All published articles of this journal are available on ScienceDirect.

Mechanical Quantification of Local Bone Quality in the Humeral Head: A Feasibility Study
Authors Info & Affiliations
Abstract
Objectives:
Surgical treatment of proximal humerus fractures can be challenging due to osteoporosis. The weak bone stock makes stable implant anchorage difficult, which can result in low primary stability. Accordingly, significant failure rates, even with modern locking plates, are reported in the literature. Intraoperative knowledge of local bone quality could be helpful in improving results. This study evaluates the feasibility of local bone quality quantification using breakaway torque measurements.
Materials and Methods:
A torque measurement tool (DensiProbe™) was developed to determine local resistance to breakaway offered by the cancellous bone in the humeral head to quantify local bone quality. The tool was adapted to a standard locking plate (PHILOS, Synthes), allowing measurement in the positions of the six humeral head screws, as provided by the aiming device of the plate. Two hundred and seventy measurements were performed in 44 fresh cadaveric human humeri.
Results:
Handling of the tool was straight forward and provided reproducible results for the six different positions. The method allows discrimination between the respective positions with statistical significance, and thus provides reliable information on the local distribution of bone quality within the humeral head.
Discussion:
This study introduces a new method using breakaway torque to determine local bone quality within the humeral head in real time. Because DensiProbe is adapted to a standard locking plate, there is the potential for intraoperative application. The information provided could enable the surgeon to improve fixation of osteoporotic proximal humerus fractures.
INTRODUCTION
Treatment of proximal humerus fractures, the third most common fracture in those aged over 65 years, remains a challenge [1]. The failure rate, despite the development of better implants, remains very high, being 13.7% in a study of 153 patients performed by Krappinger et al. [2]. One important reason for failure is the osteoporotic bone stock in elderly patients. The direct relationship between bone mineral density (BMD) and mechanical stability has been shown for many anatomical regions [3-5]. To assess the cancellous bone quality in the humeral head, various techniques have been used. Tingart et al. showed that the proximal half of the humeral head has a significantly higher trabecular BMD than the distal half. [5]. In a second investigation focusing on mechanical testing, they found that the superior anterior region has a significantly lower BMD and pull-out strength than all the other regions, and that the central region has a higher BMD compared to the inferior anterior region. Lill et al. found that the proximal aspect as well as the medial and dorsal regions of the proximal humerus have the highest BMD and strength [3]. High-resolution computed tomography (CT) scans of the trabecular microstructure of the proximal humerus showed that cancellous bone of the greater and lesser tuberosity presents with decreasing bone quality when analyzing increasingly deeper portions of the bone starting at the articular surface [6]. These data suggest that there may be an intraindividual variation in the distribution of local BMD within the humeral head and that standard implants may not attain the areas of best bone purchase. This could be one reason for the reported significant failure rates when using locking devices despite their superior mechanical stability having been clearly proven [7]. Therefore, the intraoperative knowledge of the local distribution of bone quality within the humeral head could be advantageous for the surgeon. A previous study introduced a torque measurement tool (DensiProbe™, ARI, Davos, Switzerland), which allows determination of local bone quality using mechanical torque [8]. A strong correlation between this method and a high resolution CT scan in the same volume of interest was shown. The purpose of the present study was to clarify whether the method provides reproducible results in a larger population and whether there is the potential for future intraoperative use.
MATERIALS AND METHODOLGY
Specimens
Forty-four unpaired fresh frozen human cadaveric humeri were processed, consisting of 21 right and 23 left humeri. Twenty specimens were of male and 24 of female origin. The mean age was 74.6 years (minimum 58 years, maximum 92 years). The bones were frozen at -20°C until processing. Prior to testing the specimens were kept overnight in a refrigerator at 4°C. The specimens were periodically sprayed with saline solution to prevent desiccation.
Instrumentation
A standard short PHILOS plate (Synthes Inc., Oberdorf, Switzerland) was mounted on the specimen in the correct surgical position as recommended by the manufacturer, using only three shaft screws. The positions of the proximal head screws, as provided by the aiming device, were numbered from 1-6 (Fig. 1). To compare the corresponding screws on the left and right sides, the positions were adapted corresponding to Table 1. Thus the placements for all the bones were adjusted to that of a right-positioned plate, with screws 1, 3, and 6 representing the posterior region and 2, 4, and 5 the anterior region of the humeral head.
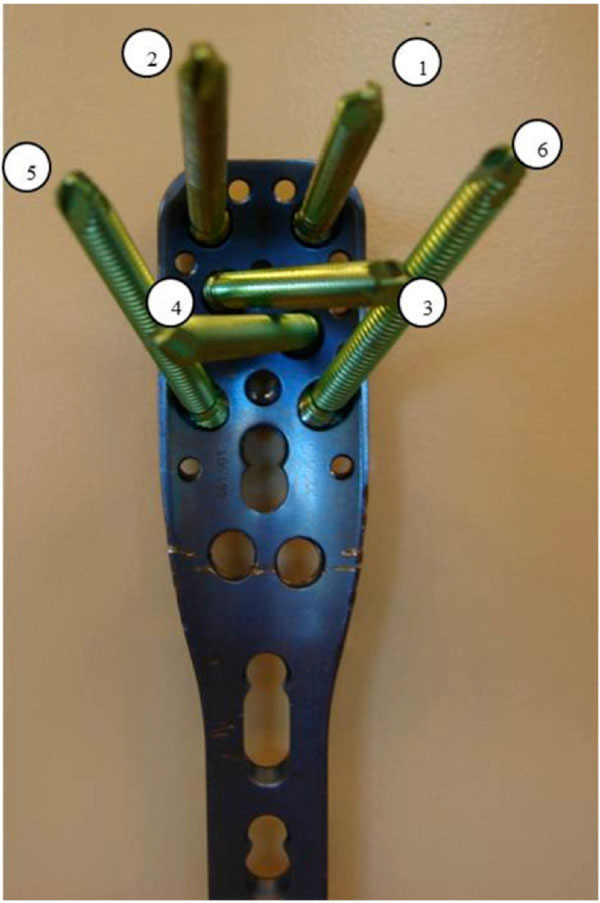
PHILOS plate (Synthes Inc.) for a right proximal humerus with the numbering system of the six proximal head screws. Screws 1, 3, and 6 aim at the posterior and 2, 4, and 5 at the anterior region of the humeral head.
Positions of the Screws on the Right Side with Corresponding Positions on the Left Side
| Right | Corresponding Position on the Left |
|---|---|
| 1 | 2 |
| 2 | 1 |
| 3 | 4 |
| 4 | 3 |
| 5 | 6 |
| 6 | 5 |
Torques Measurements
The torque measurement tool, DensiProbe™, for the proximal humerus is a 316L medical stainless steel, 115 mm long, solid cylinder with a 2.8 mm diameter, and a 25 mm long gauging tip. The gauging tip is made of three “V-shaped” depressions, 120° apart. A solid cylinder runs through a polyacetal copolymer (POM) holder that allows rotation of the solid cylinder with negligible friction. At the opposite end of the gauging tip, a bush connection allows the attachment of a torque sensor (Fig. 2). After gently hammering the probe into the bone, the sensor is rotated while keeping the probe through the POM holder and the local resistance to breakaway offered by the cancellous bone is measured. The direct relationship to the bone quality was shown in the study of Deckelmann et al. for the spine and by Brianza et al. for the humeral head [8, 9].
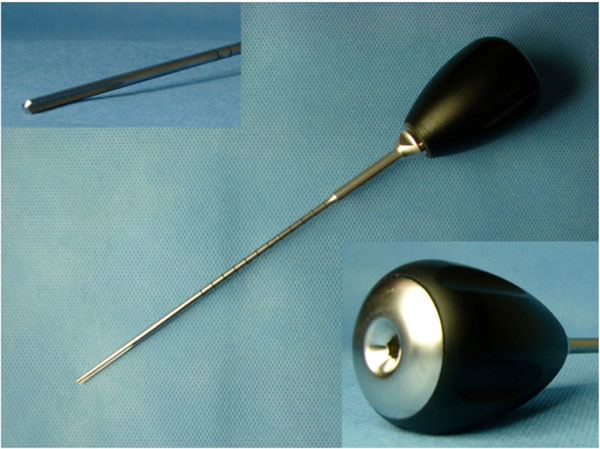
DensiProbe™ (ARI, Switzerland) for determination of local bone quality using mechanical torque. In the left upper corner the tip with three “V-shaped” depressions, which is inserted in the cancellous bone, is shown. The holder (right lower corner) has a bush connection for attachment of the torque sensor.
For application via the PHILOS plate, the aiming device for the proximal head screws is mounted. The standard centering and drill sleeve are connected. A calliper is introduced in the sleeves and the distance between the flat surface on the drill sleeve and the humeral head surface is recorded. A second custom-made measuring device is used to fix stoppers on the drill at -28mm and on the torque measurement tool at -3mm to the initially recorded distance between the flat surface on the drill sleeve and the humeral head surface. This algorithm ensures that the V-shaped depression of the 25mm probe gauging tip is fully in contact with undrilled cancellous bone at a distance of 3mm (Fig. 3). A 10-Nm range torque measuring device (MECMESIN Torque Handsensor, Mecmesin, West Sussex, UK) with an accuracy of ± 0.032 Nm at 1 Nm is connected to the torque measurement tool and rotated 120° clockwise. The peak torque recorded on the sensor display is documented as an indicator of local bone resistance.
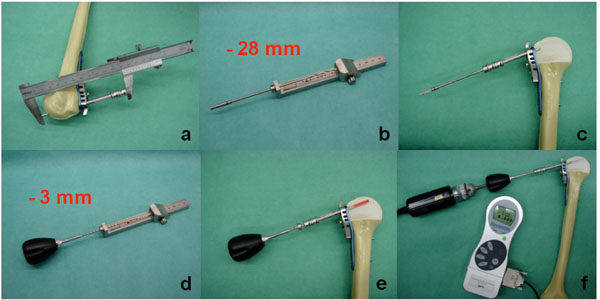
Algorithm of the torque measurement using the DensiProbe. The application is adapted to the standard tools of the PHILOS plate. A custom made caliper is used to measure the distance between the flat surface on the drill sleeve and the humeral head surface (a). The drill is set to -28mm (b, c) and the DensiProbe to -3mm (d) to that distance to ensure measurement in a 25 mm cylinder of undrilled cancellous bone at a 3mm subchondral distance (e, f).
Statistics
Statistical analysis was performed with IBM SPSS Statistics Version 21 using the Mann Whitney test based on a significance level of p ≤ 0.05. Screw positions at the same level and anterior screws versus posterior screws were evaluated for significant differences.
RESULTS
In total 270 measurements in the 44 specimens were performed. The 120° rotation always resulted in bone failure, and thus represented the maximum torque the bone could have withstood. Twenty-six measurements were excluded because of the wrong length measurement or perforation of the head. The mean torque measurement for the respective positions was 0.409 ± 0.167 Nm (position 1), 0.244 ± 0.083 Nm (position 2), 0.407 ± 0.180 Nm (position 3), 0.165 ± 0.077 Nm (position 4), 0.185 ± 0.094 Nm (position 5), and 0.379 ± 0.174 Nm (position 6) (Fig. 4, Table 2). The positions (according to Fig. 1) 4 and 5 (anteromedial or – inferior) displayed less than half the strength of positions 1, 3, and 6. Screw in position 2 had approximately half the torque of positions 1, 3, and 6. In summary, the anterior region (positions 2, 4, and 5) emphasizing anteromedial or – inferior (positions 4 and 5) of the humeral head specimen displayed the lowest trabecular stability. Statistical analysis showed highly significant differences between positions 1-2, 3-4, and 5-6 (p < 0.01). Furthermore, the analysis between anterior (positions 2, 4, and 5) and posterior (positions 1, 3, and 6) showed a highly significant difference, with p < 0.01.

Results for the torque measurements at the different screw positions with side adjustment according to Table 1. Light grey: left; dark grey: right. Positions 2, 4, and 5 represent the anterior region, having reduced trabecular stability with emphasis on the anteromedial and – inferior region (* p ≤ 0.01).
Mean Torque Measurements at the Screw Positions with Standard Deviation
| Screw Position | Left (Nm) | Right Corresponding (Nm) | Mean (Nm) |
|---|---|---|---|
| 1 | 0.457 ± 0.184 | 0.361 ± 0.137 | 0.409 ± 0.167 |
| 2 | 0.249 ± 0.088 | 0.239 ± 0.082 | 0.244 ± 0.083 |
| 3 | 0.410 ± 0.154 | 0.403 ± 0.215 | 0.407 ± 0180 |
| 4 | 0.190 ± 0.079 | 0.140 ± 0.068 | 0.165 ± 0.077 |
| 5 | 0.187 ± 0.083 | 0.182 ± 0.109 | 0.185 ± 0.094 |
| 6 | 0.436 ± 0.189 | 0.321 ± 0.139 | 0.379 ± 0.174 |
DISCUSSION
Fracture fixation of osteoporotic proximal humerus fractures remains a challenge even in the era of locking plates [10,11]. Solid implant anchorage can be difficult to achieve, resulting in limited primary stability and failure of fixation [12,13]. One reason may be the heterogeneous distribution of bone quality within the humeral head, which can lead to screw placement in areas where the bone is not of the best quality [5, 14]. However, there was no method previously available that provided information on the local bone quality within the humeral head during surgery to allow the surgeon to take this into account when performing a procedure.
The DensiProbe tool presented in this study is based on an already existing application for the femur and spine, and allows for direct measurement of local bone quality of the humeral head in real time [15,9]. The good correlation between the DensiProbe measurements and local BMD was confirmed in the study of Brianza et al. comparing the results of DensiProbe to high-resolution peripheral quantitative computed tomography (HR-pQCT) in the identical volume of interest [8]. This tool is able to evaluate the local bone quality at the provided screw site. The results of the present study represent a constant mapping of the local distribution of bone quality within the humeral head, and thus demonstrate that the method provides reproducible results. A comparison with existing studies regarding humeral head BMD is difficult, because of the different methods used to address the problem. Whereas the studies of Hepp et al., Lill et al., and Tingart et al. locate the BMD to anatomical regions [3, 4, 5], our study provides a direct measurement at the local screw site. Nevertheless, the results match in certain aspects: the posterior and proximal regions of the humeral head display a better local bone property than the anterior regions [3-5, 14]. The DensiProbe can also distinguish between different positions, such that screws aimed at the posterior region encounter a statistically significantly higher local bone quality than those aimed at the anterior region. These measurements were again consistent in all specimens. An aspect of the method which should be mentioned is the potential influence of the DensiProbe on the surrounding cancellous bone when being applied. However, its diameter is limited to its core diameter of 2.8 mm, which represents the same amount of bone destroyed as for regular pre-drilling for the screws, thus its impact, if any, would be very limited.
Although the mechanical resistance of the bone is mainly determined by the BMD, the overall bone strength depends on additional factors, including trabecular anisotropy and spacing or the remodelling state [15-18]. Using a local measurement of the breakaway torque, all these aspects are taken into account and thus provide a more specific knowledge of local bone quality, or rather properties, than from BMD. With this knowledge it is possible to take into consideration the positions where bone strength is critical and thus try to improve implant design or local stability, such as using cement augmentation of the screws. Furthermore, with the intraoperative use of this tool potentially in combination with polyaxial implants, regions with better local bone resistance could be identified and results improved [19,20].
CONCLUSION
The DensiProbe displayed consistent and reproducible results in this large sample, providing a mapping of local bone quality distribution within the humeral head, being highest in the posterior region. This method is able to distinguish between different positions within the humeral head with statistical significance. The clinical potential is considerable because it offers the possibility of real time local assessment of bone quality during surgery and could enable surgeons to adapt their procedure to the individual properties of the patient, including with cement augmentation of the screws or using polyaxial implants.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

