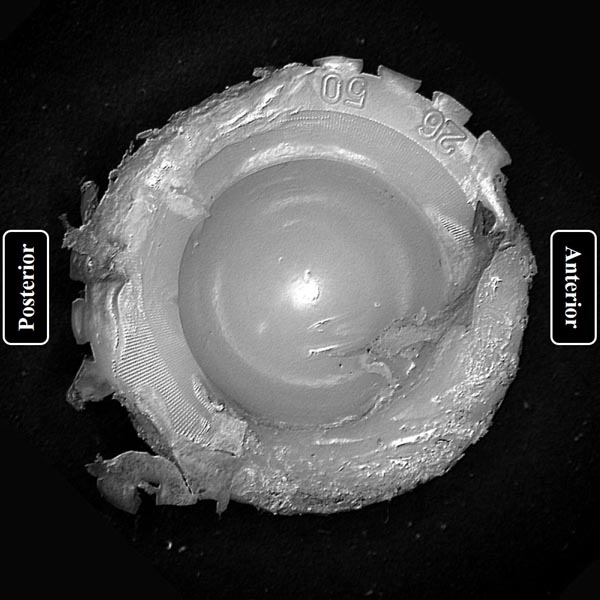
| Case 2 | Surface of the end face is crushed due to friction with the stem neck following dissociation, which is believed to have caused exfoliation in some areas | Partial damage to the elevate rim and end face surface | Partial scratches from the click of the shell in the lower center | Scratch marks throughout a large area caused by the click of the shell occurring in the process leading to dissociation |


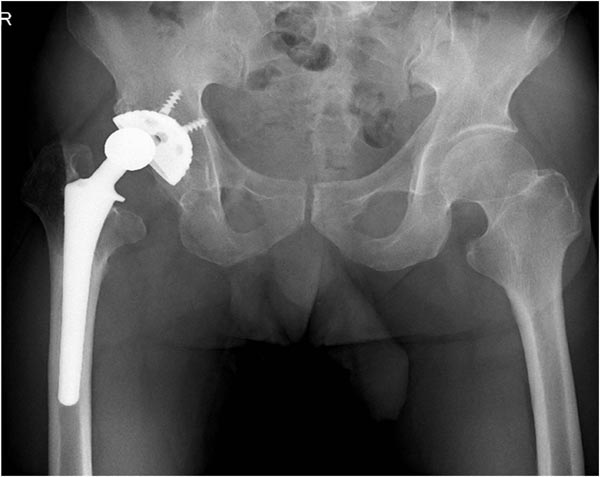
Case 2 pertains to a 72-year-old man. He underwent right THA from a posterolateral approach due to a diagnosis of coxarthrosis. An AMS-HA acetabular shell (outer diameter 50 mm, inner diameter 44 mm) with an XLPE liner was set in the acetabulum with two screws, and a cementless proximal-hydroxyappatite-coated femoral component (a PerFix-HA #12-M stem) was used along with a 26 mm zirconia ball (Kyocera Medical, Osaka, Japan). The inclination angle of the socket was 50 degrees, the anteversion angle was 1 degree, the vertical distance from the tear drop to the center of the femoral head was 27 mm, and the horizontal distance was 33 mm. Although no problems were observed till 9 years following surgery (Fig. 3a), inguinal pain in the right hip occurred at 9 years and 10 months following surgery. Although a plain X-ray revealed that the right femoral head had deviated to the outer upper side of the acetabular socket, osteolysis was not observed in the vicinity of the acetabulum and femoral implant (Fig. 3b). Upon surgery, the XLPE liner was found to have dissociated to the inner lower part from the acetabular socket in the same manner as case 1. No loosening of the acetabular socket was observed, but damage was observed in 1 among the 4 clicks, which is the liner gripping mechanism of the acetabular socket. Fixation of the femoral component was good with no macroscopic observation of the trunnion, so revision surgery of the acetabulum side was carried out and the ball was exchanged. The extracted XLPE liner was observed with partial damage in the elevated rim of the alternative side and end section surface along with scratches on the back side (Fig. 3c and 3d, Table 1).

DISCUSSION
In this study, we experienced two cases of PE liner dissociation from an acetabular cementless metal socket, which is relatively rare. The inclination degree of the acetabular socket was within 50°, approximately 10 years had passed since surgery, and a 26 mm femoral head and XLPE liner were used in both cases. As of 2016, XLPE liner dissociation has been observed in only 2 of the 4153 cases (0.04%) at our institute, and according to a manufacturer’s survey, it has occurred in 11 of 63057 cases (0.02%).
Hara et al. reported two cases of damage to the elevated rim of the XLPE liner using the present model. No damage to the conventional PE liner has been reported, and it is believed that damage to the rim of the liner was caused by oxidation due to using the annealed highly cross-linked method, leading to dissociation of the XLPE liner following this damage [19]. It is difficult to verify whether or not the dissociation was caused by this damage or whether the damage was caused following dissociation; however, the elevated rim of the XLPE liner remained in Case 1, suggesting that dissociation occurred first at least in Case 1, and we concluded that dissociation of the XLPE liner occurred due to sinking of the posterior side inside the shell and rotating of the anterior side downwards, thereby causing friction between the liner and stem neck at the bottom part after dissociation.
There have been several reports on PE liner dissociation from cementless acetabular shells regarding Harris-Galante cementless prostheses. Harris-Galante cementless prostheses are considered problematic in that the PE liner is fixed by gripping the cementless acetabular shell with tines using a push in type liner fixing format [1 - 6]. Gonzalez Della Valle et al. mentioned that dissociation of the PE liner of Harris-Galante cementless prosthesis occurs via the following three mechanisms: (1) damage due to fatigued tines in titanium sockets;(2) increased micro motion in the socket liner interface; and (3) impingement of the stem neck and liner border [3]. The fixing formats of PE liners to cementless acetabular shells include push in, ring lock, locking groove, etc.; however, the liner fixing format of push in and ring lock have come to be considered problematic due to their weak fixing force, and so the locking groove fixing format is recommended [20]. The configuration involving gripping the groove of the PE or XLPE liner with four clicks of the AMS-HA acetabular shell is also a push in type liner fixing format similar to Harris-Galante cementless prostheses, and it is believed that there was a problem with this fixing mechanism. Upon finite element method analysis of the present model, it was found that force concentrated in the clicking part, leading to a loss in the locking machinery when the groove of PE liner is damaged and ultimately causing dissociation. The size of the force is affected by the thickness of the PE liner, with the force increasing as the PE thins. In the present model, no dissociation of the PE liner has been observed in cases using a 22 mm femoral head; however, many cases of dissociation have been observed with sandwich type ABS liners, and it is surmised that the liner thickness is involved in the occurrence of dissociation. Scratch marks from the gripping click have been observed on the back side upon analysis of extracted PE liners, and it is surmised that force concentrated on the clicking part of the liner gripping, causing the locking machine of the clicking part to gradually break, leading to dissociation. Moreover, increased load due to increased alternative torque accompanying enlargement of the femoral head and the structural problem of the rotatable fixation contributing to one area are also believed to cause micro motion and back side wear, which may have enhanced polyethylene liner dissociation.
In other models, Gray et al. reported that offset, face-change polyethylene liners dissociate due to enlargement of the inclination angle of the acetabular socket [7]. The inclination angle of the acetabular socket was within 50° in the present cases, and it is believed there were no problems with setting of the socket.
AMS-HA acetabular shells have a problem with the liner fixing format, which may cause dissociation due to an enlarged femoral head, rim impingement, and declined strength at XLPE. Moreover, in recent years, a tendency has been observed for the femoral head to enlarge, with the same problem potentially occurring in other models, and it is believed that a strong locking groove fixing format is required.
CONCLUSION
Attention is required regarding AMS-HA acetabular shells as they are problematically of a push in type liner fixing format having a danger of PE liner dissociation.
LIST OF ABBREVIATIONS
| ABS | = Alumina-bearing-surface |
| PE | = Polyethylene |
| THA | = Total hip arthroplasty |
| XLPE | = Cross-linked polyethylene |
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

