All published articles of this journal are available on ScienceDirect.

A Systematic Review of Dynamometry and its Role in Hand Trauma Assessment
Abstract
The dynamometer was developed by American neurologists and came into general use in the late 19th century. It is still used in various ways as a diagnostic and prognostic tool in clinical settings. In this systematic review we assessed in detail the different uses of dynamometry, its reliability, different dynamometers used and the influence of rater experience by bringing together and evaluating all published literature in this field. It was found that dynamometry is applied in a wide range of medical conditions. Furthermore, the great majority of studies reported acceptable to high reliability of dynamometry. Jamar mechanical dynamometer was used most often in the studies reviewed. There were mixed results concerning the effect of rater experience. The factors influencing the results of dynamometry were identified as age, gender, body weight, grip strength, BMI, non/dominant hand, assessing upper/lower limbs, rater and patient’s strength and the distance from the joint where the dynamometer is placed. This review provides an understanding of the relevance and significance of dynamometry which should serve as a starting point to guide its use in hand trauma assessment. On the basis of our findings, we suggest that hand dynamometry has a great potential, and could be used more often in clinical practice.
INTRODUCTION
The dynamometer ranks among the instruments developed by American neurologist which came into use in late 19th century [1-3]. William Alexander Hammond (1828-1900) described several dynamometers and the dynamograph for the purpose of assessing muscle power and graphically recording these data respectively [4]. In 1868 Mathieu, a French instrument maker from Paris, constructed Hammond’s first dynamometer and by the end of 19th century it was the most popular instrument of its kind [4]. Despite being part of the small group of diagnostic tools used in 19th century, there were several limitations associated with dynamometers [1, 4]. However, dynamometry is still used, and commonly applied to determine muscle strength [5].
Currently, various examinations and investigations can be used by clinicians in order to predict the patients’ diagnosis and prognosis. With the help of these predictions, the individuals that are at higher risk of unwanted future events can be identified, and adequate measures can be taken to reduce risks of further injuries. Assessing the muscle strength aids to spot the areas of muscle weakness and injury [6]. Accurate and quantifiable musculoskeletal testing decreases the chances of a misdiagnosis, and an appropriate rehabilitation protocol can be prescribed. Despite all these advantages, muscle strength examination is not commonly used to predict clinical outcomes, since there is a high controversy concerning its efficiency and dissimilar research outcomes retains researchers. Furthermore, there is not adequate information regarding the reliability of this instrument, thus it may be at times difficult for clinician to know how reliable different dynamometers are or what type of dynamometer to use in the first place.
Evidence has shown us that dynamometry has been used in various ways as a diagnostic and prognostic tool in clinical settings. Nevertheless, there are no articles bringing together and summarizing the various uses of dynamometry. The studies referencing the applications were searched predominantly using Medline, CINAHL (EBSCO), ZETOC, PubMed, EMBASE and AMED. The purpose of this study is to assess in detail the different uses of dynamometry, its reliability, different dynamometers used and the influence of rater experience by bringing together and evaluating all published literature in this field. This review provides an understanding of the relevance and significance of dynamometry which should serve as a starting point to guide its use in hand trauma assessment.
MATERIALS AND METHOD
The studies referencing applications of dynamometry were searched predominantly using the electronic databases Medline, CINAHL (EBSCO), ZETOC, PubMed, EMBASE, AMED, PREMEDLINE In-Process & Non-Indexed Citations (OvidSP), ASSIA (CSA Illumina), Conference Proceedings Citation Index: Science (ISI) on Web of Knowledge, PsycINFO (OvidSP), Science Citation Index (ISI) on Web of Knowledge, Social Sciences Citation Index (ISI) on Web of Knowledge and Cochrane Library (Wiley). The following keywords were used to cite relevant articles: Dynamometry, hand-held dynamometry, Dynamometer, hand trauma, Reliability of dynamometry, rater experience, mortality, survival, disability, hospital or surgery. The inclusion criteria were based on 1) using dynamometry to assess clinical outcome 2) any study evaluating the reliability of dynamometry 3) any study comparing dynamometry with either manual muscle testing or another device or both 4) any study commenting on the influence of rater experience in using dynamometry and validity of the results. Studies were excluded which 1) were any language other than English 2) did not use dynamometry to report on a clinical outcome 3) were not available for free viewing. A total of 169 articles were reviewed. 102 articles were identified as relevant according to the inclusion criteria above. All studies meeting the inclusion criteria were summarized and the relevant information was recorded in Tables 1-5 and Figs. (1, 2) depending on whether the studies assessed the reliability, different uses, different methods or devices, or rater experience related to dynamometry. Specifically in each table the authorship, sample, method and/or device and the relevant findings of the study were recorded.
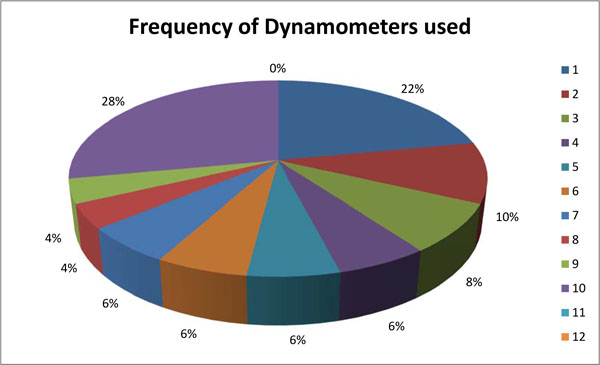
Frequency of dynamometers used in the studies reviewed.

The reported reliability of dynamometry in the reviewed studies.
General Uses of Dynamometry
| Cerebral palsy [16] |
| MB leprosy [17] |
| Huntington’s Disease [18] |
| Charcot-Marie-Tooth (CMT) disease [15, 19, 20] |
| ICU-acquired paresis [21] |
| Duchenne Muscular Dystrophy (DMD) [22] |
| cystic fibrosis [23] |
| COPD [9] |
| Ulnar and median nerve injuries [24] |
| Capsuliti [2] |
| Stroke [26-28] |
| Coronary artery disease [29] |
| Tetraplegia [30] |
| Osteoarthritis [31] |
| Hemiparesis [28] |
| Malnutrition [10] |
| Patients with disability [7, 32] |
| Pneumonia [33, 34] |
| Acute rehabilitation [35] |
| Oral and maxillofacial cancer [11] |
| Gastrointestinal cancer [36] |
| Coronary artery bypass grafting [37] |
| Liver transplant [38] |
| Rheumatoid arthritis [39] [40-44] |
| ESRD (end stage renal disease) [45] |
| chronic PD patients [13] |
| Cirrhosis [46] |
| Hip fracture [47, 48] |
| Spinal cord injury [49] |
| Haematological cancer [50] |
| Spina bifida [51] |
| spinal muscular atrophy (SMA) [52] |
Different Types of Dynamometers Used
| Number | Dynamometer | Number of Studies Using Device | References |
|---|---|---|---|
| 1 | Jamar mechanical dynamometer | 11 | |
| 2 | Sphygmomanometer | 5 | [17, 39, 40, 44, 58] |
| 3 | Smeldy hand dynamometer | 4 | [13, 32, 59, 60] |
| 4 | Kin-Com dynamometer | 3 | [55, 61, 62] |
| 5 | Harpenden hand-grip dynamometer | 3 | [47, 63, 64] |
| 6 | Martin Vigorimeter | 3 | [65-67] |
| 7 | “single spring” dynamometer | 3 | [36, 38, 68] |
| 8 | Rotterdam Intrinsic Hand Myometer (RIHM) | 2 | [15, 24] |
| 9 | BIODEX dynamometer | 2 | [25, 69] |
| 10 | Fugl-Meyer motor scale | 1 | [70] |
| 11 | Nicholas Hand-Held Dynamometer (NHHD) | 1 | [71] |
| 12 | Baseline and Grip dynamometers | 1 | [72] |
| 13 | Penny and Giles myometer | 1 | [61] |
| 14 | Hand-held electric dynamometer | 1 | [73] |
| 15 | Spring-loaded device | 1 | [73] |
| 16 | Chatillon Series D hand-held spring-scale dynamometer | 1 | [74] |
| 17 | Preston Dynamometer | 1 | [75] |
| 18 | RKK grip dynamometer | 1 | [76] |
| 19 | Therapeutics Instruments dynamometer | 1 | [77] |
| 20 | MyGripper dynamometer | 1 | [78] |
| 21 | Duffield dynamometer | 1 | [79] |
| 22 | Kratos ZM dynamometer | 1 | [46] |
| 23 | Clinifeed/Roussel dynamometer | 1 | [48] |
Combined Assessment of Reliability
| Reliability | Number of Studies Assessing Reliability | References |
|---|---|---|
| Inter- and intra- rater | 5 | [30, 49, 50, 83, 89] |
| inter- session, intra-session and test re-test | 2 | [52, 91] |
| within session test re-test | 1 | [86] |
| intra-session test re-test | 1 | [62] |
| inter- and intra-session | 1 | [88] |
| inter-rater, intra-rater and within session | 1 | [84] |
| Within-session inter- and intra-tester reliability and between session intra-rater reliability | 1 | [80] |
Summary of Studies Involving Rater Experience
| Study/Sample | Use | Device/Method | Relevant Finding |
|---|---|---|---|
| Larson et al., [49]/Individuals with spinal cord injury | Rater experience | Hand held dynamometry | measurement reliability not affected by the rater experience |
| Lindstrom-Hazel et al., [85]/73 healthy university students, faculty, and staff members | Inter-rater reliability of student assessors | Hand and pinch strength/Hand held dynamometry | occupational therapy students can be reliable in testing after training and testing for competency |
| Mahony et al., [51]/20 children with spina bifida (10 males, 10 females; mean age 9 years 10 months; range: 5 to 15 years) | Student assessment | Hand held dynamometry and Manual muscle testing | When the child is incapable of moving limb against gravity, MMT should be used. otherwise, HHD. |
| Burns et al., [30]/19 patients with upper limb weakness secondary to tetraplegia | Rater experience | Hand held dynamometry | Showed high reliability in weak elbow extensor and flexor when performed by novice examiner. |
| Goonetilleke et al., [73]/Nine muscle groups in 19 patients with motor neuron disease | Reproducibility, variability and accuracy according to rater experience | Hand-held electric dynamometer + Spring-loaded device | Greater rater experience increased the overall accuracy but not the reproducibility or variability |
RESULTS
Out of the 169 articles reviewed, 90 were found to be relevant according to the inclusion criteria. These studies were reviewed carefully and summarized in different tables according to whether they included information about the use, reliability, different types or rater experience related to dynamometry.
Onder et al., [7] studying 884 disabled women commented on the limitations of dynamometry and concluded that grip strength failed to significantly predict the onset of progressive disability of activities of daily living.Figueiredo et al., [8] reported that handgrip strength was “not associated (t-test) with total hospital length of stay, development of infection, blood use, acute cellular rejection or global resource utilization”[8].O'Shea et al., [9] reported that hand held dynamometry is suitable for testing hypotheses and monitoring changes in muscle strength in COPD patients but is unlikely to detect changes in muscle strength. Watters et al., [10] found that handgrip dynamometry cannot replace other nutritional assessment test despite being a quick, easy and reproducible test. However Guo et al., [11] found that hand grip strength is a reliable measure of the patient’s nutritional status. Similarly, Klidjian et al., [12] reported that dynamometry is a useful screening test for malnutrition that can predispose patients to major complications following surgery and Wang et al., [13] identified handgrip strength together with serum albumin to be a measure for nutritional assessment. Stokes et al., [14] used dynamometry to develop a model to categorize patients into low-effort or sincere group. Selles et al., [15] described Rotterdam Intrinsic Hand Myometer as being able to assess muscle loss more directly than grip and pinch dynamometers.
Intrinsic Hand Myometer was reported to better assess muscle loss directly than grip and pinch dynamometers [15]. Bohannon [6] states that grip dynamometer is suitable for upper limb assessment but not lower limb in which case strength knee extension dynamometer can be applied. Newman et al., [55] determined grip strength as having a higher potential to be incorporated in clinical practice compared to isokinetic dynamometry as it is easier to measure. This shows that the not all dynamometers can be suitable for similar assessments. A further issue is that the specific dynamometer employed was not always stated.
Of the 90 studies, 22 assessed the reliability of dynamometers used. Most of these reported an acceptable to high reliability of dynamometry, regardless of what aspect of reliability they were looking at. Nevertheless, some studies reported contradicting results. O'Shea et al., [9] argued that hand held dynamometry is not likely to detect changes in muscle strength for a subject with chronic obstructive pulmonary disease. McMahon et al., [80] showed that placing the hand-held dynamometer farther away from the joint centres increases the reliability of the measurements. Verschuren et al., [81] argued that inter-tester reliability of hand held dynamometry is questionable in measuring lower extremity muscle strength. Wadsworth et al., [74] found that the reliability of muscle testing using a hand held dynamometer could be affected by the rater’s gender, body weight and grip strength as these parameters affect the rater’s ability to stabilize the dynamometer. Rice et al., [82] showed that for predicting hand function while opening a select group of containers, pinch and grip dynamometry are not the most reliable tools to be used. Arnold et al., [83] assessing the inter-rater and intra-rater reliability of hand held dynamometry in 18 men and women aged 65 to 92 concluded that it is not a reliable measure for ankle strength. However, they reported that hand held dynamometry showed good reliability for isometric hip and knee strength. Another situation dependent application of hand held dynamometer was explained by Mahony et al., [51] involving a cohort of 20 children with spina bifida. They found that hand held dynamometry has acceptable inter-rater reliability unless, the child cannot move limb against gravity, where manual muscle testing should be used [51]. Interestingly Kelln et al., [84] when assessing intra-tester, inter-tester and within session reliability of hand held dynamometer found that it can be a reliable tool unless the subject can overpower the tester.
Most studies assessed the test re-test reliability followed by the combined assessment of inter- and intra-rater reliability. Results are summarized below in Tables 3 and 4.
Studies commenting on the rater’s experience and its effect on the results were also included. Larson et al., [49] claimed that the experience of rater did not affect the level of measurement reliability. Burns et al., [30] found that hand held dynamometry make and break techniques showed high reliability in weak elbow extensor and flexor when performed by novice examiner. Similarly, Lindstrom-Hazel et al., [85] showed that occupational therapy students can be reliable in testing after being trained and tested for competency. On the contrary, Goonetilleke et al., [73] reported that greater rater experience increased the overall accuracy but not the reproducibility or variability.
DISCUSSION
In this systematic review we looked at 90 papers which included the different uses of dynamometry, its reliability, different dynamometers used and the influence of rater experience in the results produced. The data was collected from a wide range of sources and the dynamometers involved were used to measure a variety of outcomes. This was not limited to hand trauma assessment. We found that dynamometry has been applied in a variety of clinical setting ranging from Charcot-Marie-Tooth (CMT) disease [15, 19, 20] to Cerebral palsy [16] and Huntington’s Disease [18]. All in all, 32 different medical applications were found in the 43 studies reviewed for the general uses of dynamometry. There are, however, very few studies looking at each individual condition.
We then identified the various types of dynamometers currently used in clinical practice. Among the 50 studies reviewed for different dynamometry devices, Jamar dynamometer proved to be the most used [8, 26, 32-34, 53-57] followed by modified sphygmomenometers [17, 39, 40, 44, 58] Smedly hand dynamometer [13, 32, 59, 60] Kin-Kom dynamometer [55, 61, 62] Harpenden handgrip dynamometer [6, 47, 63]. Martin Vigorimeter [65-67] and “single-spring” dynamometer [36, 38, 68]. However, it was found that not all dynamometers can be suitable for similar assessment. A further issue is that the specific dynamometer employed was not always stated. This could affect our results, in that we simply have more data concerning Jamar dynamometer than, say, Duffield dynamometer.
A further aim of this systematic review was to assess the reliability of dynamometry. Most of the 22 studies assessing the reliability reported an acceptable to high reliability of dynamometry, regardless of what aspect of reliability they were looking at. Nevertheless, some studies discussed situations where dynamometry is reliable, as well as when it is unreliable. Overall, we can conclude that the reliability of dynamometry depends on the type of dynamometer used and the clinical situation where it is applied. Therefore, a dynamometer having a high reliability in measuring muscle strength in one part of the body may prove to produce unreliable results when used in a different part of the body. Also, according to O'Shea et al., [9] we can assume that the reliability may vary when used in different clinical conditions. Furthermore, the reliability of dynamometry is questionable if the subject is too weak to move limb against gravity [51] or strong enough to overpower the tester [84]. According to McMahon et al., [80] the reliability is increased if the dynamometer is placed farther away from the joint centres. Other factors affecting the reliability of hand held dynamometry were listed by Wadsworth et al., [74], which include the rater’s gender, body weight and grip strength, since they influence the rater’s ability to stabilize the dynamometer. One limitation of this part of the review was that not all the studies measured the same aspect of reliability. Most studies assessed the test re-test reliability [9, 20, 31, 61, 90, 92] followed by the combined assessment of inter- and intra-rater reliability [30, 49, 50, 83, 89] as summarized in Tables 3 and 4.
There were few studies which analyzed the influence of rater experience on the results. Larson et al., [49] assessing Individuals with spinal cord injury and Burns et al., [30] examining 19 patients with upper limb weakness secondary to tetraplegia provide a straightforward conclusion that reliable results can be produced by novice examiner. Lindstrom-Hazel et al., [85] showed that occupational therapy students can be reliable in testing after being trained and tested for competency. On the contrary, Goonetilleke et al., [73] in a study involving 19 patients with motor neuron disease argues that the overall accuracy, but not reproducibility and variability, was increased with greater rater experience.
Despite the numerous positive findings in this systematic review, we should take into account the various factors which have been reported to influence the results obtained. Pincus et al., [39] distinguished between the results obtained for men compared with women and concluded that the survival rate according to mean grip strength was statistically significant in women but not men. On the contrary, Stenvinkel et al., [45] reported that low hand grip strength was a good predictor of outcome in men but not in women. In another study Pincus et al., [44] also found that the mean grip strength was not different between the patients who died and the ones who did not. Davies et al., [48] showed that handgrip strength was predictive of complications for patients over 80 but not for those under 80. Luna-Heredia et al., [72] noted that grip strength is dependent on age, gender, BMI and dominant/non-dominant hand. Wadsworth et al., [74] found that the reliability of muscle testing using a hand held dynamometer could be affected by the rater’s gender, body weight and grip strength as these parameters affect the rater’s ability to stabilize the dynamometer. Other factors include measuring upper or lower extremity strength [81], the distance where dynamometer is placed from the joint centres [80], subject not being able to move limb against gravity [51] and subject overpowering the rater [84].
Ultimately, by looking at the results of this systematic review we can conclude that dynamometry is a reliable tool that is currently being used for a wide range of medical conditions. From the results of this study we can see that only a small number of studies involved the use of dynamometry in hand trauma assessment. By looking at the general reliability of dynamometry, we can say that there would be no harm in applying dynamometry in hand trauma assessment. In fact we found a number of advantages to using dynamometry. These being due to its cheap [61-63, 69, 95] reproducible [63], sensitive [12, 68] convenient [63], quick [91], objective [91], simple [61], viable [95], portable [69, 95] and objective [31] nature. Based on the results found we suggest that dynamometry is used more often in clinical practice. At the same time we should take into account the various factors which have been reported to influence the results.
CONCLUSION
In this systematic review of the literature we have collected the available evidence concerning the reliability, general use, different types and the influence of rater experience in dynamometry. The results have been presented in Tables 1-5 and Figs. (1, 2) in the results section. It was found that dynamometry is applied in a wide range of medical conditions. Furthermore, the great majority of studies reported acceptable to high reliability of dynamometry, regardless of the different type of device or aspect of reliability they were looking at. In total, 23 different types of dynamometers were identified of which Jamar mechanical dynamometer was used most often in the studies reviewed. There were mixed results concerning the effect of rater experience. The factors influencing the results of dynamometry were identified as age, gender, body weight, grip strength, BMI, non/dominant hand, assessing upper/lower limbs, rater and patient’s strength and the distance from the joint where the dynamometer is placed. Due to its numerous advantages found in this review, we suggest that hand dynamometry has a great potential, and could be used more often in clinical practice.
CONFLICT OF INTEREST
None declared.
ACKNOWLEDGEMENT
None declared.

