All published articles of this journal are available on ScienceDirect.

Orthopaedic Approaches to Proximal Humeral Fractures Following Trauma
Abstract
Proximal humeral fractures have been a topic of discussion in medical literature dating back as far as 3rd century BC. Today, these fractures are the most common type of humeral fractures and account for about 5-6% of all fractures in adults with the incidence rising rapidly with age. In broad terms the management of proximal humeral fractures can be divided into two categories: conservative versus surgical intervention. The aim of treatment is to stabilize the fracture, aid better union and reduce pain during the healing process. Failure to achieve this can result in impairment of function, and significantly weaken the muscles inserting onto the proximal humerus. With the rising incidence of proximal humeral fractures, especially among the elderly, the short and long term burden for patients as well as the wider society is increasing. Furthermore, there is a lack of consistency in the definitive treatment and management of displaced fractures. This systematic review of literature compares the surgical treatment of proximal humeral fractures with their conservative management, by evaluating the available randomised controlled trials on this topic.
BACKGROUND
Proximal humeral fractures have been a topic of discussion in medical literature dating back as far as 3rd century BC (1). For many centuries the mainstay of treatment in these fractures had been the Hippocratic doctrine: forceful reduction and bandaging followed by splinting (1). In the 19th and 20th century, notable advances were made in the management of these fractures with the introduction of sophisticated splinting techniques and internal fixation for displaced fractures [1]. Today, proximal humeral fractures are the most common type of humeral fractures [2-5] and account for about 5-6% of all fractures in adults [6]. The prevalence is highest in the elderly population and the incidence rises markedly with age [6], with highest prevalence in those aged 70 years and over [7-9]. These fractures are about 3 times more common in women than men [10, 11] and the majority (about 90%) are as a result of falls from standing height [12]. Patients with poor bone quality [2] and osteoporosis are those at highest risk of sustaining this type of fracture. In fact, a study of the Finish population by Palvanen [13], showed that the incidence of proximal humeral fractures related to osteoporosis had tripled in number between 1970 and 2002. The majority of proximal humeral fractures are closed fractures meaning thatthere is no laceration of the overlying skin by the fracture of humerus [14]. It has been reported that about a fifth of all proximal humerus fractures require a surgical intervention [15].
CLASSIFICATION
Neer’s Classification
Charles Neer’s classification of the proximal humeral fractures in 1970 is the most widely used system for classifying these fractures [16]. The essence of this method of classification is based on the anatomical concepts described by Codman in the 1930s [17]. The proximal humerus subdivided into four segments 1) the humeral head superior to the anatomical neck 2) greater tuberosity 3) lesser tuberosity 4) humeral shaft. Neer argued that these parts can be affected by fracture lines, however, will be considered as a significant displacement if the segment has moved more than 10mm, or is at an angle of 45 degrees or more in relation to the rest of the segments or the humerus. Therefore, a fractured lesser tuberosity that does not meet the above criteria, is classified as an undisplaced fracture i.e. one-part fracture according to Neer’s method. A considerable number of proximal humeral fractures are undisplaced fractures. Despite the common reference to Neer that 85% of all proximal humeral fractures are undisplaced [18], a recent prospective study showed that the figure could be closer to around 50% [7]. Depending on the number of fracture lines present, the fracture can be subdivided into two, three or four part fractures. Each of these fractures, whether displaced or undisplaced can be accompanied by an anterior or posterior gleno-humeral joint dislocation, however this has been shown to be associated with a low rate of inter and intra observer reliability [19]. At times even with sophisticated imaging techniques, it may be difficult to access the fracture pattern at first presentation. This classification is not correlated with the extent to which the humeral blood supply may be affected following a fracture.
AO Classification
Muller in 1991, proposed another widely used classification method, the AO classification [20] which has been updated with the OTA association in 2007 [21]. Taking into account the importance of the blood supply this classification describes proximal humeral fractures in relation to the anatomical neck of the humerus i.e. distal or proximal. The blood supply of the proximal humerus resembles that of the proximal femur and can lead to avascular necrosis of the humeral head if compromised. The blood supply of the humeral head is mainly through the arcuate artery which comes from the ascending branch of anterior humeral circumflex artery. Its entrance into the humerus is marked by the intertubercular groove and branches off to supply the lesser and greater tuberosities and perfuses the entire epiphysis of the humeral head. If the arcuate artery was resected, the blood supply to the humeral head cannot be maintained through alternative routes such as the posterior humeral circumflex artery. This would lead to avascular necrosis. In this classification three different fracture types are introduced: Type A, B and C. Type A fractures are extra articular, unifocal, Type B extra articular bifocal and Type C intra articular [22].
Interventions
In broad terms, the management of proximal humeral fractures can be divided into two categories: conservative versus surgical intervention. Conservative management of the proximal humeral fractures involves immobilisation of the arm followed by encouraging early mobilisation through exercise and physiotherapy. This approach is generally used for undisplaced fractures, stable fractures, minimally displaced fractures, and at times even for some displaced fractures. Surgical interventions, on the other hand, are reserved for more complicated, displaced and unstable fractures. These can be summed up as:
- External fixation
- Closed reduction and percutaneous pinning
- Open reduction and plating
- Open reduction and tension-band fixation
- Anterograde/ retrograde intermedullary nailing
- Hemiarthroplasty
- Total shoulder replacement
Close reduction is performed with either percutaneous pinning or K-wires. Hemiarthroplasty refers to replacement of humeral head in contrast to total shoulder replacement where both the humeral head and the glenoid are replaced using a procedure known as reverse polarity arthroplasty. In this approach the configuration of humeral head (ball) and glenoid (socket) is reversed in that the glenoid is replaced by a ball and humeral head becomes the socket.
The management following surgical intervention involves immobilisation followed by exercise and physiotherapy.
The Benefit of Interventions
The purpose of immobilisation is to stabilise the fracture, aid better union and reduce pain during the healing process. Failure to achieve fracture union can result in impairment of function, and significantly weaken the muscles inserting onto the proximal humerus. However there are risks associated with immobilisation, especially if it is done for an extended period of time, such as pain, stiffness and significant reduction in function. The post-operative management aims to reduce or even prevent these complications, through encouraging early use of the arm, together with gentle exercise and physiotherapy. Surgery aims to stabilise the fracture and allow restoration of the joint. Once the fracture has been reduced and is stable, this will allow earlier mobilisation of both the shoulder and elbow joints. This can in turn help reduce post-operative complications such as pain, stiffness, muscle weakness or reduced functional ability. It is important to realise that there are many factors that affect the surgical outcome of the proximal humeral fractures. Factors such as patient’s age, bone quality, mobility and frailty determine the choice of intervention, length of rehabilitation and recovery time, both following trauma and further management.
The Purpose of this Review
With the rising incidence of proximal humeral fractures, especially among the elderly, the short and long term burden for patients as well as the wider society is increasing [13]. Furthermore, there is lack of consistency in the definitive treatment and management of displaced fractures [23] and recovery [24]. The purpose of this review is to compare the available randomised controlled trials in the management of proximal humeral fractures, with the intension of finding evidence whether surgical intervention is preferred to conservative treatment.
Methodology
The randomised controlled trials were searched using the electronic databases Medline, CINAHL (EBSCO), ZETOC, PubMed, EMBASE, AMED, PREMEDLINE In-Process & Non-Indexed Citations (OvidSP), ASSIA (CSA Illumina), Conference Proceedings Citation Index: Science (ISI) on Web of Knowledge, PsycINFO (OvidSP), Science Citation Index (ISI) on Web of Knowledge, Social Sciences Citation Index (ISI) on Web of Knowledge and Cochrane Library (Wiley). The following keywords were used to cite relevant articles: fractures, proximal humerus, randomised controlled trial, internal fixation, conservative management, shoulder fracture, treatment outcome, immobilisation, bandages
All available randomise controlled trials comparing the surgical management of proximal humeral fractures with conservative non-surgical approach, were included in this review.
Studies were excluded which 1) did not include conservative management of proximal humeral fractures 2) did not comment on the functional outcome 3) were not randomise 4) were not available for free viewing. A total of 17 articles were reviewed. 6 articles were identified as relevant according to the inclusion criteria.
RESULT
DISCUSSION
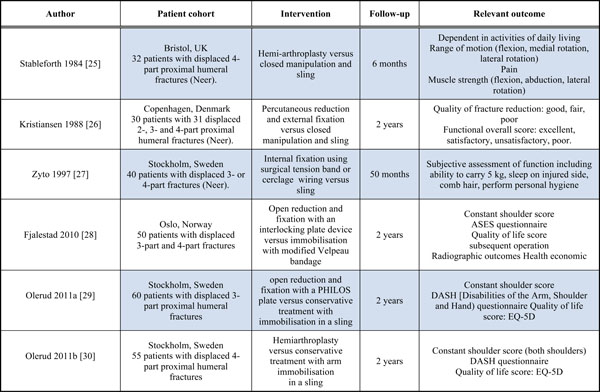
Fjalstadt [28] included 50 patients aged 60 years and over with severe displaced 3- and 4-part fracture. 25 patients were randomly allocated to conservative treatment and the other 25 had angular stable interlocking implants. They reported that at 12 months follow up there was no significant difference in the QALYs between the two groups (mean difference in number of QALYs = 0.027 Confidence Interval (CI) = -0.025,0.078).
However, there are several limitations associated with this trial, the first being the short follow up period. There are however several limitations associated with this trial. The first is the short follow up period. It is important to assess long term follow up to obtain thorough results in relation to the effect of treatment [31]. Although it has been reported that 12 month follow up is adequate in assessing the outcome of ORIF approach [32], it should be noted that the possible development of avascular necrosis of humeral head is likely to impact QALYs. Another limitation of this study is the small sample size.
Kristiansen [26] compared the functional outcome and quality of fracture reduction in 30 patients, with 31 displaced 2-, 3-, and 4-part proximal humeral fracture. The two methods of treatment compared were closed manipulation, versus transcutaneous reduction and external fixation. At 12 months follow up, they concluded that external fixation produced more favourable results in terms of regaining function, safer healing and better reduction. The quality of reduction was judged by post-operative radiography. Functional results were assessed as being excellent, satisfactory, unsatisfactory or poor according to Neer [16] scoring system, although they excluded the anatomical score.
Zyto [27] randomised 40 patients with a mean age of 74 years into two different intervention arms, comparing conservative treatment with tension-band osteosynthesis. All patients had displaced 3- or 4-part fracture of proximal humerus. They reported that the optimal functional ability was regained within the first 12 months, although the follow up period of the participants lasted up to 5 years. The main complications noted were among the surgical cohort. Despite the improved positioning and reduction in the patients treated surgically, the functional outcome as measured by the subjective assessment of function at 12 months and at final follow up was not different between the two groups.
Stableforth [25] randomly allocated a total of 32 participants with 4-part fracture into either hemo-arthroplasty intervention or closed manipulation and sling. The surgical group made a better functional recovery. This was assessed by being independent for activities of daily living at 6 months, pain score and power in flexion, abduction and lateral rotation. The hemi-arthroplasty group scored higher in all categories, although there is no statistical analysis showing that the difference in the functional outcome between the two groups is actually significant. He concluded that the closed manipulation did not result in a satisfactory outcome due to the severe soft tissue injury associated with the fractures and the detachment of the humeral head.
Olerud et al. [29] in their study of 60 participants with displaced 3-part fracture, included patients sustaining low-energy trauma with no history of previous shoulder problems. Furthermore, all participants were living independently and were not institutionalised prior to sustaining the fracture. They found that the functional outcome according to DASH and HRQol was better in the locking plate group compared to the non-surgical group. Despite this, 13% of the surgical patients had some form of severe complication which required a major re-operation. In addition to these, 17% of the locking plate patients required a second intervention in form of a minor surgical operation. They concluded that considering the risk of the surgical intervention, conservative treatment is probably the treatment of choice for the majority of elderly patients with lower functional demands. They report a potential limitation of their study being the lack of power in the comparison of randomised groups. There is also an element of recall bias due to the fact that the interpretation of quality of life data, is based on the participants’ ability to recall their health state prior to sustaining the fracture.
Olerud et al. [30] reported on the outcome of their 2 year randomised controlled trial of 55 participants with displaced 4-part fracture of the proximal humerus, treated with either conservatively or with hemi-arthroplasty. At 2 year follow-up the health-related quality of life according to the EQ-5D was significantly better in the Hemi-arthroplasty group. The results of DASH and pain assessment score were both in favour of hemi-arthroplasty. There was no difference in the range of motion between the groups.
CONCLUSION
Overall due to the mixed outcomes reported in the randomised controlled studies included in this systematic review of literature, it is hard to draw a clear cut conclusion as to which intervention is most favourable, for the treatment of proximal humeral fractures. These trials are small in terms of patient cohort and follow up period. We have concluded that there is lack of adequate evidence to suggest that surgical intervention is preferable to conservative treatment of proximal humeral fractures.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

