All published articles of this journal are available on ScienceDirect.

The Use of the S-Quattro Dynamic External Fixator for the Treatment of Intra-Articular Phalangeal Fractures: A Review of the Literature
Abstract
Intra-articular phalangeal fractures are a common injury. If left untreated, these injuries can lead to poor functional outcome with severe dehabilitating consequences, especially in younger patients.
The S-Quattro external fixator device (Surgicraft®, UK) can be used to treat such injuries. Its use has been widely documented and has shown many advantages in comparison to other conventional treatments. Advantages include reduced operative time, rigid fixation and early range of motion.
We present a review of the current literature and use of the S-Quattro serpentine system in the management of intraarticular phalangeal fractures.
INTRODUCTION
Phalangeal fractures of the hand are common injuries, especially in contact sports. In younger patients, with higher functional demands, the effects of suboptimal treatment can be devastating.
The average accident and emergency department will see several hundred each year, with causal factors including falls and road traffic accidents. More commonly in sport, especially football and cricket, the injuries may be severe [1]. It is estimated from current literature that approximately 18% of all phalangeal fractures extend into a joint. In most cases, the proximal interphalangeal joint and 8% are associated with comminution. Such injuries are associated with considerable morbidity, the main problem being stiffness and deformity [1].
The management of displaced intra-articular phalangeal fractures of the hand is difficult, challenging and controversial. These joints are uniquely susceptible to injury due to their limited, singular plane of motion. Most phalangeal and metacarpal fractures can be managed conservatively by temporary splintage followed by rehabilitation [2]. Immobilization in extension has shown varying result, with finger stiffness being the main problem.
Displaced comminuted intra-articular fractures pose many problems to the surgeon. Displaced comminuted phalangeal fractures or intra-articular fractures, especially where more than 40% of the joint surface is involved, present the greatest difficulties. Common associated with intra-articular phalangeal fractures include angulation, flexion deformity, malrotation, malunion, joint stiffness and joint subluxation [3]. The relative indications for operative intervention include displaced intra-articular fractures, failed conservative treatment in unstable fractures, multiple fractures and open fractures with associated soft tissue injury [2].
To achieve a successful outcome in the majority of case, it is prudent to initiate to early mobilization. This is appropriate for minor avulsions and other stable fractures, however, in complicated injuries, a more aggressive approach is required. Various different techniques have been advocated, but treatment of these difficult fractures is often complex and inconvenient for the patient [1].
Fahmy (1990) and Fahmy & Harvey (1992) described treatment of such fractures using a dynamic external fixator [2]. Treatment relies on the concept that the fixator applies traction but also allows some movement of the involved, injured joint. This concept enables that early mobilization is clearly without jeopardizing the accuracy of the fracture reduction [4].
The S-Quattro (Surgicraft Limited®, Redditch, UK) is an external fixator designed to treat displaced comminuted intra-articular phalangeal fractures which works on the principle of ligamentotaxis to reduce and hold the fracture. The system is elastic and this allows some movement of the affected joint [2, 4]. An arthrodiastasis is maintained throughout a limited range of motion of injured joint effecting moulding of the articular cartilage and restoration of joint congruency [2].
PATTERN OF INJURY
A spectrum of joint injury pattern occurs depending on the direction, rate and force of loading. Pilon-type injuries can occur if the loading force is severe and axially directed. Such fractures are characterized by comminution that involves the whole phalanx base and are associated with central depression or splaying of the concave articular surface (in the coronal plane, sagittal plane or both) [3].
When force is directed from the dorsal or palmar direction, a fracture of the corresponding lip of the articular surface is likely to ensue. This may be associated with a dislocation or a subluxation. When the fracture involves a significant proportion of the articular surface, subluxation occurs [3].
Other fracture patterns include unicondylar and bicondylar fractures. Literature review suggests poor results are achieved in on-operative management of these injuries, which usually comprises of immobilization with splintage. Complications associated with this method of treatment include pain, stiffness and reduced range of motion. For best functional results, it is important for any subluxation to be reduced efficiently and early mobilization instigated. Although these fractures can usually be reduced by the traction principle, methods of maintaining reduction until the fracture has united are difficult and often compromise joint movement [3].
Stiffness is a particular problem with the proximal interphalangeal joint (PIPJ) whose normal range of movement exceeds that of the distal interphalangeal joint (DIPJ). This contributes considerably to grip strength. Fractures that involve the PIPJ, can often lead to dorsal subluxation of the base of the middle phalanx, and lthough stable in flexion, it is undesirable to immobilize the joint to prevent future stiffness.
CONVENTIONAL TREATMENT METHODS
Closed reduction with zimmer splintage or volar slab may be adequate for simple fractures, but may not always prevent recurrent displacement and also risks future stiffness.
In many cases, open reduction and internal fixation (ORIF) may become necessary after failure of splintage to maintain reduction. In such fractures, single large fragments may be held with Kirschner wire (K-wire) fixation introduced (either percutaneously or open) or by AO screw fixation. As with all surgical procedures, there are associated complications. These include risk of tendon adherence, ligament and capsule fibrosis and avascular necrosis of the fragment. Trans-articular K-wire fixation precludes early mobilization and further damages the healthy articular surface [3].
Much of the current literature for more comminuted or severely compound injuries suggests poor results. Intra-articular unstable fractures with comminution and a depressed fragment very often have no satisfactory treatment. This compromises patient care and renders the patient susceptible to future surgery. The patient inevitably has to accept the deformity and later be considered for corrective osteotomy, arthrodesis or even joint replacement [3].
THE S-QUATTRO SYSTEM
The Stockport Serpentine Spring System or S-Quattro (Surgicraft®) is a flexible mini external fixator designed to treat comminuted unstable intra-articular phalangeal fractures [1]. It consists of a unique, dual, parallel but opposing action, spring column system and was devised by Fahmy (1990). It has now become a well established successful system in the management of intra-articular phalangeal fractures of the hand [3].
There are advantages of the S-Quattro system over conventional methods of fixation. Amongst those documented, these include a relatively lightweight system that is effective in the management of fracture dislocations; a reduced operative time; distraction of joints in different degrees of flexion, extension and radial-ulnar deviation; allowing of movement in intra-articular fractures and its’ use in some compound fractures and in cases of mal-union.
The S-Quattro system works on the principle of ligamento-taxis, reduction being achieved and maintained by tension in the joint capsule and ligamentous structures produced by dynamic distraction. It is a flexible system and therefore allows early active mobilization and guards against tendon adherence [1].
PRINCIPLES OF FIXATION WITH THE S-QUATTRO SYSTEM
There are two main principles in managing intra-articular fractures; [3] maintaining congruency of the joint by reduction and stabilization of fragments and [2] promoting early joint mobilisation.
By maintain joint congruity, it aid in the prevention of joint stiffness and allow pain free movements by allowing free gliding of adjacent tendons. This inevitably causes less pain and reduces long term arthritis. Vidal et al., described the principle of ligamentotaxis and demonstrated how simple traction can be used to reduce displaced and comminuted fractures by tightening various ligamentous and capsular structures. This principle is now in everyday use in the management of various types of fractures [3, 4].
Early joint mobilisation reduces swelling and facilitates joint nutrition, surface remodelling, contouring and healing. It guards against tendon adherence and subsequent joint stiffness. It also prevents the fibrous thickening of collateral ligaments and contractures of the palmar plate with subsequent restriction of extension. Traction by application of the external fixator prevents shortening of the ligaments, which would otherwise contribute to joint stiffness.
Conventional methods of treating intraarticular phalangeal fractures have proven difficult in obtaining and maintaining anatomical alignment and stable fixation to allow early motion. In contrast to existing techniques, the S-Quattro external fixation device works on the principle of ligamentotaxis, which overcomes the potential difficulties described. It has the advantage of restoration of the articular surface and early joint motion. Even though, the S-Quattro system results in limited movement at the injured joint, it allows free movement of the other digital joints. This reduces swelling, prevents tendon adherence and allows quick recovery after the removal of the external fixator [3]. In most units, the common practice is to remove the device between 4 to 6 weeks post application.
SURGICAL TECHNIQUE
The surgeon may perform the operation under general or local anaesthesia. The S-Quattro system consists of two modified K-wires and two serpentine springs [1]. Manual traction is applied to the finger tip of the injured joint and is gently distracted. This allows correction of the deformity (angular or rotational) [5]. The unthreaded notched wires are introduced using a power drill percutaneously through the dorsal or mid lateral approach either side of the injured joint [1].
The device manufacturers’ (Surgicraft, UK), suggest that if the If the dorsal approach is chosen the distal pins should be inserted in the bare area just distal to the insertion of the central slip to avoid the extensor tendon. The proximal pin is inserted through a small incision splitting the extensor tendon longitudinally to avoid transfixing it with the pin. Both pins should be inserted in sagittal plane. Furthermore, in the mid-lateral approach, the pins should not be introduced through the phalangeal necks. The mid lateral approach is reported as technically more difficult and does not allow the distal interphalangeal joint to be placed in 30° flexion, which is stated as the optimum position [1]. Repeated attempts at introducing the pin at the same level should be avoided due to the risk of fracturing the phalanx. It is advised that the pins are inserted through the most convex part of the shaft [5]. Both cortices must be breached and in the same cortical plane.
The springs are then inserted between the two pins (in the first or second grooves) near the tapered ends [5]. The stiffer spring is applied first (to act as a fulcrum), and the second spring applied to provide distraction [1]. By bringing the free ends of the pins closer, a greater degree of distraction is achieved and by placing the second spring further away from the finger maintains the distraction [5]. This allows the system to achieve distraction or compression of the fracture as appropriate or in the neutral format [1]. Tension in both the ligaments and capsule maintains the reduction and prevents rotation. All other joints remain mobile, with the use of the hand remaining intact whilst the external fixator is applied [1].
A check X-ray should be taken to confirm a satisfactory positioning of the device and reduction of the fracture. The procedure is completed by applying gauze dressings over the pin ‘entry’ sites and adhesive dressings should be used to secure the junctions between the pins and the springs. The pins and serpentine springs need to be trimmed and gauze dressings applied over the sharp ends [5]. The device is secured with adhesive ('plastic padding') and further protection is afforded by gauze dressing and a 5cm elasticated cling bandage (3) (Figs. 1-3).
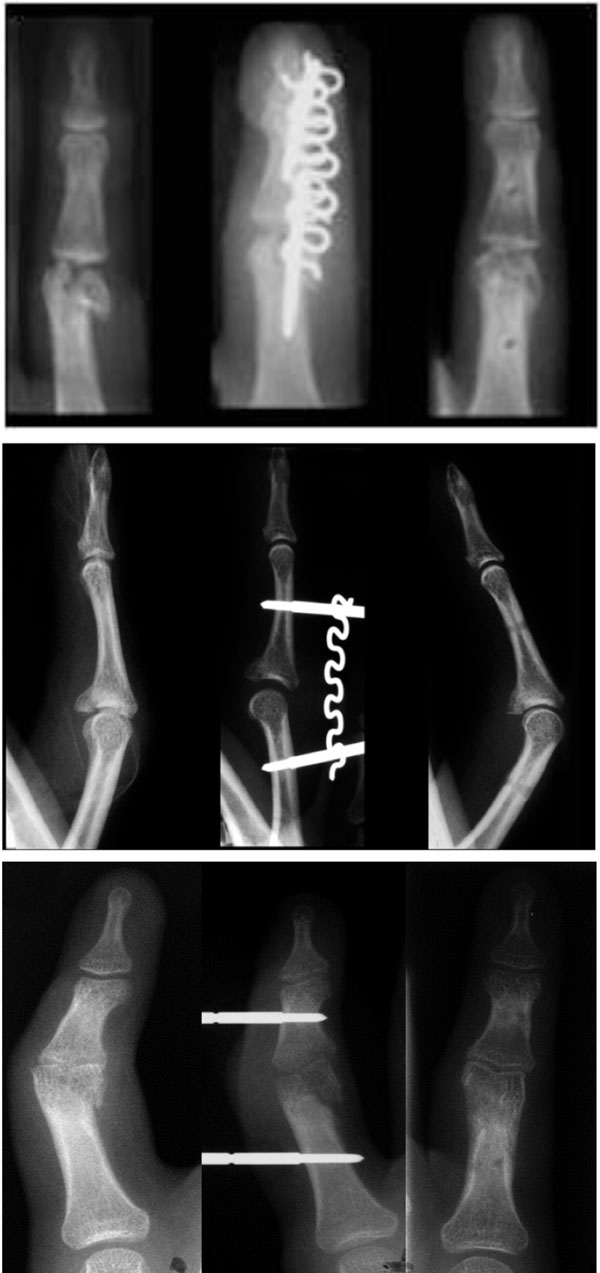
Three sets of radiographs for phalangeal fractures managed with the S-Quattro external fixator and radiographs at final follow-up.
Post operatively, the patients are encouraged to exercise the finger regularly to prevent complications.
CURRENT EVIDENCE
Since its’ introduction two decades ago, evidence supporting the use of the S-Quattro in the surgical management of intra-articluar phalangeal fractures has now become widely documented. Although a great number of clinical trials have not been conducted, those that have demonstrate promising results. Results from the original studies using the S-Quattro device have been shown to be reproducible in both large regional hand units and smaller district general hospitals.
Table 1 summarises the main clinical studies involving the use of the S-Quattro fixator in the management of these injuries.
Summary of Outcomes Following Treatment with S-Quattro Fixation
| Author | Study Type | No. of Patients | Age | Mean Follow Up (Months) | Injuries | Operative Technique | Outcomes | Patient and Radiographic Satisfaction | Complications |
|---|---|---|---|---|---|---|---|---|---|
|
|
|||||||||
| Byrne AM et al., 2008 | Prospective | 10 | Mean 31 (18-69) | 10.7 (7-21) | All involving base of thumb
8 Rolando 3 bennett 1 open comm 1 frac/disloc |
Removed mean 4.9 weeks | Mean loss Total Active Motion 7.5 degrees 5/10 lost >10 degrees -2/5 lost >20 degrees | Mean DASH score at 3 years 3.4 | None stated |
|
Total Active Motion 4/10 Excellent (100%) 6/10 Good (76-99%) |
|||||||||
|
|
|||||||||
| Khan WS and Fahmy N, 2006 | Retrospective | 100 | Mean 39.3 (18-94) | 10.5 | PIPJ – 81
DIPJ – 10 MTCJ – 6 IPJ Thb - 3 |
LA Day case | Mean Arc Degrees
PIPJ – 92 (60-120) DIPJ – 82 (65-100) MTCJ – 91 (90-95) IPJ Thb – 80 (80) |
Patient:
PIPJ – 79/81 DIPJ – 10/10 MTCj – 6/6 IPJ Thb – 3/3 |
2 devices dislodged and needed to be resited |
| Total Active Motion
PIPJ – 255 (225-280) DIPJ – 274 (260-280) MTCJ -274(265-280) IPJ Thb – 113 (110-115) |
Radiographic:
PIPJ – 76/81 DIPJ – 10/10 MTCj – 6/6 IPJ Thb – 3/3 |
||||||||
|
|
|||||||||
| Khan W and Fahmy, 2006 | Retrospective | 20 | Mean 34 (18-51) | 14 (7-20) | PIPJ – 15
MCPJ – 2 DIPJ – 2 IPJ Thb - 1 |
LA Day case | Mean arc Motion 94 degrees (80-120) | Patient 20/20 | 1 device dislodged and resited |
| Removed 4-6 weeks | Mean DASH score 5 (0-12) | ||||||||
| VAS 18/20 no pain, 2.20 minimal pain | |||||||||
| Radiographic 20/20 | |||||||||
|
|
|||||||||
| Mullet JH et al., 1999 | Prospective | 39 | Mean 29.2 (16-64) | 22.5 months | 30 intra articular 7 extra articular | LA Day Case Removed 4-6 weeks |
Intra articular Mean Arc Degrees 72 |
None stated | 2 pin site infections – no sequelae |
|
Total Active Motion Finger 232 Thumb 123 |
2 loosening of pins – no sequelae |
||||||||
|
Extra articular Mean Arc Degrees not stated Total Active Motion Finger 241 Thumb 125 |
1 poor patient compliance and late reattendance, led to fixed flexion deformity |
||||||||
|
|
|||||||||
| Bostock SH et al., 1993 | Prospective | 11 | Mean 34.2 (19-51) | 12.6 (6-28) | 10 PIPJ 1 MCPJ |
Removed 3.5 weeks | Mean Arc Motion 88 (75-110) | Patient 11/11 | 1 patient aged 45 had stiffness which improved post tenolysis |
|
|
|||||||||
| Fahmy NR and Harvey, 1992 | Prospective | 14 |
Malunited 28 (11-44) |
Malunited
11.4 |
Malunited PIPJ – 4 DIPJ 1 |
Malunited Removed 3.6 weeks |
Malunited Mean arc motion 85 degrees (50-105) Mean Total Active Motion 257 degrees (230-280) |
None stated |
Malunited 1 patient had pin loosening |
|
Comm Condylar 27.4 (21-38) |
Comm
Condylar 12 (6-24) |
Comm
Condylar 5 patients |
Comm
Condylar Removed 4 weeks |
Comm Condylar Mean arc motion degrees 76 (45-95) Mean Total Active Motion 190 degrees (90-250) |
Comm
Condylar 1 pin site infection -no sequelae |
||||
|
Comm Compound Fractures 34 (12-32) |
Comm
Compound
Fractures 15 (12-24) |
Comm
Compound
Fractures 4 patients |
Comm
Compound
Fractures Duration not stated |
Comm Compound
Fractures Mean Total Active Motion 198 degrees (160-250) |
Comm
Compound
Fractures None stated |
||||
Fahmy (1990) reported the use of the S-Quattro in 20 cases of intra-articular phalangeal fractures. In most cases the fixator was applied in the first week following fracture, the longest interval from injury to application being 21 days. Fahmy left the device in place for 2-6 weeks. A minimum of 6 month follow-up was achieved with the mean range of movement recorded as 81% was possible in the affected joints. In the majority of patients, movements were pain free after removal of the device. No pin tract infections were reported [1, 6]. Furthermore, early controlled mobilization restores the congruity of the joint surface preventing stiffness and later arthritis.
A further study by Fahmy & Harvey (1992) of 14 cases of displaced intra-articular phalangeal fractures (5 mal-unions, 5 comminuted condylar fractures, 4 communited compound fractures; mean presentation 31 days post injury) yielded good results. They showed a mean total deformity (angular, flexion and rotation) at the start of treatment of 70°. The mean residual deformity after an average 11.4 months follow-up was 14° [1, 7].
In a study of 37 patients treated over a 7-year period using the S-Quattro system, Mullett et al., (1999) demonstrated a good outcome. 30 fractures were intra-articular and nine extra-articular. The average follow-up was 22.5 months. Indication in all 30 cases was a displaced intra-articular fracture. The average total range of motion for the affected digit at follow-up was 232° for intra-articular and 241° for extra-articular fractures. The external fixator device was removed at 4-6 weeks [1, 2].
Khan et al., (2006) conducted a retrospective study for acute intra-articular phalangeal fractures of the hand using the S-Quattro. One hundred patients with a variety of fractures underwent fixation over a 6 year period, with all fractures involving a single joint. All were closed injuries and mean follow up was 6 months. Results compared favourably with those in other published series. Interestingly, from their study, Khan et al., noted that patients regained more movement and less pain following the second 6 months of the first year. A similar trend was also shown by Fahmy (1990), with favourable results expected if the patients are less than 40 years of age, have no associated osteoarthritis and are treated within 1 week of injury (Fahmy, 1990) [6].
Other trials demonstrate similar results. Byrne et al., (2008) reported outcomes in 10 patients who underwent S-Quattro external fixation for complex fractures of the base of the thumb. Between 1996 and 2003, 9 men and one woman (mean age of 3 years). The dominant hand was involved in 8 patients. Three patients had Bennett fractures, 5 had Rolando fractures, one had an open multi-fragmented fracture, and one had a fracture-subluxation. Mean follow up of 10.7 months. The mean loss of total active movement (TAM) at the carpometacarpal joint was 7.5°. After a mean of 41 months of treatment, the mean disability of arm, shoulder and hand (DASH) score was 3.4. This study therefore also demonstrates a good outcome for complex intra-articular base of thumb fractures fixed with the S-Quattro system [8].
Studies of injuries were sustained during sports also demonstrate a good outcome with the use of the S-Quattro system. Bostock et al., (1993) examined 11 consecutive sports injury cases in which the S-Quattro was used phalangeal fracture sustained during sports (19 to 51 years of age). The fracture was displaced, comminuted and intra-articular in all cases. None of the injuries was compound. 10 patients had a good range of movement at the injured joint (75-110°), whilst in one case there was marked stiffness (35°), which was subsequently improved with tenolysis (55°). 73% of patients were pain free; all were satisfied with the outcome of surgery [1].
Furthermore, the largest series of patients with sports injuries treated with the S-Quattro revalidates the results produced by Bostock et al., (1993). 20 patients were treated over a three-year period (Khan et al., 2006). Results demonstrated an average arc of movement of the affected joint of 94° at a mean follow-up of 14 months. The mean DASH score was 5 indicating mild impairment. 100% of the patients were satisfied with the results following surgery thus reinforcing the argument for the routine use of the S-Quattro in difficult sports injuries [9].
DISCUSSION
The S-Quattro system has gained popularity over recent years supporting evidence grows. It owes its success to many of the attributes this external fixator possesses. The device is a light, dynamic, and versatile system, which enables distraction of the injured joint and controlled movement of uninjured joints to maintain joint congruency [8].
Use of the S-Quattro has been reported in a spectrum of hand traumas and is a versatile device with an increasing range of applications [4]. The Stockport Hand Unit reports good results following trapeziectomy or excision arthroplasty of the proximal interphalangeal joint. Other indications include intra-articular comminuted phalangeal fractures, fracture-dislocations to mal-united phalangeal fractures. Modifications of the S-Quattro device have also been used for treating neglected dorsal interphalangeal dislocations and chronic subluxation at the proximal interphalangeal joint [8].
It is particularly suitable where fragments are too small to fix and where comminution affects the joint surface. The device achieves and maintains excellent reduction, prevents deformity and allows early mobilization of the affected joint. The procedure is short and straight forward, complications are few, and functional results are surprisingly good considering the severity of these injuries and the inadequacy of other treatment [4].
Several other techniques of distraction have been described; all with varying results. All have demonstrated advantages and disadvantages in the treatment of phalangeal fractures. Thus far, there has been no review comparing the outcomes of these treatments. However, all treatments have problems associated with their use, which are complexity, infection and loosening. Examples include external fixators [10], pins and rubber traction systems [11], dynamic springs [12], force couple splint [13], dynamic longitudinal traction [14] and compass hinges [15]. Discussion of these treatment modalities is beyond the scope of this review.
Principal indications for using the S-Quattro are displaced and comminuted intraarticular phalangeal fractures [1]. Anatomic reduction is achieved by capsuloligamentotaxis which and provides stability for fracture healing with early active digital movement [8]. Compared to traditional treatment modalities such as splinting and Kirschner wiring, the S-Quattro appears to provide superior results according to current literature regaining and maintaining at the congruity of articular joint surfaces, on the basis of many clinical trials demonstrating good clinical outcomes [8]. Much of the literature is in favour of early mobilisation to prevent future stiffness and indeed, return of hand function in young working patients is an essential goal.
Many advocate the use of this system in injuries that may be difficult to treat successfully with conventional methods. The surgical technique described previously, enables accurate reduction with minimal soft tissue dissection and is relatively straight forward procedure with reduced operative time [2]. Open phalangeal fractures can be easily stabilised whilst preserving soft tissue and this device overcomes the need for extensive soft tissue dissection for fracture fragment fixation, and avoids ensuing complications such as avascular necrosis [6]. Fahmy & Harvey (1992) showed good results in compliant patients in treating intra-articular-subluxations that were treated within 2 weeks of the injury. They suggest that their results are transferrable to regional trauma units [2].
Many of the papers discuss technical point for use of the S-Quattro system. Some suggest avoiding excessive tension on the Serpentine springs when attempting reduction, as to avoid overdistraction of the joint and resultant stiffness [2]. In those intra-articular fractures where there is a single fragment of sufficient size, it may be fixed with a K-wire or an AO screw (open or percutaneously). This method can also be used for condylar fractures and also selected cases of dorsal or volar fracture dislocation [1].
CONCLUSION
It is clear from the studies presented that the S-Quattro external fixator system is an effective and useful treatment option for the management of acute intra articular fractures of the phalanges. It may also be a treatment option for mal or non unions of such injuries following previous conservative or surgical attempts. However, further clinical evaluation is needed to consolidate its use for these fractures.
CONFLICT OF INTEREST
None declared.
ACKNOWLEDGEMENT
None declared.

