All published articles of this journal are available on ScienceDirect.

Test-Retest Reliability and Convergent Validity of a Computer Based Hand Function Test Protocol in People with Arthritis
Abstract
Objectives: A computer based hand function assessment tool has been developed to provide a standardized method for quantifying task performance during manipulations of common objects/tools/utensils with diverse physical properties and grip/grasp requirements for handling. The study objectives were to determine test-retest reliability and convergent validity of the test protocol in people with arthritis.
Methods: Three different object manipulation tasks were evaluated twice in forty people with rheumatoid arthritis (RA) or hand osteoarthritis (HOA). Each object was instrumented with a motion sensor and moved in concert with a computer generated visual target. Self-reported joint pain and stiffness levels were recorded before and after each task. Task performance was determined by comparing the object movement with the computer target motion. This was correlated with grip strength, nine hole peg test, Disabilities of Arm, Shoulder, and Hand (DASH) questionnaire, and the Health Assessment Questionnaire (HAQ) scores.
Results: The test protocol indicated moderate to high test-retest reliability of performance measures for three manipulation tasks, intraclass correlation coefficients (ICCs) ranging between 0.5 to 0.84, p<0.05. Strength of association between task performance measures with self- reported activity/participation composite scores was low to moderate (Spearman rho <0.7). Low correlations (Spearman rho < 0.4) were observed between task performance measures and grip strength; and between three objects’ performance measures. Significant reduction in pain and joint stiffness (p<0.05) was observed after performing each task.
Conclusion: The study presents initial evidence on the test retest reliability and convergent validity of a computer based hand function assessment protocol in people with rheumatoid arthritis or hand osteoarthritis. The novel tool objectively measures overall task performance during a variety of object manipulation tasks done by tracking a computer based visual target. This allows an innovative method of assessing performance than considering the time taken to complete a task or relying on subjective measures of self-reports on a limited range of objects and tasks covered. In addition, joint pain and stiffness levels before and after a manipulation task are tracked, which is lacking in other hand outcome measures. Performance measures during a broad range of object manipulation tasks relate to many activities relevant to life role participation. Therefore, task performance evaluation of common objects, utensils, or tools would be more valuable to gauge the difficulties encountered in daily life by people with arthritis. Future studies should consider a few revisions of the present protocol and evaluate a number of different objects targeting strength, fine, and gross dexterity based tasks for a broader application of the tool in arthritis populations.
INTRODUCTION
Hand exercise programs that include range of motion (ROM), and strengthening exercises are important compo-nents of non-pharmacological management in people with rheumatoid arthritis (RA) or hand osteoarthritis (HOA) [1-4]. With moderate literature evidence available on the thera-peutic effectiveness of ROM and strength exercises in improving hand function [1-4], a novel task-oriented training using real life object manipulation tasks has been developedfor people with arthritis affecting the hands [5-7]. An innovative computer game-based Tele-rehabilitation platform (TRP) has also been developed in which task-oriented training is coupled with interactive computer gaming [5-7] to increase client motivation and engagement. Using the task- oriented approach, a variety of manipulation tasks with objects of daily life can be practiced while playing computer games [5, 7]. Since home exercise programs are important part of the rehabilitation process, the TRP was designed to extend clinical practice to the home, supported by a clinician. The TRP also includes a telemonitoring application, which is a computer based hand function assessment tool that evaluates task performance during any object manipulation. The telemonitoring module automatically logs clients' task performance measures, and data analyses methods have been developed to quantify task performance during functional object manipulation tasks. These objective outcomes can then be used to track and monitor hand function over repeated sessions [5, 7].
Difficulties in many gross/fine dexterous activities such as opening jar lids, turning door knobs or keys, gripping small objects between finger tips, and holding heavy objects are well documented in RA [8, 9] and HOA [10, 11]. A number of performance based tests are available, such as the Purdue peg board test, nine hole peg test (NHPT) [12, 13], O’Connor Finger Dexterity test [16] Grip Ability Test (GAT) [12], Arthritis Hand Function Test (AHFT) [12-15] and the Jebsen hand function test (JHFT) [12, 13]. These tests measure hand function by the time taken to complete a task. This approach has limited value [12] because, 1) time does not directly relate to performance [20], 2) it is unclear how speed translates into hand use in daily life [17] and 3) speed should not be prioritized over quality [18]. More recently, computer-based hand function assessment tools are being developed which quantify fine/gross motor manipulat-ion skills. For example, Culmera et al [19] developed a standardized hand tracing task that measures both movement duration and spatial-temporal accuracy of fine/gross manipulat-ion skills. However, the above-mentioned tests are limited to a narrow range of objects and tasks, for example: pegs coins, a pen, or kitchen utensils. The pain or stiffness associated with a task was also not considered in any of the test measures. A novel computer based hand function tool has been designed to, 1) provide a standardized method to objectively quantify task performance (movement quality) during manipulation of a broad range of common objects, and 2) evaluate pain and joint stiffness related with each object manipulation task. Reliability and validity of the tool’s test protocol has been demonstrated in asymptomatic individuals [20].
The objectives of the present study were to determine test-retest reliability and convergent validity of the computer based hand function test protocol in people with arthritis. Task performance during three different object manipulation tasks were evaluated. We hypothesized that the performance measures of object manipulation tasks would exhibit high test-retest reliability (ICCs >0.75), and demonstrate moderate correlations (Spearman rho between 0.4 and 0.7) with grip strength, NHPT, DASH and the HAQ. Our secondary object-ives were to evaluate joint pain and stiffness outcomes with three different object manipulation tasks.
SAMPLE SIZE JUSTIFICATION
With no dropouts assumed, 39 participants were included for ICCs >0.6 with a power of 0.80 and a significance level of 0.05 [21]. A sample size of 30 is considered enough for estimates of reliability and validity, though larger numbers are often preferred [22].
METHODS
A repeated measures design was used to establish test-retest reliability of the test protocol. Forty participants were recruited through advertisements in local newspapers and rheumatology clinics in Winnipeg. Men and women between 30 and 65 years and diagnosed with RA or HOA were included. People with fixed finger joint deformities, recent upper limb surgeries or trauma (< 6 months), or vision/ hearing problems were excluded. The study was approved by the University of Manitoba Health Research Ethics Board (H2008: 216). Written informed consent was obtained from each participant before evaluation.
Materials
A computerized custom visual tracking task with configurable amplitude and frequency designed with a visual target (a bright colored circular cursor) moving sinusoidally in x or y-axis served as a standardized input to guide a manipulation task. The physical components of the tool include a miniature motion sensor (5mm x10mm Minibird model 800, Ascension Technology, Burlington VT, USA) and a hardware interface. Many different objects of daily life can be instrumented with the motion sensor and hence different types of functional tasks can be examined (Table 1). The sensor records the linear and angular position coordinates in the x, y, and z-axes at a sampling rate of 100Hz. The interface allows seamless translation of motion signals from any instrumented object and makes it behave as a standard mouse. The object motions are then used to perform the tracking task (for example: a wineglass tilted up down, as shown in Fig. 1A insert). The moving visual target is set at a frequency of 0.5 Hz and an onscreen amplitude of 15 cm representing optimal motion parameters experienced in daily activities. The position coordinates of the visual target and the motion sensor (user motion) were saved as an electronic file [20]. The tool was also embedded with two separate 0-10 numerical verbal scales for self-reporting of pain and stiffness (Fig. 1B, 1C). These scales appeared in sequence on the computer screen and participants were asked to self-report their pain and stiffness before and after performing the tracking task [20]. The study staff recorded the scores, which were automatically saved with the user motion data [5, 7, 20].
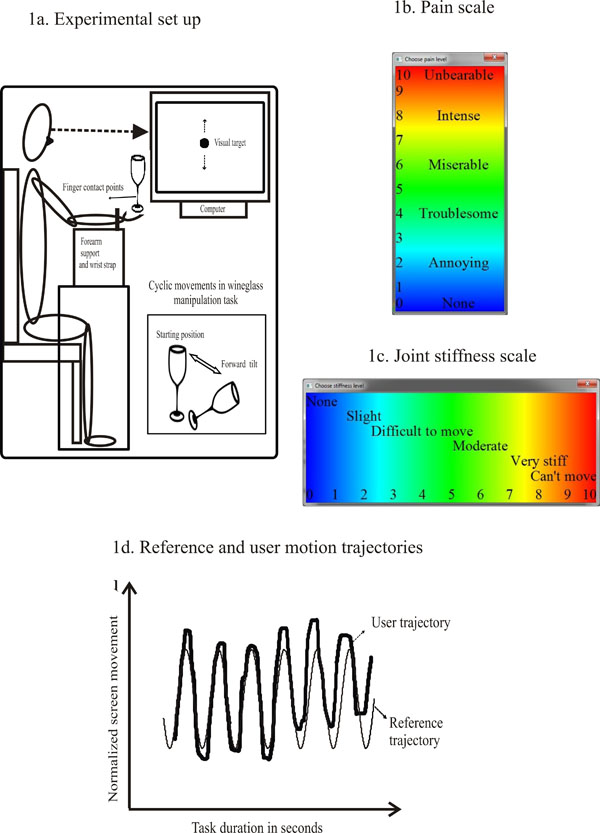
A. Experimental setup. Participants were comfortably seated before a computer monitor. A plastic wineglass is held with a tripod grip and moved in concert with a sinusoidally moving visual target. The bottom insert shows forward and backward tilting movements of the wine glass on tracking the target moving upward and downward respectively. B. Pain scale. The verbal numerical pain rating scale (0-10) is shown. Blue, green, yellow and red colors depict increasing intensities of pain. C. Stiffness scale. The verbal numerical stiffness rating scale (0-10) is shown. Blue, green, yellow, and red colors depict increasing intensities of stiffness. D. Reference and user movement trajectories. The bold lined waveform represents the user trajectory and the light shaded waveform is the reference trajectory. Y-axis represents screen amplitude and the x-axis represents time in seconds.

a. User movement trajectory plots for all three tasks. The user trajectory plots for wineglass, salad tongs, and jug tasks are shown. The top panel of plots represent user trajectories with COD’s >0.80 and bottom panel with COD’s <0.5. The maximum and minimum boundaries of reference waveform are highlighted by horizontal lines above and below each user trajectory. b. Mean and standard error of mean for COD of each task. Histograms of mean and standard error of mean for COD of wineglass (WG), salad tongs (ST) and jug (JG) tasks in test sessions 1 (grey bars) and 2 (black bars). COD measured from 0-1, is represented on the y-axis.
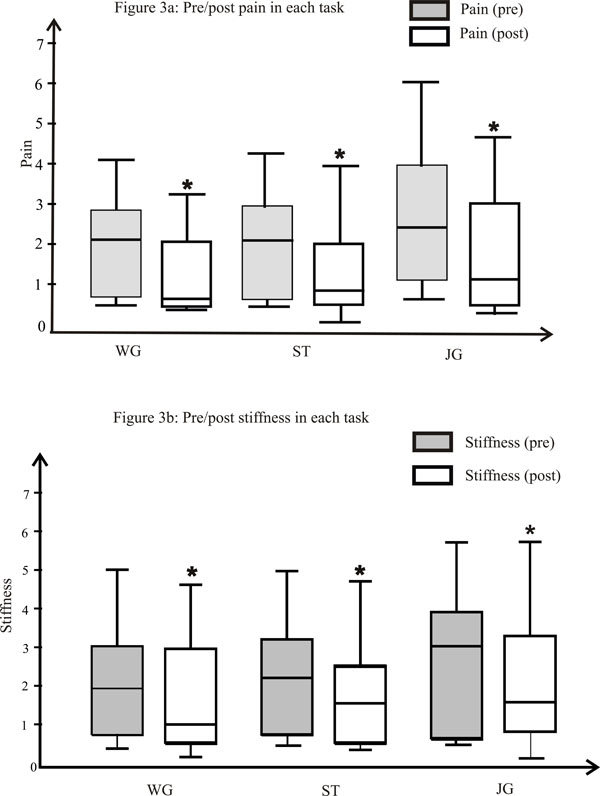
A. Pre/post pain in each task. The box and whisker plot shows pain scores for each task. The Y-axis represents the pain scores on (0-10) scale. The upper and lower parts of the boxes represent the upper and lower quartiles and the median is presented as the middle line. The upper and lower whiskers are the maximum and minimum values, * significance p<0.05. B. Pre/post stiffness in each task. The box and whisker plot shows stiffness scores for each task. The Y-axis represents the stiffness scores on (0-10) scale. The upper and lower parts of the boxes represent the upper and lower quartiles and the median is presented as the middle line. The upper and lower whiskers are the maximum and minimum values, *significance p<0.05.
Examples of functional tasks that could be examined with computer based tracking
|
Demographic characteristics of the study participants and clinical, self-report hand function measures Mean (SD).
| Total participants/RA/OA | 40/14/26 |
| Men/Women | 6/34 |
| Age range (years) | 34-63 |
| Age | 54±6.7 |
| Grip strength (kgs) | 19.9±8.2 |
| NHPT (seconds) | 28.2±7.8 |
| DASH (/100) | 36.3±16.1 |
| HAQ-DI (/3) | 1.1±0.8 |
NHPT=Nine Hole Peg Test; DASH=Disabilities of Shoulder, Arm and Hand; HAQ-DI =Health Assessment Questionnaire- Disability Index.
Means (SDs) of the test and retest COD scores, ICC (95% CI) and SEM for each manipulation task.
| Object | COD Scores | ICC (95% CI) | SEM | |
|---|---|---|---|---|
| Test 1 | Retest | |||
| Wineglass | 0.64±0.2 | 0.66±0.2 | 0.84*(0.67-0.93) | 0.08 |
| Salad tongs | 0.4±0.24 | 0.4±0.3 | 0.5*(0.07-0.77) | 0.19 |
| Jug | 0.54±0.23 | 0.6±0.2 | 0.53* (0.1-0.83) | 0.15 |
*Significant p<0.05.
Spearman correlation co-efficient ‘rho’ between task performances of object manipulations with other clinical and self-report measures of hand function.
| Variables | WG-COD | ST-COD | JG-COD | Grip | NHPT | DASH | HAQ-DI |
|---|---|---|---|---|---|---|---|
| WG-COD | - | 0.17 | 0.33* | -0.22 | -0.15 | -0.3* | -0.5* |
| ST-COD | - | - | 0.3 | -0.1 | -0.14 | -0.23 | -0.12 |
| JG-COD | - | - | - | -0.1 | -0.2 | -0.2 | -0.4 |
| Grip | - | - | - | - | -0.3* | -0.41* | 0.5* |
| NHPT | - | - | - | - | - | -0.3* | -0.25 |
| DASH | - | - | - | - | - | - | 0.61* |
*Significant p<0.05.
WG-COD=Wineglass-Co-efficient of Determination; ST-COD=Salad tongs-Co-efficient of Determination; JG –COD=Jug-Co-efficient of Determination; NHPT=Nine Hole Peg Test; DASH=Disabilities of Shoulder, Arm and Hand; HAQ = Health Assessment Questionnaire- Disability Index.
Protocol
The first test session included administration of grip strength test; NHPT and DASH in the same order, before evaluating the three object tasks. Grip strength of the dominant hand was tested using an isometric hand dynamometer (G100, Biometrics Ltd., UK) in the testing position recommended by American Society of Hand Therapists [23, 24]. Participants gripped the dynamometer as hard as possible once without any jerking. The best score out of three consecutive trials was used for analyses. Sufficient time was allowed for the participants to recover from any fatigue related to grip testing. Fine finger dexterity was then assessed by the time taken for placement and removal of nine pegs in the pegboard using the NHPT [25]. Participants also completed the DASH [26, 27], which contains 30 items on disability/symptoms related to upper limb activities. Level of difficulty in performing each item is rated on a 1-5 point scale (1- no difficulty and 5- unable to do). Scores range between 0-100 with higher scores indicating greater disability.
Fig. (1) illustrates the experimental setup, and the pain and stiffness scales. The participant was comfortably seated before a computer monitor positioned at eye level. The arm was positioned with the shoulder flexed at 60 degrees and internally rotated, elbow flexed and forearm supported on a 15-inch Styrofoam block. A strap around the wrist allowed free hand movements in the air. The objects included a long stem plastic wineglass, salad tongs and a jug half filled with water. These objects represent a wide range of physical properties requiring different modes of manipulation such as tripod grip, thumb opposition, and whole hand grasp respectively. In both test sessions, the motion sensor was secured on a same point marked on the mid portion of the wineglass bowl; the top arm of the salad tongs and on the mid portion of the jug’s front surface (opposite to handle). Manipulation of the wineglass required a tripod grip involving the thumb, index, and middle fingers. The wineglass held at the stem was tilted forward down (away from the body) and straight up to vertical (towards the body), bottom insert of Fig. (1A). The task involved thumb opposition and interphalangeal (IP) flexion, index finger abduction, metacarpophalangeal (MCP) flexion, rotation and IP flexion or extension of index and middle fingers, and ulnar/radial deviations. The other two fingers could flex or extend. Manipulation of the salad tongs involved full open-ing and closing of the two arms together with the vertical movements of the visual target. They were held with the thumb placed on the top arm while the index and middle fingers held the lower arm. The task involved thumb extension, adduction/abduction MCP and IP flexion/extens-ion at the second and third digits. The jug was held with a power grasp and tilted left and right along the horizontally moving target. With the forearm in the mid prone position, the task included supination/pronation, and flexion at the MCP, IP joints of all fingers and the thumb in extension. The motion was restricted to the wrist and forearm while the fingers provided a stable grip. Three to five minutes of transition time was allowed before the next consecutive task. All of the participants were provided with a demonstration before testing. After one practice trial, each task was evaluated for 20 seconds, which produced 12 movement cycles.
A week later, the HAQ questionnaire [28, 29] which measures difficulties in daily activities using a 0-3 point scale (0- without difficulty, 3- unable to do), was completed. The same assessor then evaluated the three tasks in the same order.
Data Analyses
The user motion data from each task was processed using custom Matlab scripts (The Math Works, Natick, MA) [5, 7, and 20]. A non- linear least squares algorithm was used to obtain a sine-wave function of the target cursor waveform. Based on the known reference trajectory and the participant’s actual motion, the co- efficient of determination (COD) was calculated to represent task performance, i.e. how well each participant followed the cyclic cursor motion. CODs range between 0 and 1 with values closer to 1 [20] representing more closeness. Based on the COD values, task performance could be arbitrarily classified as good (COD>0.8), fair (COD between 0.5-0. 8), and poor (COD <0.5). Fig. (1D) shows the reference and user motion trajectories for one of the tasks.
Statistical Analyses
Test-retest reliability of the test protocol was evaluated using:
- Intraclass correlation co- efficient [ICC (2, 1)] to determine the relative retest reliability. ICC values were interpreted [30] as very high (ICC>0.9), high (ICC > 0.75), moderate (ICC between 0.5- 0.75) and low (ICC > 0.5).
- Standard error of measurement (SEM) to determine the absolute reliability, using the formula SEM = SD , where SD is the average standard deviation of the two session scores [31].
- Paired student ‘t’ test for mean differences between the two session scores.
- Convergent validity was analyzed using Spearman rank correlation co-efficient (rho) to determine the strength of the relationship between task performance measures and grip strength, NHPT, DASH and HAQ. The strength of correlation was interpreted as high (rho > 0.7), moderate (0.4 to 0.7) and low (<0.4) [32].
- The Wilcoxon signed rank test to evaluate the differences in joint pain and stiffness before and after each manipulation task.
- Data was analyzed with IBM SPSS Statistics for Windows, Version 19.0. Armonk, NY: IBM Corp. Statistical significance was p<0.05 (Two tailed).
RESULTS
Demographic characteristics and the scores (Mean ±SD) of grip strength, NHPT, DASH and HAQ of the study participants are presented in Table 2. Fig. (2a) presents representative examples (and respective CODs) of the user motion trajectories with the three tasks. The top panels of plots are examples of good performance (CODs > 0.8) and the bottom panels, of poor performance (CODs <0.5). Fig. (2b) presents the mean (standard error) for the COD of each task during both test sessions. Table 3 presents the group means (SD) for COD, ICCs, and SEMs. Test re-test reliability of the task performance was high (ICC >0.75) for wineglass task and moderate (ICC between 0.5 and 0.75) for the jug and salad tongs tasks. Paired student’t’ tests showed no significant differences in mean performance measures for each task between the sessions (p>0.05).
Table 4 presents the ‘rho’ values reported between 1) task performance measures of wineglass, salad tongs, and jug manipulations with grip strength, NHPT, DASH, and HAQ, 2) task performance measures of wineglass, salad tongs, and jug manipulations, and 3) grip strength, NHPT, DASH, and HAQ. The HAQ was moderately correlated with the task performance measures of wineglass and jug tasks but had low correlations with salad tongs task. Low correlations were observed between all task performance measures and grip strength, NHPT and the DASH, and between the task performance measures of three objects themselves. Moderate correlations were seen between the DASH and HAQ; and between grip strength, DASH, and HAQ respectively.
Fig. (3A, 3B) presents the box and whisker plots for group median and Interquartile range (IQR) for pain and stiffness scores reported before and after each task. There was significant reduction in pain and stiffness levels after each task in both test sessions (p<0.05).
DISCUSSION
The study purpose was to determine Test-retest reliability and convergent validity of a computer based hand function test protocol in people with arthritis. Test-retest reliability of performance measures during manipulation of three common objects (wineglass, salad tongs, and jug) ranged from high to moderate. In general, we observed low correlations between the task performance measures and grip strength, NHPT, DASH and HAQ. Exceptions were moderate correlations between the wineglass and jug task performance measures with the HAQ. In addition, performance measures between the objects demonstrated low correlations with each other. Interestingly, there was a significant reduction in joint pain and stiffness after performing each task.
Test-Retest Reliability
The test protocol indicated moderate to high test-retest reliability of performance measures for three manipulation tasks using objects with a broad range of properties and functional requirements. These findings are comparable to other hand function measures such as the Arthritis Hand Function Test (ICCs range 0.53-0.96) [33]. It was interesting to note that the task with the best performance (wine glass) also had the highest ICC; the task with the poorest perf-ormance (salad tongs) had the lowest ICC. There is evidence that difficult tasks demonstrate low test-retest reliability likely due to poor reproduction of task performance [14, 34]. For example, in people with hand disabilities [14] the simu-lated feeding subtest of the Jebsen hand function test was found to be less reproducible (Pearson r=0.60) than the other subtests such as picking up small objects and card turning(r >0.80). Similarly, the pegboard dexterity of AHFT demon-strated an ICC of 0.53 compared to the other test items (ICC between 0.69 - 0.95) [33]. The SEMs were 12%, 47.5%, and 26% for the task performance measures of the wineglass, salad tongs and jug tasks respectively.
Convergent Validity
The low correlations between grip strength and the task performance measures were not surprising. Isometric grip strength is an objective measure of maximal voluntary effort of wrist and hand muscles, which is required for handling and moving heavy items. Manipulation of the salad tongs and the wineglass involved only the thumb, index, and middle fingers where grip force is not important; similarly, the jug task also required precise and cyclic tilting movements, in addition to a modest magnitude of grasp. Tsang et al, 2004 [34] found fair to moderate (Pearson coefficients ‘r’ ranging from -0.38 to -0.53) correlations between grip strength and functional tasks of Jebsen Hand Function Test (JHFT), which do not require isometric hand strength for their execution such as writing (r=-0.45), card turning (r=-0.38), picking up small common objects(r=-0.48), simulated feeding (r=-0.48), stacking checkers(r=-0.53), picking up large light cans (r=-0.42), and picking up large heavy cans (r=-0.43) evaluated in people with rheumatoid arthritis.
Low correlations were also observed between NHPT and the task performance measures. The NHPT uses very small pegs requiring fine control of the thumb and index finger and minimal joint motions. Performance is graded by time in seconds. Neither movement quality nor efficiency is quantified, whereas COD measures quality of movement during different tasks irrespective of object used. This likely explains the low correlations between the NHPT and task performance measures. Similarly, low correlations between the task performance measures themselves may be explained as these three objects are completely different from each other in terms of physical properties, grip/grasp, and functional requirements for handling. In the present study, the DASH and HAQ showed low correlations with the task performance measures and the NHPT. The DASH and HAQ are questionnaires covering an individual’s health and functioning predominantly in terms of activity and participation. The DASH contains 21 items related to daily activities, social participation (4 items), and body functions (5 items). Only six items pertain to finger/hand use while the other items require either whole upper limb or bilateral upper limb action. Similarly, out of the twenty items in the HAQ, only seven are specifically related to finger/hand use while the other items require either whole body or lower extremity mobility for execution, e.g. walking. Both questionnaires have a limited proportion of items focused on finger/hand tasks, 25% in the DASH, and 35% in the HAQ. The HAQ also has items of high content density ratio [35] which are difficult to answer, examples: “are you able to dress yourself, including tying shoelaces and doing buttons” and “are you able to do chores such as vacuuming or yard work” [28, 29]. In addition, factors such as compensatory movements and different adaptive strategies that are often learned to accomplish a task [37] may influence perceived level of difficulty. Taken together, these would explain why performance based COD measures had low correlations with self- reported composite scores of activity/participation. Consistent with previous studies [36-38], the present study showed modest correlations between grip strength and the DASH and HAQ. Both questionnaires measure level of difficulty experienced during activities and share similar items such as personal hygiene, opening jars, household work, and transportation activities. Since the majority of daily tasks are dexterity- based and less than 14% requires maximal grip strength [39] for execution, this is not surprising.
Pain and Stiffness Outcomes
One may have thought that repeated cyclic manipulation tasks would have aggravated pain. Unexpectedly, pain and stiffness decreased after performing the cyclic tasks for all three objects during both test sessions. These findings are consistent with evidence on the role of exercises in the management of arthritis pain and stiffness affecting larger joints such as hip, knee, and shoulder [40-42] in individuals with OA and RA.
Strengths and Limitations
The tracking task provides a standardized method to collect and analyze movement from a diverse range of objects, utensils, or tools used in daily activities. A functional framework to select “assessment” objects relevant for individual clients has been developed and the present protocol allows quantification of the ability to manipulate a broad range of objects. The disease severity and magnitude of finger joint deformities were not determined in the present study. In addition, each of the tasks was tested only once in each session. These factors might have influenced the performance outcomes. Although the tracking task is easy and simple to follow, it does require some cognitive abilities, which was not specifically addressed before application.
Disease factors such as structural joint deformities, muscle weakness, daily variations in arthritis joint pain [43-47] and stiffness, and/or timing of pain medications [43] are some of the additional factors to be considered in measurement variations. Daily variations in pain have been well documented in both arthritis populations. For example, in one study [44] involving 40 patients with hand osteoarthritis, considerable variations was noted in daily pain levels, ranging between minimum mean (sd) of 17.9 (19.1) to maximum 54.4 (27.9) on 1-100 visual analogue scale. There was also considerable inter-subject differences noted in the daily pain patterns which generally represented the osteoarthritis clinical picture with pain levels declining in morning and evening, and increasing during afternoon. Another study [45] that recorded pain over 24 hours in 21 patients with hand osteoarthritis reported an average variation of 42 points on 0-100 scale. Similarly, pain and stiffness levels were reported less during evenings in patients with rheumatoid arthritis [46-49]. In relation to such variations in everyday pain levels, the manipulation tasks performance or the responses to the questionnaires might have been influenced during the day of assessment. However, no clinical evidence was mapped between timings of assessment, pain medication, and tasks performance in the present study.
A standardized test protocol would reduce random errors of measurement and lead to high reliability [43]. Before performing each object manipulation task, all participants followed a standard protocol (standardized starting position, task duration, amplitude and speed settings, and movement) to execute each task. In spite of the efforts taken to reduce random errors, the study data reported with ICCs <0.9. One of the reasons was that a narrow range of mean CoD was generated for each task during each test session, meaning the study sample was homogenous with less between-subject variability in the measurement and hence leading to low reliability estimates [43]. In order to obtain a wide range of between-subject variable measures and high reliability estimates, a heterogeneous sample should be considered in future validation studies. Learning effects are unlikely to occur across first and second test sessions as the one-week gap between is considered appropriate to alleviate any recall bias.
FUTURE DIRECTIONS
Concerning the grip strength been considered for construct validity, it is often an important outcome of hand rehabilitation programs and has been evaluated as a proxy measure for hand function in many studies involving rheumatoid and osteoarthritis populations [50-58]. The DASH questionnaire was considered for: 1) the questionnaire items focus on impairments, activity limitations, and participation restrictions, which are the three constructs of the Internatio-nal Classification of Functioning Disability and Health (ICF) taxonomy model, 2) compared to other upper limb self-report questionnaires, the DASH has excellent psychometric proprieties in a wide variety of upper limb conditions [26, 59-61], 3) it is also being extensively used in clinical practice and research in rheumatoid and osteoarthritis popu-lations [61], and, 4) administration and respondent burden to complete the questionnaire is minimal. The approximate time for administration and scoring were 10-15, and five minutes respectively. However, as the DASH questionnaire represent limited number of hand function related tasks in daily life, it would of benefit and meaningful to include other self-report measures such as Patient Rated Wrist Hand Evaluation (PRWHE) [26, 27, 61], and Michigan Hand Out-comes Questionnaire (MHQ) [15] in future studies. Both cover specific domains of hand function such as difficulties in performing activities of daily life, pain, aesthetics, and satisfaction and hence might be considered for validity evaluation of the computer game based hand function tool.
The potential contribution of the novel measure is that it provides an objective measurement of overall performance of any object manipulation task. While other objective hand function measures the time taken to complete a task as a surrogate for hand function, the novel tool analyses the entire movement trajectory of a manipulation task to provide direct outcome of the performance. Evaluation of the tool measure in three different objects has provided valuable evidence on the feasibility of the protocol and initial data on the COD, pain, and stiffness scores. The tool should be tested further in other manipulation tasks that have been documented difficult to perform in people with arthritis hands, for example, opening a jar lid, pouring activity, and carrying heavy weights etc. Future modifications in the final protocol would include a heterogeneous study sample, tracking of pain medication data, and repeated testing of the tool measure in many number of manipulation tasks and validating with other comparative hand function measures in hand osteoarthritis and rheumatoid arthritis populations.
CONCLUSION
According to the International Classification of Functioning, Disability, and Health (ICF) framework, the impact of a health condition on an individual can be classified through Body Structure/Function and Activities and Participation, which are further influenced by environmental/personal factors [62]. Measurement of function and life-role participation interact [63] and many agree that we should measure at each level in order to determine which interventions that result in gains in task skills and function also result in sufficient improvements in life role participation [63, 64]. For example how and to what extent does increased strength, or movement quality of fine/gross object manipulation tasks improve an individual’s ability to manage housework, go shopping, use an ATM card or participate in various leisure and social activities. There is also a definite need to develop tools to identify and delineate outcomes and parameters of rehabilitation programs [65], which could be used to track changes over time and make informed decisions about efficacy and dose response relationships [66, 67]. The computer based assessment tool allows a within subject analysis and trends could be identified with even larger variations in performance measures. In addition, hand function cannot be graded with just one task; therefore testing of many several common objects should be included. A pilot randomized trial [7], in which the present tool is used as an exploratory outcome measure has been completed.
The computer based hand assessment tool provides a standardized method to evaluate task performance during any object manipulation task. This approach allows one to focus not only on body functions and on structures but also on outcomes related to activity and participation; and movement precision that is a critical factor for efficient performance. Many different objects of daily life can be used and thus performance with different types of manipulation tasks can be objectively quantified with the tool. Knowledge of the object properties and functional demands allows therapists to target specific treatment goals such as graded joint mobility, endurance, strength, and dexterity. In this way, the tool can also be used for task-oriented training with real life objects and personalized training goals in order to improve hand function in daily life.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
This study was financially supported by operating grants from the Canadian Arthritis Network (CAN) and Manitoba Centre of Excellence Fund (MCEF).

