All published articles of this journal are available on ScienceDirect.

Radiocarpal and Midcarpal Instability in Rheumatoid Patients: A Systematic Review
Authors Info & Affiliations
Abstract
Background:
This study was aimed at identifying the criteria for the diagnosis of Radiocarpal instability in rheumatoid arthritis RA).
Methods:
The main databases were searched to identify studies describing the pathophysiology of Radiocarpal instability in patients with RA. We focussed on the epidemiology, radiographic parameters, criteria for instability and on treatment options. Results. In the search 108 articles were found, of these 12 studies were included for this review. Instability occurs in at an average of 35.2% of the rheumatoid wrists. The instability was found between 8 and 13 years after onset of rheumatoid arthritis. A strong correlation was found between instability, duration of RA and Larsen score. Several radiographic methods were described to evaluate Radiocarpal instability in RA. Several treatment options for instability in patients with RA are described. All with their own indications and limitations.
Conclusion:
OOn a standard AP radiograph deformity can be measured using the carpal height and the ulnar translation index of Chamay. This gives an indication for instability. For describing the deterioration of the joints the Larsen score is most used. If there are more radiographs in time the Simmen classification can be used. For real assessment of instability dynamic radiographs are needed.
Level of Evidence:
Level IV.
INTRODUCTION
The wrist is frequently involved in rheumatoid arthritis (RA) and often the first site of expression of symptoms of the disease [1-3]. Within the wrist, synovial inflammation causes changes in articular cartilage and subchondral bone. There may also be involvement of the synovial lining of the ligaments and the tendons, particularly at the site of their attachment to the bone [4]. Synovitis at capsular insertions may stretch the intrinsic and extrinsic carpal ligaments, which may cause an abnormal transfer of loads (dyskinetics)and abnormal wrist motion (dyskinematics), such as among others the so-called Radiocarpal and Midcarpal instability [5]. The functional stability of the wrist is determined by the shape of the carpal bones, the integrity of the supporting ligamentous structures and the function of the muscles in controlling wrist motion during functional tasks. The ligaments of the wrist are either intrinsic or extrinsic. The former are located within the carpus and link carpal bones, whereas the latter originate outside the carpus and attach to the carpal bones at some part of the anatomic course [5].
The progression of wrist deformity is well described by Taleisnik (1985) [6] who postulated the sequential, predictable events in the RA wrist. The scapho-lunate ligament is prone to weakening from the synovitis, which leads to flexion of the scaphoid and collapse of the radial column. Stretching of the wrist ulnar collateral ligament attenuates the ulnar column support. These two events ultimately lead to the typical carpal supination pattern. It has been observed that the carpus may subluxate in an ulnar direction along the inclined radius. The consequence of carpal supination is the collapse of the radial wrist, which contributes to the radial deviation of the metacarpals and accentuates the ulnar deforming forces on the fingers at the MCP joints. The wrist joint may also subluxate in an anterior direction, which causes difficulties with wrist extension. Early detection en treatment of instability of the wrist might prevent further damage to the MCP joints and fingers.
Early diagnosis and treatment of wrist instability might prevent further deterioration of the wrist en subsequently it might prevent deviation of the metacarpals and destruction. Early intervention might prevent loss of function caused by instability and destruction.
It was the initial intention of the authors to use a strict methodology for paper selection, focussing on objectively measurable variables of instability, separate evaluation of different stages of rheumatoid arthritis (early, middle and late) and comparison of dynamic radiographs with conventional radiographs the different diagnostic modalities. These standards had to be abandoned however, as almost none of the available papers fulfilled the above mentioned criteria. So this study was aimed at identifying the criteria as reported in the literature for the diagnosis of Radiocarpal instability in rheumatoid arthritis. Which are the radiographic parameters to define instability and what are the normal values? What are the diagnostic tests and what is the value of each test? Other study questions: are there different types of carpal instability in RA. What is the epidemiology of carpal instability in RA patients? What are the functional impairments as caused by carpal instability, what are the treatment options and results of carpal instability in RA patients?
MATERIALS AND METHODS
The search of the literature performed in this study was limited to published original studies including male and/or female patients with uni- or bilateral rheumatoid arthritis of the wrist. Rheumatoid arthritis was defined with revised criteria for the classification of rheumatoid arthritis of the American Rheumatism Association [7]. All types of instability of the rheumatoid wrist in humans were included. Articles concerning instability of the distal radio ulnar joint were not included in this review, except when the patients with Radiocarpal and Midcarpal instability could be analysed separately. Only original published studies were included; review articles, expert opinions and abstracts from scientific meetings were excluded. The main databases Pubmed/ MEDLINE, Cochrane Clinical Trial Register, Current Controlled Trials and EMBASE were searched from 1968 to September 2013 to identify studies relating to the patho-physiology, prevention, diagnosis, treatment and prognosis of radio- and Midcarpal instability in patients with rheumatoid arthritis of the wrist (Fig. 1).
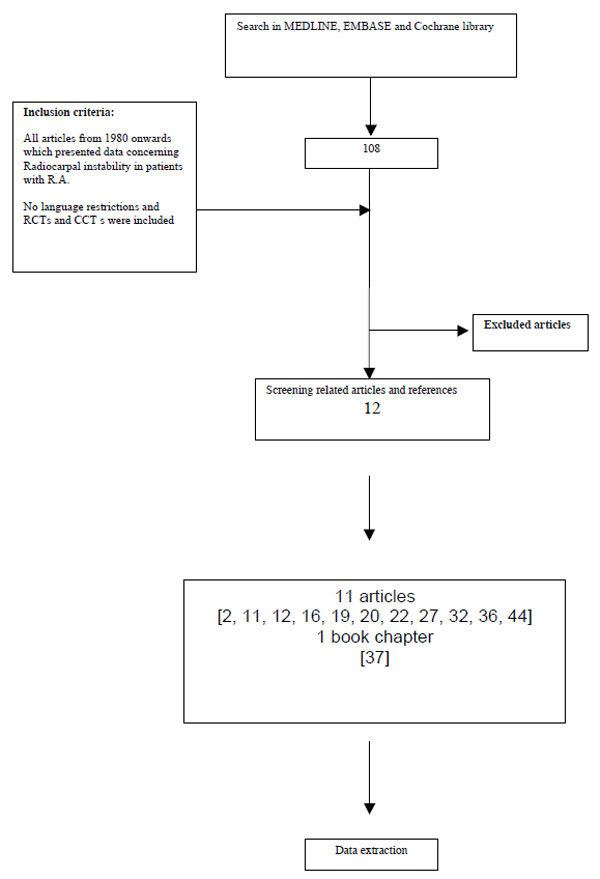
Flowchart summarizing the selection of relevant articles.
The applied search terms were: Radiocarpal instability, carpal ligaments, rheumatoid arthritis, wrist and pathophysiology. Furthermore, the lists of references of retrieved publications were manually checked for additional studies potentially meeting the inclusion criteria and not found by the electronic search. The search was restricted to articles written in the English, German, French and Dutch language. From the title, abstract, two reviewers (ER, MB) independently reviewed the literature searches to identify relevant articles for full review. From the full text, using the above mentioned criteria; two reviewers (ER, MB) independently selected articles for inclusion in this review. Any disagreements were resolved by consensus on the articles to be included.
RESULTS
The search strategy revealed 108 articles. After deduction of the overlaps between the different databases, evaluation of the abstracts and for some studies contact with the authors, a final total of 31 potentially eligible studies remained. The full texts of these articles were retrieved and thoroughly assessed as described above. This resulted in the inclusion of 11 studies 8-18, involving 576 patients with 687 unstable wrists (Table 1). From the initial 11 published references an additional book chapter was added [19]. The main reason for exclusion of the other 20 articles was that studies did not describe Radiocarpal nor Midcarpal instability in rheumatoid wrists but other types of instability and many articles did not describe original research. The publication dates span 20 years; in 1992, Simmen and Hagena’s [19] paper published was earliest and the paper from, Shimizu et al. [17] was the most recent publication. Five studies were performed in Europe, 2 in North America and 5 in Japan.
Pubmed/Medline search strategy.
| ("joint instability"[MeSH Terms] OR ("joint"[All Fields] AND |
| "instability"[All Fields]) OR "joint instability"[All Fields]) |
| AND |
| ("wrist"[MeSH Terms] OR "wrist"[All Fields] OR "wrist joint"[MeSH Terms] OR ("wrist"[All Fields] AND "joint"[All Fields]) OR "wrist |
| joint"[All Fields] OR "carpus"[All Fields]) |
| AND |
| ("arthritis, rheumatoid"[MeSH Terms] OR "rheumatoid arthritis"[tw]). |
Epidemiology
Instability occurs in at an average of 35.2% (Range 17-44%) of the rheumatoid wrists in the studies were prevalence was reported 8, 10, 11, 13-16, 18, 19.
The instability was found between 8 and 13 years after the onset of the rheumatoid arthritis 8, 11, 12, 14, 16. Muramatsu [16] found a strong correlation between instability duration of RA and Larsen score.
Radiographic Parameters
Several radiographic methods were described to evaluate Radiocarpal and Midcarpal instability in rheumatoid wrists
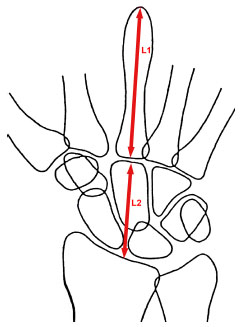
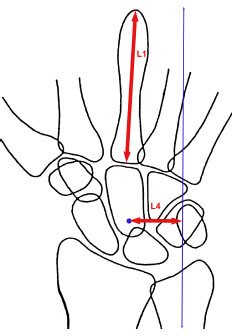
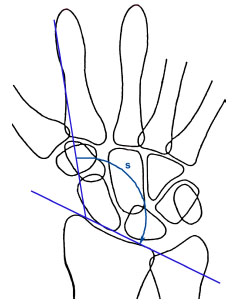
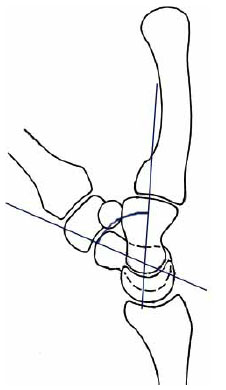
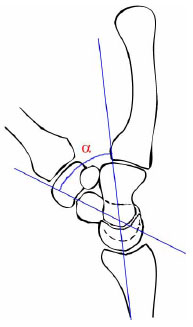
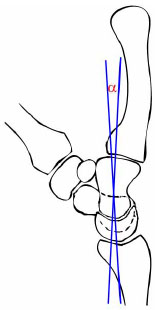
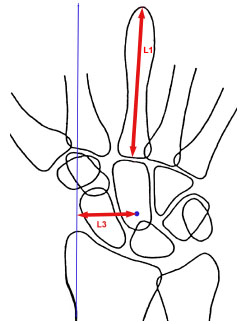
The Simmen classification 19; this is not a true radiographic classification it is merely a classification of the changing of the X-ray in time. The late stage of wrist destruction in rheumatoid arthritis was classified into three groups. I Ankylosis, II osteoarthritis and III disintegration Larsen scoring system (Table 2 and Fig. 2) [20] is based on the severity of joint space narrowing of the wrist and erosions of the wrist and the ulnar head. Carpal height ratio (CHR: Fig. 3) [21], is calculated by dividing the length of the third metacarpal by the height of the Carpus. Carpal Translation Index (CTI: Fig. 4) [22], is calculated by dividing the ulnar distance (distance from centre of the Capitate tot the centre axis of the Ulna) by the length of the third metacarpal. Radial Rotation Index (RRI: Fig. 5) [23]: The angle is measured between a line which is drawn in the longitudinal axis of the second metacarpal shaft at the radial cortex. A second line is drawn from the tip of the radial styloid at the radial limit of the articular surface to the ulnar limit on the volar side of the distal radius. Scaphocapitate angle (SCA: Fig. 6) [24]; the angle between the lines drawn at the longitudinal axis of the Scaphoid and the longitudinal axis of the Scaphoid on a lateral radiograph of the wrist Scapholunate angle (SLA: Fig. 7) [24], the angle between the lines drawn at the longitudinal axis of the Scaphoid and the longitudinal axis of the Lunate on a lateral radiograph of the wrist Capitolunate angles (CLA: Fig. 8) [24], the angle between the lines drawn at the longitudinal axis of the Capitate and the longitudinal axis of the Lunate on a lateral radiograph of the wrist. Ulnar Carpal translation (UCT: Fig. 9) [25]; this is the distance from the centre of the proximal Capitate to the line bisecting the longitudinal axis of the radius. For compensation of hand size the distance is dived by the length of the third metacarpal. Ulnar translation Index (UTI: Fig. 10) [26] Parameters for measuring collapse and translation of the Carpus. Centre of rotation of the Carpus. L1 length of the 3rd metacarpal, L2 height of the carpus, L3 carpo-stylo-radial distance. L3/L1 index of carpal translation.
Larsen Score [24].
| Modified Larsen Score | ||
|---|---|---|
| Ulnar Head | Other Wrist/Finger Joints | |
| 0 | Normal | |
| 1 | Osteoporosis, periarticular soft tissue swelling with our without minimal joint space narrowing. | |
| 2 | Erosions with normal architecture. | Erosions with joint space narrowing by at least 50% |
| 3 | Erosions sith abnormal architecture. | Moderate destruction. Obliteration of the joint space. |
| 4 | Minimum 50% loss of ulnar styloid. | Severe destruction. Joint line remains discernible. |
| 5 | Complete loss of ulnar styloid. | Mutilans. Joint line not discernible |

Larsen score [24].
Carpal Height ratio CHR [45].
Carpal Translation Index [28].
Radial rotation index RRI [35]
SCA – scapho capitate angle [26].
Scapho lunate angle SLA [26].
Capitate lunate angle [26].
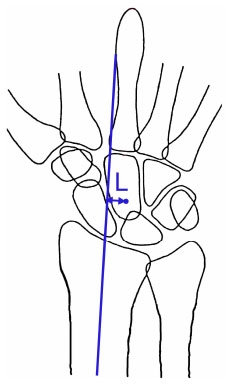
Ulnar carpal translation UCT [13].
Ulnar translation index [26].
Radio Lunate Angle (RLA: Fig. 11) [24] the angle between the lines drawn at the longitudinal axis of the Radius and the longitudinal axis of the Lunate on a lateral radiograph of the wrist.
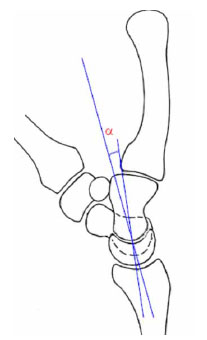
Radio Lunate Angle RLA [24].
Carpal stretch test (CST) [17] for evaluation of vertical laxity. In this test the index and middle finger are pulled; Vertical laxity is judged to be significant when the Radiocarpal joint space is at least 3 mm in width, or at least 3 mm of vertical laxity in both the Radiocarpal and Midcarpal joint.
CRITERIA FOR INSTABILITY
Some of the above mentioned tests have normal values of which instability can be deducted. Normal values are, for the Carpal height ratio (CHR): 0.54±0.03, for the Ulnar translation index (UTI): 0.28±0.03. For the Radio Lunate Angle RLA the average is -5ᵒ and if the RLA is more than +15ᵒ it means that the wrist has an dorsal intercalated instability (DISI) whilst if the RLA is less than -20ᵒ in indicates a volar intercalated segmental instability (VISI)[24]. The normal value of the Carpal Translation Index (CTI) [22] is 0.30±0.03, for the Scapho Lunate Angle (SLA) this is 46 ±15ᵒ [24], for the Capito Lunate Angle (CLA)this is 0±15ᵒ [24]. The Scapho Capitate Angle can be calculated: SCA+SLA=CLA.
Carpal stretch test (CST) [17] for evaluation of vertical laxity. In this test the index and middle finger are pulled; Vertical laxity is judged to be significant when the Radiocarpal joint space is at least 3 mm in width, or at least 3 mm of vertical laxity in both the Radiocarpal and Midcarpal joint (Table 3).
Larsen Score [24].
| Normal values: |
| Carpal height ratio (CHR): 0.54±0.03 |
| Ulnar translation index (UTI): 0.28±0.03 |
| Radio Lunate Angle RLA: average = -5°; RLA < +15° means DISI; RLA > -20° means VISI, |
| Carpal Translation Index (CTI): 0.30±0.03 , |
| Scapho Lunate Angle (SLA): 46 ±15° |
| Capito Lunate Angle (CLA): 0±15° |
| Scapho Capitate Angle: SCA+SLA=CLA |
| Carpal stretch test positive if >3mm or > 3 mm of vertical laxity |
Treatment
In 10 studies [9, 10, 12, 13, 15, 17-19]. 7 different treatment options or combinations of treatment were described.
Synovectomy
Radio-carpal and mid-carpal synovectomy increased the carpal ulnar sliding [9].
Tendon Transfer
The modified Shapiro's angle was corrected by transfer of the extensor carpi radialis longus on to the extensor carpi radialis brevis [9].
Resection of the Distal Ulna
Resection of the distal Ulna is described by Masada [15]. They found good results in the stable wrist (Simmen classification), but in the unstable wrists they found a collapse of the wrist in 6 out of 11 wrists. Simmen described that comparing carpal height ratio and ulnar translocation between non-operated and operated (dorsal wrist synovectomy and distal ulna excision) revealed no significant difference for carpal height loss. Distal ulna resection initially led to an increased ulnar translocation, however later on the ulnar translocation was similar to none operated wrists [19].
Radiolunate Arthrodesis
Radiolunate arthrodesis was described by Della Santa and Chamay [10], they concluded that it can prevent dislocation of an unstable wrist but it cannot prevent deterioration. Justen en Westenhage [13] concluded that the Radiolunate arthrodesis was successful in correcting the lunate drift in the sagittal plane.
Radiolunate and Radioscapholunate Arthrodesis
Ishikawa [12] advises Radiolunate or Radioscapholunate arthrodesis for the unstable wrist with moderate deterioration, he combines this with the Darrach procedure and tenosynovectomy of the extensor tendons.
Synovectomy Combined with Sauvé-Kapandji
The Sauvé-Kapandji procedure limited ulnar sliding and radial tilting of the carpus [9, 17].
Wrist Arthroplasty
The wrist arthroplasty has a 50% rate of failure [18].
No treatment described in the studies of Muramatsu [16] Kushner [14] and Flury [11].
The problem with all the studies that describe treatment is that it is not clear how instability is measured and how the patients are distributed among the subgroups. As there are no comparative studies that measure outcome of the different procedures.
DISCUSSION
In treating Radiocarpal and Midcarpal instability in patients with RA it is important to understand the underlying pathophysiology. There are no basic studies on that topic. However there are reports that describe assumptions on the pathophysiology.
Harrington et al. [27] stated that jointspace narrowing and carpal instability develop due to pannus resulting in disruption of articular cartilage and interosseous ligaments. A DISI pattern may occur because of disruption of the scapholunate interosseous ligament and the distal attachment of the palmar Radiocarpal ligament. A VISI pattern may be present because of synovial destruction of the ulnar carpal ligaments.
According to Stäbler [28] the start of the radiological destruction is the erosion of the SL and the RSL ligament. This leads to progressive SL dissociation. These are assumptions and the author does not give a scientific explanation.
In the study of Milz et al. [29] they found that the a high fibrocartilaginous nature of the scapholunate interosseus ligament, (and notebably the presence of aggrecan, link protein, COMP;a non-collagenous protein, and type II collagen), could explain why the ligament is an early target for destruction in the rheumatoid wrist, because it is known that in rheumatoid arthritis there is an autoimmune response against antigens known to be present in articular cartilage [30-34].
The study of Muramatsu [16] demonstrated a typical pattern of carpal instability: in the early to middle stages of the disease, the lunate flexes volarly in relation to the scaphoid. This instability is caused by laxity of the extrinsic ligaments in the proximal carpal row. Persistent synovitis eventually leads to interosseous ligament destruction, particularly of the Scapho-Lunate interosseous ligament. In the middle to late stages, the Capitate flexes dorsally. This malalignment of the Midcarpal joint may be related to laxity of the extrinsic ligaments and causes a significant decrease in Carpal Height.
There are some studies that claim that the instability starts with the caput ulnae syndrome [35]. The caput ulnae syndrome is a complex of synovial swelling and dorzalisation and instability of the caput ulna in RA which leads to painful pro and supination and reduced strength [36] tenosynovitis in the ECU leads to a elongation of the tendon. Because of a lack of counter weight to the ECRL this leads to radial deviation of the carpus. Following the chain of Landsmeer [37] and Shapiro [38] this leads to ulnar drift of the fingers. In the meantime a destruction of the SL ligament leads to a dissociation. The resulting instability will lead to a dislocation of the Lunate and the Capitate [39].
It is difficult to give criteria for instability since almost all the studies use different criteria. Arimitsu [8] defined instability as the ulnar carpal translation is 9.5 and the carpal height ratio is 0.30. Ishikawa [12] includes the patients to the study if the Larsen Dale Eek is more than stage II, the Midcarpal joint space is equal or larger than 1mm, if there is an Ulnar shift or palmar subluxation (e/MC>0.12, h/MC>0.24) and the SL dissociation has to be over 3mm. Justen and Wessinghage [13] include the patients if they are stadium IV a of Alnot [40]. Kushner [14] talks of definitive instability if the Scapholunate angle is over 80ᵒ and of possible instability if the SLA is 60-80ᵒ. Muramatsu [16] describes DISI and VISI patterns and scapholunate dissociation of over 2mm. Simmen and Hagena [19] describe instability in time but they do not have hard criteria. The studies of Chantelot [9], Della Santa and Chamay [10], Flury [11] and Masada [15] do not give criteria on which they decide if there is instability.
There are some normal values for some of the measurements. The normal Carpal height ratio (CHR) is 0.54 ± 0.03 [21], the normal Ulnar Translation Index (UTI) is 0.28 ± 0.03 [26], the average of the Radio Lunate Angle (RLA) is between - 5ᵒ and +15ᵒ. If the RLA is more than 15ᵒ means the wrist has a DISI and if the RLA is less than - 20ᵒ it means the wrist has a VISI [24]. The normal value of the Carpal Translation Index (CTI) is 0.30 ± 0.03 [22]. The normal value of the Scapho-Lunate Angle (SLA) is: 46 ± 15ᵒ [24]. The normal value of the Capito-Lunate Angle (CLA) is 0 ± 15ᵒ[24]. The Scaphocapitate Angle can be calculated by subtracting the SLA from the CLA (SCA=CLA- SLA)[24], Radial Rotation Index (RRI)[23] does not have a normal value. Ulnar Carpal translation [25] and vertical laxity of the wrist Carpal stretch test are positive if >3mm or > 3 mm of vertical laxity
The problem with all these values is that they are measured on a radiograph, while instability is a dynamic problem. The study of Arimitsu [8] tries to measure the instability on a 3D CT however in the end they still use the Ulnar carpal translation, the carpal height and SL dissociation. In the future dynamic CT or dynamic 3D fluoroscopy might be the solution, however it is not available in a lot of places around the world and it is costly especially if the examinations have to be done in yearly controls. There are some studies that describe this however not on rheumatoid arthritis patients so far [41]. There are different treatment options in literature for in stability of the wrist; Synovectomy [9] which give s good pain relief however it does not stabilize the wrist nor does it prevent further deterioration. Tendon transfer [9] can corrected the alignment of the wrist but also does not prevent deterioration. The Radiolunate arthrodesis restores carpal height and stabilizes the wrist but also does not prevent deterioration [10, 13, 42, 43]. Radioscapholunate arthrodesis can be performed if there is also deterioration between the scaphoid and the radius, but it has no advantages, nor disadvantages above Radiolunate arthrodesis [12, 42, 43]. Sauvé Kapandji procedure prevents Lunate dislocation on the ulnar side [9, 17, 44]. Total wrist arthrodesis and Wrist arthroplasty can be performed if there is a total deterioration of the wrist. There is a systematic review on fusion or arthroplasty of the wrist in rheumatoid arthritis [45], outcomes for total wrist fusion were comparable and possibly better than those for total wrist arthroplasty in rheumatoid patients. The average follow-up period was 4.5 years. The study of Ward with a minimal follow up of 5 years shows a dramatic Kaplan Meyer survival curve with a revision rate of 50% at 5 year [18]. If you take in account the high revision rate one cannot defend an arthroplasty for instable wrist in rheumatoid arthritis.
In our opinion synovectomy is accepted only in the early stages where there is no clear evidence of instability. Tendon transfer is also preserved for early stage instability without joint destruction (LDE 1-2). If there is mild joint destruction and clear instability (for instance LDE 1-2 and abnormal carpal height and ulnar translation index, or Simmen III) partial arthrodesis like Radiolunate, Radioscapholunate arthrodesis or Sauvé-Kapandji procedure should be performed. In later stages with clear Midcarpal joint destruction total wrist arthrodesis is in our opinion the treatment of choice. Maybe in the future there will be better Wrist arthroplasties that have better outcome and a lower revision rate to validate its use.
RECOMMENDATIONS FOR CLINICAL PRACTICE
On a standard AP radiograph deformity can be measured using the carpal height and the ulnar translation index of Chamay this gives an indication for instability. For describing the deterioration of the joints the Larsen score is most used. If there are also radiographs in time than also the Simmen classification can be used. For real assessment of instability dynamic radiographs are needed.
Frequent checkups are essential because RA patients are used to slowly worsening of function and pain. This may lead to late recognition of instability in a stage where there is already joint damage and only salvage treatment modalities remain.
RECOMMENDATIONS FOR FUTURE RESEARCH
A study comparing X ray results and measurement based on the X ray should be compared with dynamic CT scan or dynamic Fluoroscopy.
INFORMED CONSENT
Informed consent was obtained from all individual participants included in the study.
This article does not contain any studies with human or animal subjects.
CONFLICT OF INTEREST
The authors Eric Raven and Michel Bekerom declare that they have no conflict of interest. Author Niek Dijk is consultant for Smith and Nephew. Author Annechien Beumer is board member of the Dutch orthopaedic Lady Society, the Dutch Hand, Wrist group and consultant for the Force Foundation orthopaedic research.
ACKNOWLEDGEMENTS
The authors are grateful to Albertine van Horssen for her help with the systematic search and collecting the required articles.

