All published articles of this journal are available on ScienceDirect.

Revision Total Hip Arthroplasty Combined with Subtrochanteric Shortening Osteotomy: Case Report
Authors Info & Affiliations
Abstract
Revision surgery is one of the most difficult reconstructive challenges facing orthopaedic surgeons; therefore, many new techniques and implants are needed to ensure that such patient can be successfully treated. We report a 66-year old female with a chronic dislocated bipolar hip prosthesis. She underwent a revision total hip arthroplasty combined with V-shaped subtrochanteric shortening osteotomy. This report demonstrates that V-shaped subtrochanteric shortening osteotomy can be used for revision surgery. Nevertheless, this technique is not suitable for all hip revisions, and the indications and various possible procedures and devices should be carefully considered to select the best treatment for each patient. We believe that the current report provides evidence supporting a new technical option for complex cases during revision THA.
INTRODUCTION
The burden of revision total hip arthroplasty (THA) is expected to increase in many countries due to aging of society [1]. Revision surgery is one of the most difficult reconstructive challenges facing orthopaedic surgeons; therefore, many new techniques and implants are needed to ensure that such patient can be successfully treated [2-4].
In the case of a completely dislocated hip joint, subtrochanteric shortening osteotomies can be used to place the acetabular component at the true acetabulum without including nerve injury [5-8].
To our knowledge, this is the first reported case of revision total hip arthroplasty combined with V-shaped subtrochanteric shortening osteotomy for a patient with a chronic dislocated bipolar hip prosthesis. This report demonstrates that V-shaped subtrochanteric shortening osteotomy can be used for revision surgery.
The study protocol adhered to the ethics guidelines of the 1975 Declaration of Helsinki, and the study was approved by the institutional review board of Saga University. The patient was informed that this case study would be submitted for publication, and she gave her informed consent.
CASE REPORT
A 66-year old female was referred to our hospital with a chief complaint of pain in her bilateral buttocks and the need to use two crutches to walk.
She had a history of acetabular dysplasia, however, the treatment was unspecified. When she was 44 years old, she underwent bipolar head arthroplasty (BHA) with a bone graft.
No clinical signs and laboratory findings of infection were observed prior to the revision surgery.
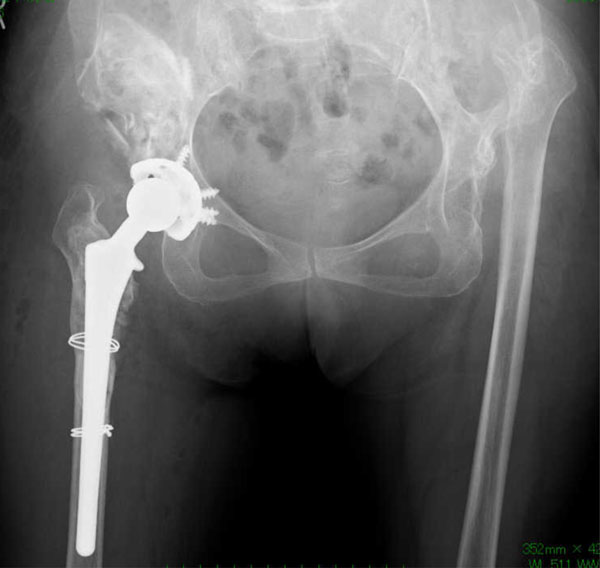
Roentgenograms showed that the implant of her right BHA had migrated proximally, and sapphire pins were placed at the new acetabulum. We concluded that she underwent BHA with a bone graft to create a new acetabulum in the high hip center, because her right true acetabulum was intact in spite of the hypoplasia. In addition to the right implant migration, her left hip joint was congenitally completely dislocated (Fig. 1).

An anteroposterior radiograph obtained before the revision surgery.
The patient then underwent revision THA combined with V-shaped subtrochanteric shortening osteotomy and allogenic bone grafting. A posterolateral approach was used under spinal anesthesia.
Around the proximal femur, there was massive metallosis which had been created from the friction between the outer head and sapphire pins. In addition, there was a marked bone defect in the proximal femur, and stem loosening was also observed.
First, the prosthesis of the BHA and sapphire pins were removed, and sufficient irrigation and debridement were performed. Placing a shell at the new acetabulum was impossibile, because there was a severe bone defect. Therefore, a V-shaped subtrochanteric shortening osteotomy was performed in order to place the shell at the true acetabulum. The V-shaped osteotomy is considered to be an appropriate surgical procedure because the osteotomy site is torsionally more stable than other types of osteotomy and the osteotomy site can be stabilized with a shorter stem. We performed the V-shaped osteotomy using a special device that was developed by Hotokebuchi et al. [5] (Fig. 2).
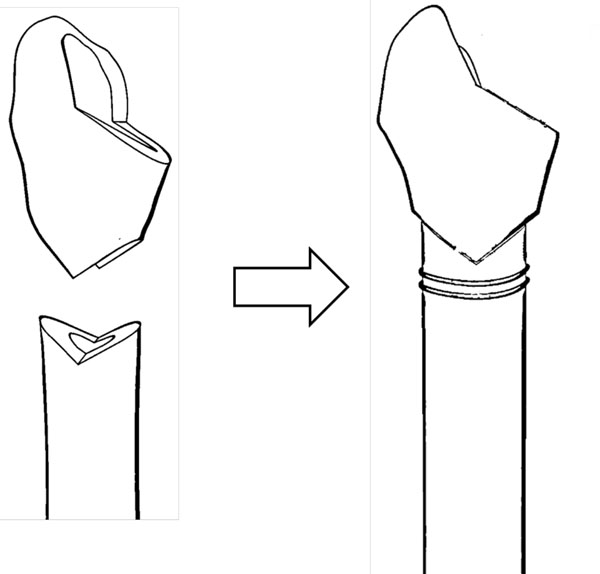
A diagram showing the V-shaped subtrochanteric shortening osteotomy.
Then, an AMS-HA acetabular shell with an AMS (polyethylene liner) liner was placed with six screws at the true acetabulum, and a cementless full hydroxyapatite-coated femoral component (a PerFix-HA Mid Size Stem) with a 28-mm zirconia ball (Kyocera, Kyoto, Japan) was used.
Morselized allogenic bone was grafted at the superior site of the shell and defect site of the proximal femur, and bulk allogenic bone was grafted at the new acetabulum (Fig. 3). The allogenic bone was frozen, and the grafts were processed aseptically. And they were not irradiated. The total length of the operation was 125 minutes, and the total blood loss was 1151 ml.
An anteroposterior radiograph taken after the first revision surgery.
Unfortunately, the patient had to undergo stem revision 26 days after the first revision surgery for a recurrent dislocation. Moreover, two months after the first revision surgery, she underwent irrigation and debridement for an infected right revisionTHA due to Staphylococcus caprae. The infection was not controlled, and two-stage revision surgery using a cement mold including antibiotics was performed to treat the infected revision THA. The femoral component was changed from a PerFix-HA Mid Size Stem to a Per-Fix HA Long Size Stem (Kyocera, Kyoto, Japan).
Thereafter, we performed THA with a subtrochanteric shortening osteotomy for the left hip. The last follow-up occurred approximately four years after the first revision surgery, at which time all laboratory findings indicative of infection remained well within the normal limits, and no clinical signs of infection were noted. The patient is currently able to walk without a cane.
Roentgenograms showed marked bone absorption at the site of the stem shaft, however, there was no evidence of instability (Fig. 4).

An anteroposterior radiograph taken at the final follow-up examinations.
DISCUSSION
During revision THA, orthopaedic surgeons therefore need to be ready for the occurrence of various difficulties when performing reconstructions. A wide variety of implants and techniques are available for revision surgery, and a clear understanding of the implants and techniques chosen is essential (e.g., proximal femoral osteotomy, impaction bone graft, modular stem, etc.) [ 2-4].
There are many types of subtrochanteric osteotomies that have been reported in the past for femoral shortening or to correct a deformed proximal femur, including transverse osteotomy, oblique osteotomy, step cut osteotomy, double-chevron osteotomy and V-shaped osteotomy during primary THA [5-8]. Moreover, various types of stems were used for such operations, including cement stems, cementless stems, long stems and modular stems.
In the revision THA cases, there have been some reports about revision THA combined with various types of subtrochanteric femoral osteotomies [9-13]. In these reports, these osteotomies were performed to correct deformed femurs, not for shortening osteotomy, during revision THA. The V-shaped subtrochanteric osteotomy was not indicated for revision THA in the past.
During a revision THA, many other types of implants have been used, because stable fixation of the stem is often difficult, especially in the cases with massive osteolysis.
The V-shape subtrochanteric shortening femoral osteotomy is reasonable for use during revision procedures in that the osteotomy site is torsionally more stable and can be stabilized with a shorter stem [5]. Therefore, regardless of the type of the stem, a V-shaped subtrochanteric osteotomy is a reasonable technique for not only primary THA, but also for revision THA.
Nevertheless, this technique is not suitable for all hip revisions, and the indications and various possible procedures and devices should be carefully considered to select the best treatment for each patient. We believe that the current report provides evidence supporting a new technical option for complex cases during revision THA.
On limitation associated with this case report was that the follow-up period was only four years. Therefore, the progression of bone absorption at the proximal femur is unclear. Further experience in terms of both longer follow-up and more patients will be necessary to fully define the safety and efficacy of this procedure.
CONCLUSIONS
We herein described a case of successful V-shaped subtrochanteric shortening osteotomy during revision THA. Although a deep infection occurred, no neurological abnormalities were observed.
CONFLICT OF INTEREST
The authors did not receive and will not receive any benefits or funding from any commercial party related directly or indirectly to the subject of this article.
ACKNOWLEDGEMENT
Declared none.

