All published articles of this journal are available on ScienceDirect.

The Humelock Hemiarthoplasty Device for Both Primary and Failed Management of Proximal Humerus Fractures: A Case Series
Abstract
Fractures of the proximal humerus account for 4-5% of all fractures. Managing proximal humerus fractures operatively and non-operatively have their respective complications both short- and long-term. We present our experience using the Humelock hemiarthoplasty device for both primary and failed management of proximal humeral fractures. We present four different examples from ten cases that include a failure of internal fixation, a failure of intramedullary nailing, a complex case in a patient with multiple co-morbidities, and a failure of nonoperative management. The patients in our series had multiple injuries and the device allowed early mobilization and produced good results. We suggest that this device has a role in the failure of primary and secondary management of proximal humeral fractures in a district general hospital setting.
INTRODUCTION
Fractures of the proximal humerus account for 4-5% of all fractures and occur in a bimodal distribution, in elderly women after a low energy fall or in younger men as a consequence of high-energy trauma [1, 2]. Neer reported poor results with nonoperative management, and reported high rates of symptomatic non-union, malunion, tuberosity resorption and osteonecrosis of the humeral head in significantly displaced four part fractures managed without proximal humeral head replacement [3]. He found that patients had better outcomes with humeral head replacement than with internal fixation, and suggested this as the treatment of choice in four-part proximal humerus fractures.
Relative indications for hemiarthroplasty include fracture dislocations, significant comminution and displacement, humeral head splitting fractures and delayed presentations [4]. It is important to consider patient condition in addition to fracture factors. From a technical point of view, it is important to restore humeral height and version, and to reconstruct the tuberosities [5]. In 2008, a systematic review reported a mean postoperative forward flexion of 105°, abduction of 92° and constant score of 56 after hemiarthroplasty [6]. The common complications they recorded included tuberosity non-union (11%), heterotopic ossification (9%), proximal prosthesis migration (6.8%) and infection (2%).
We present our experience (the first in the UK) using the Humelock hemiarthoplasty (Easytech, UK) for both primary and failed management of proximal humeral fractures. Wepresent the surgical technique and four different cases from ten in which we implant.
CASE REPORTS
All the patients were operated in the beech-chair position using a deltopectoral approach.
The Humelock hemiarthroplasty is a modular implant that allows anatomical reconstruction of the tuberosities. The height and version can be reproduced using an external jig to align the height and version for each individual patient according to their anatomy. It also allows the placement of distal locking screws that prevents reliance on proximal fixation that may be limited by poor bone stock.
Failure of Internal Fixation
A 71-year-old lady sustained a proximal humeral fracture, after a period of nonoperative management the fracture displaced and was subsequently treated with open reduction and internal fixation using a locking plate. The plate cut out at 13 months postoperatively, this was revised to a Humelock hemiarthroplasty (Fig. 1).
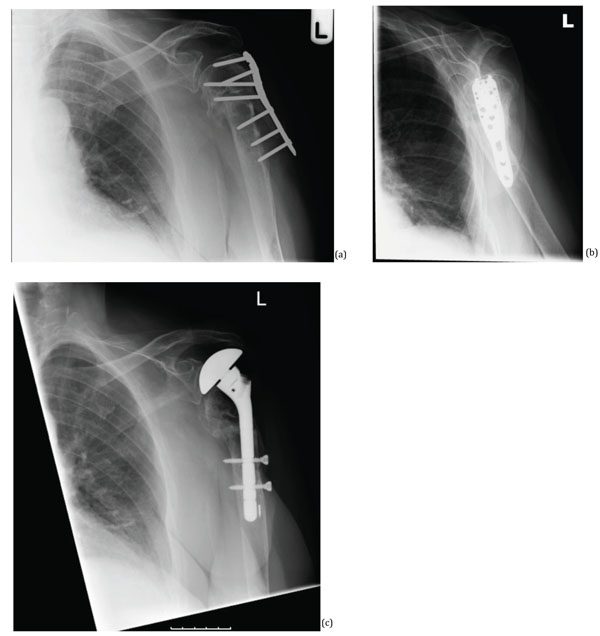
(a, b) 13 months postoperative after initial conservative management, and then with a PHILOS plate which is seen cutting out. (c) Revision using humelock hemiarthroplasty.
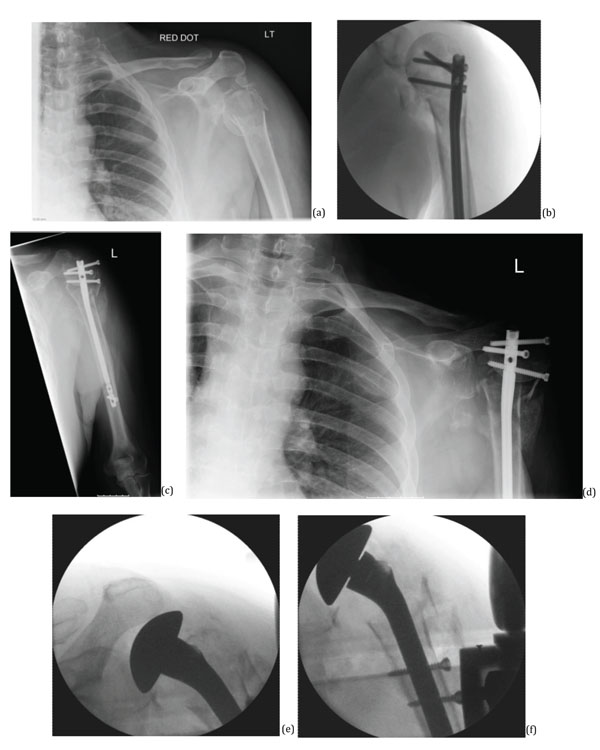
(a) Initial injury, (b) 3 days later intraoperative, (c) 8 weeks postoperatively, (d) 12 weeks postoperatively, (e, f) During revision surgery, 13 weeks following index surgery.

(a, b) X-ray after injury, (c) Intraoperative x-ray.
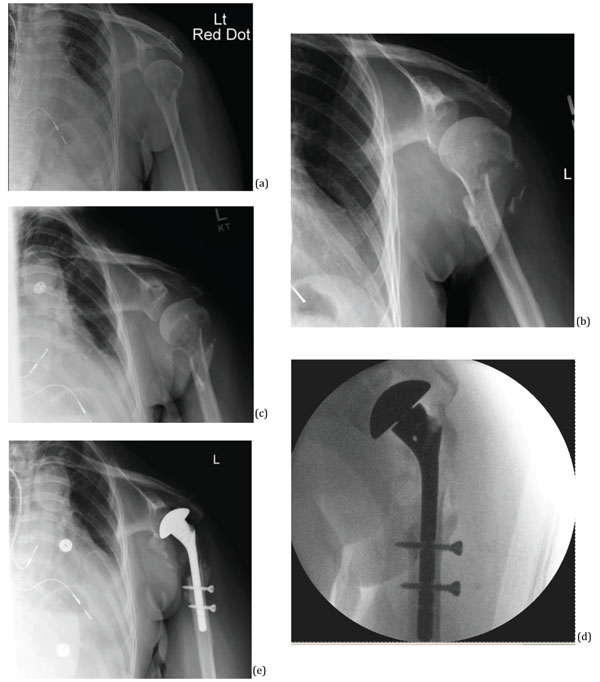
(a) Initial injury, (b) 8 weeks later, (c) 16 weeks later, (d) intraoperative (e) 16 weeks postoperatively.
Failure of Intramedullary Fixation Device
A 53-year-old male initially had a left proximal humerus fracture that was fixed with a proximal humeral nail. The fracture failed to unite and he had revision of the left humeral intramedullary nail to Humelock hemiarthroplasty (Fig. 2).
Complex Case in a Patient with Multiple Co-Morbiditiesand Trauma
A 35-year-old lady with a history of type-1-diabetes, end stage renal failure requiring dialysis, and osteoporosis, sustained a left intracapsular neck of femur fracture and a left proximal humeral fracture following a mechanical fall. The hip fracture was treated with canulated screws and the humeral fracture treated with Humelock hemiarthroplasty (Fig. 3). Postoperatively the patient was using crutches for mobilization.
Failure of Nonoperative Management
With a previous history of mastectomy and axillary node clearance for breast cancer a 69-year-old lady had non-union of her left proximal humerus fracture following a fall. Initial management was nonoperative, however there was increased displacement in subsequent clinic reviews. She had a proximal humeral biopsy, which ruled out malignancy and was subsequently managed with Humelock hemiarthroplasty (Fig. 4).
At last follow-up (12 months postoperatively) all ten patients had satisfactory ROM and the patients were able to perform hand to mouth, hand to head, hand to axilla, and hand to bottom movements.
DISCUSSION
Although the ProFHER trial [7] pointed to an equally favorable outcome with nonoperative management compared to operative management, this cannot be applied uniformly to all types of proximal humeral fractures. There is still debate amongst the orthopaedic community regarding the long-term functional outcome of these patients. Managing proximal humeral fractures operatively and nonoperatively have their respective complications both short- and long-term. Long-term follow-up of this trial might be able to answer this question; currently there is still a place for operative management.
The aim of operative fixation is to preserve the humeral head. Important factors leading to an undesirable outcome including smoking and fracture type, either non-impacted metaphyseal surgical neck fracture or fracture dislocation [3]. These are both significantly associated with osteonecrosis and secondary screw cut out, requiring revision [3]. Three or four part fractures or those with humeral head split are also at risk of developing mal-union and oseteonecrosis [8, 9]. In these instances hemiarthropalsty and reverse total shoulder arthroplasty are indicated for these complex fractures as there are higher complication rates with humeral head preserving procedures.
The position of the implant is an essential step influencing the functional result. Excessive retroversion or height can result in abnormal positioning and excessive greater tuberosity traction increasing the risk of secondary displacement [10]. Anatomical reduction of the tuberosities facilitates union and restoration of the rotator cuffs [11, 12]. Failure to restore humeral offset, defined as the distance between the centre of rotation and lateral cortex of greater tuberosity, is associated with poor functional results [13]. The optimum tuberosity position should be viewed in three planes but their respective size varies and this is a difficult technique to reproduce for every patient in every situation. If the position of the humeral stem is correct the tuberosities will also be at the correct height. Anatomical studies have demonstrated that the superior borber of the pectoralis major tendon can also be used to assess height as it is on average 5.6cm below the top of the humeral head [14]. The Humelock hemiarthroplasty utilizes the apex distance from the humeral head to the upper edge of pectoralis major as a marker for height. Attaining optimal humeral version is another technical challenge, with the prosthesis commonly placed in excessive retroversion. Ideally, the humeral implant should be in 20-30degrees of retroversion [15, 16]. Outside of this angle the force generated can cause the greater tuberosity to move out of position in the horizontal plane.
Our cases of poly-trauma, failure in nonoperative management, failure of internal fixation, and failure of intramedullary fixation show potential complications with current forms of management. These were addressed using a multipurpose device in a district general hospital setting, avoiding the need for patient transfer to a tertiary referral centre for further management or revision surgery. We have highlighted the learning curve for this prosthesis is attainable for colleagues working in district general hospitals. As shown in our case series, the benefits of this device include the ability to commence early mobilization, that is important for elderly patients and those involved in polytrauma. Thus, the Humelock hemiarthroplasty has a role in the management of failure of operative and nonoperative management of proximal humeral fractures in a district general hospital setting.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

