All published articles of this journal are available on ScienceDirect.

The Unusual Chance Fracture: Case Report & Literature Review
Abstract
The Chance fracture represents a spinal lesion caused by a flexion-distraction injury pattern. We describe a rare case of a male driver admitted at the Emergencies of our Institution, level A Trauma center. The was involved in an automobile accident without wearing a seatbelt. Radiological findings of plain radiography and computed tomography (CT) demonstrated a horizontal fracture extending across the vertebral body to the posterior elements with loss of vertebral height at the anterior aspect of T12. Based on these findings, the diagnosis of a T12 Chance fracture was established. The patient was treated conservatively with a thoracolumbar orthosis, without any subsequent disabilities. Although Chance fractures are rare lesions, they should always be considered in spinal injuries, even in cases of motor-vehicle accidents where no seatbelt is used.
CASE REPORT
A 30-year-old male was involved in an automobile accident. He was at the driver's seat and did not wear a seatbelt. During admission, his primary complain was back pain.
Upon admission, palpation revealed tenderness at the thoracolumbar region. His neurologic examination was normal with no motor or sensory deficit of the lower and upper limbs. Ultrasonography was performed to exclude blunt abdominal concomitant injuries. Simple radiographic evaluation of the cervical spine, thorax and pelvis did not demonstrate associated injuries. Radiographs (Figs. 1, 2) and CT scans (Fig. 3) of the thoracolumbar spine revealed a transverse fracture at the level of T12. The CT scan further demonstrated a split of the posterior elements, progressing anteriorly into the vertebral body. Conservative treatment was decided and the patient, following an initial period of bed rest, was mobilized wearing a thoracolumbar orthosis. Appropriate antithrombotic prophylaxis with low molecular weight heparin was administered, until full ambulation was achieved. The patient was followed up with serial thoracolumbar radiographs for the first 6 weeks of ambulation and later on, in one month intervals. The thoracolumbar orthosis was applied for three months. At the 5th month follow-up, he was pain free with radiographic signs of mild vertebral kyphosis. Upon completion of treatment, he returned successfully to pre-injury levels of daily activity, without any impairment.

Lateral radiograph demonstrating a T12 transverse fracture.
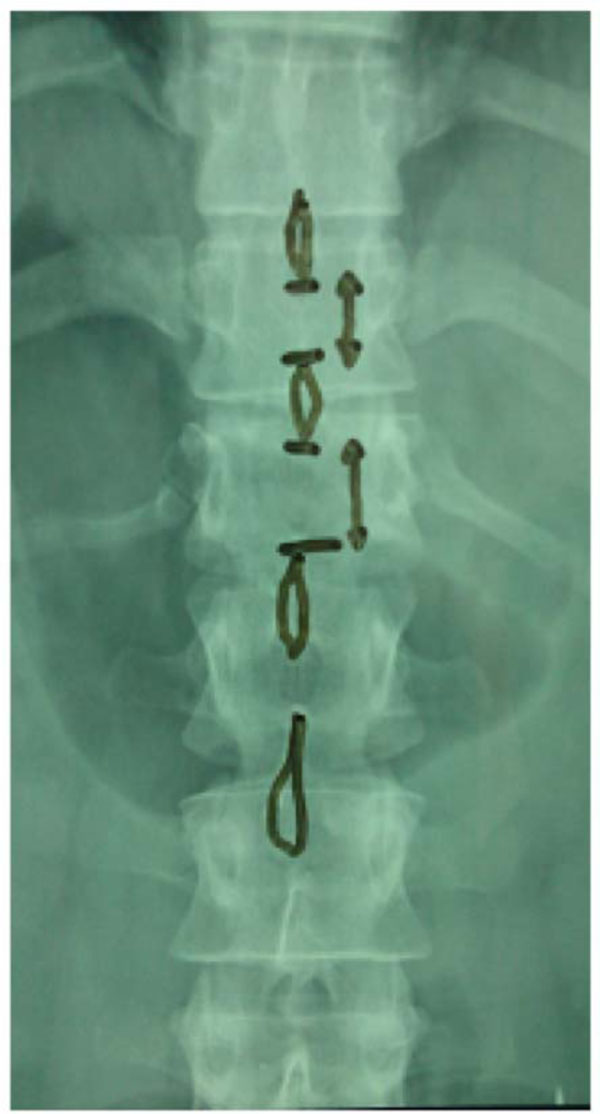
Anteroposterior (AP) radiograph demonstrating increased interspinous distance at the level of injury.

CT scan - sagittal plane, demonstrating the same T12 fracture shown in the radiographs.
DISCUSSION
Transverse fractures of the vertebra are described as Chance fractures [1]. The proposed mechanism involves a hyperflexion injury. Such fractures have been reported in adults and very rarely in children and are associated with motor vehicle injuries where a lap type seatbelt is worn [2-5]. However, this case reports a 30 year old male, involved in a high velocity motor vehicle accident, sustaining a Chance fracture of the thoracic spine in a hyperflexion type of injury, without wearing a seatbelt.
The Chance fracture consists of a horizontal splitting of the spine and the neural arch of vertebra, propagating from the posterior spinal elements to the anterior vertebral body, with no lateral displacement or rotation of the fracture fragments [2,3]. Flexion-distraction forces generated by hyperflexion of the spine over a fulcrum are responsible for the Chance fracture. Several authors have reported on lumbar Chance fractures associated with lap type seat-belts [5-7]. The proposed mechanism of injury is the deceleration which occurs in an automobile crash or a fall. During hyperflexion of the spine over a fulcrum, all spinal components are subjected to tension stress. This results either in the disruption of ligaments and posterior elements or in a combination of bony and soft tissue (ligament, and disc) injury [8,9]. Usually, Chance fractures are located at the thoracolumbar junction (T10-L2) in adults or at the lumbar spine in children [10]. However, very rarely, Chance fractures of the body of the axis have also been reported in the literature [11]. The fracture line propagates from the spinous process posteriorly throughout the lamina, pedicles, and vertebral body anteriorly.
Diagnosis is best set on good quality radiographs obtained in 2 planes (anteroposterior and lateral). As soon as the fracture pattern is recognized, appropriate reduction and immobilization usually results in a good clinical outcome. Associated intra-abdominal injuries are frequent, especially in the pediatric population [4-7]. Thus, apart from spinal trauma, intra-abdominal trauma should always be excluded at the time of admittance. If left untreated, a Chance injury may result in progressive kyphosis with subsequent chronic pain and deformity [10]. Chance fractures may generally be managed by closed reduction and immobilization in a thoracolumbosacral orthosis (TLSO) or hyperextension cast. With early recognition and management, healing can be expected in a near-anatomic reduction. After 3 months of immobilization, a rehabilitation program aiming on muscle strengthening can assist the return to preinjury activity levels. The final results may not be determined for as long as one year postinjury, with the major complaint being chronic back pain [12]. Surgery may be indicated for patients with multiple injuries or patients whose size makes closed treatment impractical (large body habitus). In those cases, a posterior approach to reconstruct the posterior tension band is preferred. The same operative approach may be used with ligamentous patterns of injury. Realignment of the spine is the goal of the surgical treatment, which is followed by stabilization and arthrodesis.
There are few reported cases of patients sustaining a Chance fracture without the involvement of a seat belt mechanism [13-16]. In this case, there was no history or evidence of an object acting as a fulcrum. However, radiological evidence was indicative of failure of the T12 vertebra in tension. The mechanism of injury appears to be acute hyperflexion of the spine that occurred when the vehicle decelerated abruptly.
CONCLUSION
The absence of seatbelt use should not falsely lead the examining physician to the assumption that a Chance fracture can be ruled out of diagnosis. A high index of suspicion based on the circumstances of the accident, may aid in the recognition of a Chance fracture. Lateral radiographs, and AP radiographs of the spine will confirm the diagnosis. Treatment options include closed reduction and immobilization with an orthosis, or open reduction and spinal fusion in those cases where conservative treatment is not possible.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

