All published articles of this journal are available on ScienceDirect.

Computerized Tomographic Morphometric Analysis of the Cervical Spine
Authors Info & Affiliations
Abstract
Background:
Detailed knowledge of cervical canal and transverse foramens’ morphometry is critical for understanding the pathology of certain diseases and for proper preoperative planning. Lateral x-rays do not provide the necessary accuracy. A retrospective morphometric study of the cervical canal was performed at the authors’ institution to measure mean dimensions of sagittal canal diameter (SCD), right and left transverse foramens’ sagittal (SFD) and transverse (TFD) diameters and minimum distance between spinal canal and transverse foramens (dSC-TF) for each level of the cervical spine from C1-C7, using computerized tomographic scans, in 100 patients from the archives of the Emergency Room.
Results:
Significant differences for SCD were detected between C1 and the other levels of the cervical spine for both male and female patients. For the transverse foramen, significant differences in sagittal diameters were detected at C3, C4, C5 levels. For transverse diameters, significant differences at C3 and C4 levels. A significant difference of the distance between the transverse spinal foramen and the cervical canal was measured between left and right side at the level of C3. This difference was equally observed to male and female subjects.
Conclusion:
CT scan can replace older conventional radiography techniques by providing more accurate measurements on anatomical elements of the cervical spine that could facilitate diagnosis and preoperative planning, thus avoiding possible trauma to the vertebral arteries during tissue dissection and instrument application.
INTRODUCTION
Spinal stenosis is a major predisposing factor for cervical myelopathy and spinal cord injury and plays a decisive role on the outcome of injury patterns [1-5]. The size of the canal has been reported to function as a diagnostic tool on the development of myelopathy, in patients with degenerative stenosis [3, 6, 7].
In the past, several efforts have been conducted to accurately measure cervical spinal canal’s diameter, in patients with degenerative canal stenosis [7-10]. Nevertheless, plain x-ray measurements lacked compatibility due to differences in magnification [11]. Studies using computed tomography have also been performed on the vertebral bodies’ width, the lateral masses, the pedicles and the foramen of C2 nerve root [12-15]. Apart from the osseous structures, other anatomical elements of the cervical spine have been analyzed [16, 17].
We performed a CT analysis of the cervical spine to provide accurate measurements on sagittal canal diameter (SCD), right and left transverse foramens’ sagittal (SFD) and transverse (TFD) diameters and distance between spinal canal and transverse foramens (dSC-TF) for each level of the cervical spine, from C1-C7. These data could serve as useful tools for preoperative planning, regarding the surgical approach and screw orientation to the cervical spine.
MATERIALS AND METHODS
One hundred patients ≥ 18 years who had cervical spinal multiplanar computed tomography (CT) imaging performed for a variety of reasons were evaluated for this study. Patients were randomly chosen from the authors’ Emergency Room Radiology imaging data bank (level A Trauma Center). Subjects with evidence of infectious, neoplastic, traumatic, or congenital spine anomalies were excluded from the study.
The study group consisted of, 50 males and 50 females. Mean age was 46.73 years (range 20-79). Mean age for males was 48.78 years (range 20-77) and for females 46.59 years (range 26-79) Table 1. CT-scans were performed with the patient supine and the neck at a neutral position. For each level of the cervical spine, axial and sagittal images from C1 to C7 were selected and the following parameters were determined using the measuring tools of the Imaging software: (i) the sagittal canal diameter (SCD) (Fig. 1), (ii) the transverse foramens’ sagittal (SFD) and (iii) transverse (TFD) diameters and (iv) the distance between spinal canal and transverse foramen (dSC-TF) (Fig. 2). The sagittal canal diameters were measured at the midvertebral level where no degenerative changes are to be expected. The data were divided into two size-matched groups: males and females. Statistical analysis was performed using paired t-test.
Patients’ Characteristics (Age in Years, Weight in Kgrs and Height in Meters)
| Total | Males | Females | |
|---|---|---|---|
| Age(Range) | 46.73(20-79) | 48.78(20-77) | 46.59(26-79) |
| Weight(Range) | 71.1(55-88) | 81.06(75-88) | 61.13(55-67) |
| Height(Range) | 1.73(1.62-1.87) | 1.78(1.68-1.87) | 1.67(1.62-1.74) |
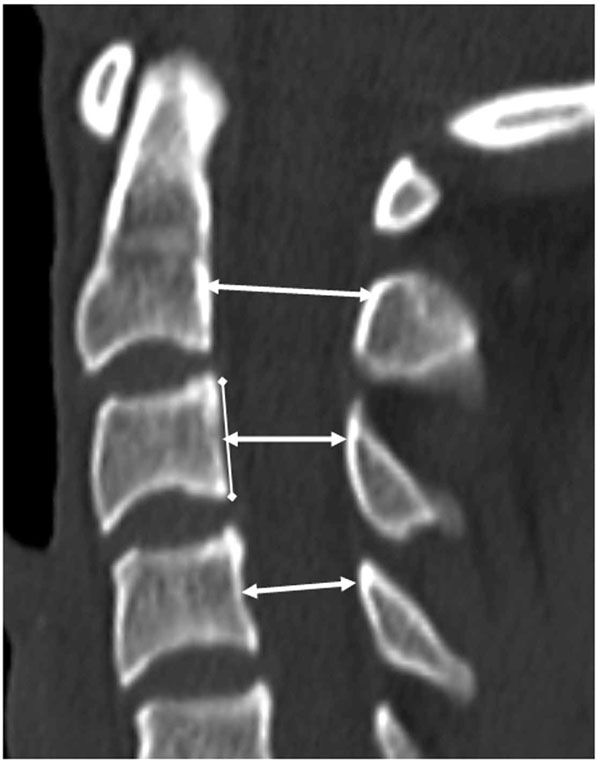
Sagittal canal diameters (SCD), at the midvertebral level, were measured on the mid-sagittal images from C1 to C7.
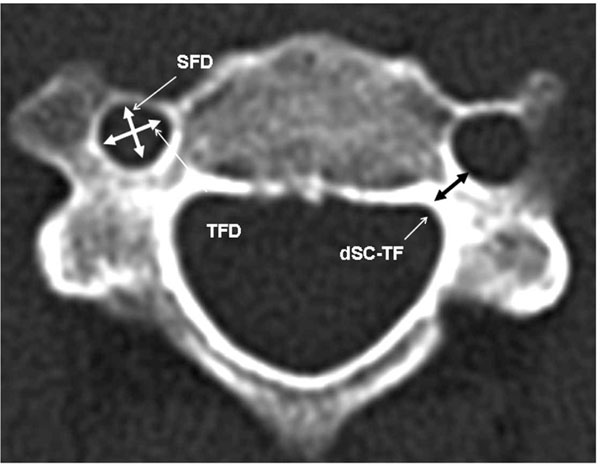
Transverse foramens sagittal (SFD) and transverse (TFD) diameters (left) as well as the distances of transverse foramens to the spinal canal (dSC-TF, right) were measured on the axial images from C1 to C7.
RESULTS
One hundred cervical spines comprising 700 vertebrae from C1 to C7 were evaluated. The means and standard deviations of the parameters were calculated at each level for male and female patients separately. Male and female SCD, SFD, TFD and dSC-TF values were compared.
Sagittal Canal Diameter (SCD)
For both groups, the widest sagittal canal diameter was measured at C1 and the narrowest at C4. Mean SCD was greater in males than in females (Table 2). However, only at the level of C6, a significant difference between male and female SCD was detected (p=0.005). Significant differences of SCD were also detected between C1 and the other levels of the cervical spine for both male and female patients, as well as between C2-C4 for males and C2-C4, C2-C6 and C3-C4 for females ((p<0.05).
Mean ± SD Values for Sagittal Spinal Canal Diameters (SCD). Mean Values were Greater for Males for All the Levels of CS. Only for C6 Level (Bold), a Significant Difference was Detected (p=0.005)
| Sagittal Diameters of Spinal Canal (mm) | ||
|---|---|---|
| Level | Males | Females |
| C1 | 16.61±1.92 | 16.28±1.57 |
| C2 | 13.59±1.62 | 13.25±1.27 |
| C3 | 13.31±1.71 | 12.94±1.32 |
| C4 | 13.05±1.01 | 12.49±1.49 |
| C5 | 13.43±1.22 | 12.66±1.68 |
| C6 | 13.28±1.85 | 12.52±1.76 |
Transverse Foramens’ Sagittal and Transverse Diameter (R/L SFD – R/L TFD)
The narrowest mean R-SFD was detected at C7 and the widest at C1, for both males and females. Similar results were obtained for the L-SFD values. On the contrary, the widest mean R-TFD values were measured at C7 and the narrowest at C1 for both males and females. Similar results were found for the L-TFD values (Table 3). Significant differences for L-SFDs between males and females were detected at C3, C4 and C5 levels (p<0.05). For male patients, significant differences for SFDs were detected between left and right foramen at the levels of C4, C5 and C6 and for females, at the levels C3, C4 and C5 (p<0.05). For TFDs, significant differences between males and females were detected at C3 and C4 levels (p<0.05). Similarly, significant differences were detected between left and right transverse foramen diameters at C3 and C4 levels for male and female patients (p<0.05).
Mean ± SD Values for Sagittal & Transverse Left and Right Transverse Foramens Diameters for Male & Female Subjects. Significant Differences (p<0.05) were Detected at C3, C4, C5 and C6 Levels of the Cervical Spine (Bold)
| Level | Transverse Foramen: Sagittal Diameters (SFD) (mm) | Transverse Foramen: Transverse Diameters (TFD) (mm) | ||||||
|---|---|---|---|---|---|---|---|---|
| Males | Females | Males | Females | |||||
| Left | Right | Left | Right | Left | Right | Left | Right | |
| C1 | 7.56±1.19 | 7.05±0.98 | 7.48±0.82 | 6.89±1.01 | 7.48±1.25 | 7.24±1.21 | 6.84±0.95 | 6.81±1.20 |
| C2 | 6.53±1.16 | 6.37±0.68 | 6.22±0.51 | 6.14±0.86 | 7.74±1.95 | 7.66±1.11 | 7.42±1.27 | 7.31±1.21 |
| C3 | 5.71±0.74 | 5.57±0.46 | 5.52±0.40 | 5.19±0.72 | 7.10±0.96 | 7.03±0.64 | 6.66±0.73 | 6.30±0.87 |
| C4 | 6.07±1.06 | 5.79±0.76 | 5.59±0.56 | 5.37±0.57 | 7.01±1.26 | 6.88±1.01 | 6.57±0.80 | 6.29±0.97 |
| C5 | 6.10±0.88 | 5.90±0.90 | 5.86±0.79 | 5.57±0.62 | 6.74±0.94 | 6.67±1.18 | 6.42±0.99 | 6.25±0.81 |
| C6 | 6.46±1.30 | 5.99±1.08 | 5.95±1.52 | 6.20±1.04 | 6.78±1.25 | 6.73±0.98 | 6.58±1.55 | 6.41±0.95 |
| C7 | 4.65±1.42 | 4.51±1.26 | 4.51±1.32 | 4.35±1.13 | 5.21±1.47 | 5.12±1.50 | 5.20±1.45 | 4.95±1.34 |
Distance Between Spinal Canal and Transverse Foramens (dSC-TF)
The narrowest mean right distance between Spinal Canal and Transverse Foramens (mean right-dSC-TF) was found at C5 and the widest at C1 for males and at C4 (narrowest space) and C1 (widest space) for females, respectively. Similar results were found for mean left-dSC-TF (Table 4). A significant difference was revealed for both male and female patients between left and right side at the level of C3 (p<0.05). Comparison between males and females demonstrated significant differences at C2, C3 and C4 levels on the left side of the cervical spine (p<0.05), while on the ride side, no significant difference was detected.
Mean ± SD Values for the Distance Between Spinal Canal and Transverse Foramens (dSC-TF). Significant Differences (p<0.05) were Detected at C2, C3, C4 Levels of the Cervical Spine (Bold)
| Level | Distances of Transverse Spinal Foramens from Cervical Canal (mm) | |||
|---|---|---|---|---|
| Right | Left | |||
| Male | Female | Male | Female | |
| C1 | 8.8091±1.50 | 8.325±1.02 | 8.619±1.49 | 8.175±1.062 |
| C2 | 4.571±1.32 | 4.037±0.99 | 4.529±1.32 | 3.750±1.00 |
| C3 | 4.761±0.94 | 4.250±1.00 | 4.428±1.12 | 3.875±0.88 |
| C4 | 4.523±0.92 | 4.00±1.15 | 4.420±1.07 | 3.687±0.94 |
| C5 | 4.429±1.07 | 4.062±0.99 | 4.340±1.11 | 4.00±1.154 |
| C6 | 4.429±1.12 | 4.307±1.21 | 4.428±1.03 | 4.30±1.095 |
| C7 | 5.904±1.48 | 5.687±1.25 | 5.523±1.43 | 5.437±0.81 |
DISCUSSION
Degenerative cervical spine diseases narrow spinal canal’s vital space, thus influencing proper function of neural elements at the level of the stenosis. The risk for the onset of neurological symptoms, even with low energy trauma, becomes greater in patients with progressed stenotic changes [9, 10, 18].
Several radiological techniques have been applied to measure canal’s sagittal diameter and detect a correlation with cervical myelopathy with the aim to establish a potent predicting factor [19, 20]. Application of Torg-Pavlov’s ratio on plain x-rays is a widespread, low cost technique [6, 10, 11]. Herzog et al, evaluating Torg-Pavlov ratio reported a high sensitivity but a poor positive predictive value [21]. On the other hand, CT-scan and MRI perform accurate measurements on the anatomical structures of the cervical spine, thus avoiding technical errors that could lead to false calculations. At our institution, all patients with head and cervical spine injuries receive a CCT (cranial computed tomography), according to the Canadian CT head rules for patients with minor head injury [22].
These results suggest gradual decline of spinal canal sagittal diameters, from C1 to C4. At the level of C5 the sagittal diameter increases and then declines again at the level of C6. The smallest sagittal diameter of the canal was detected at the level of C4. This was observed in both study groups (males, females). Similar findings have been reported by Song et al. in their study on spinal stenosis and neurological outcome in traumatic cervical spine injury [23]. However, when comparing these findings to other, more clinically related studies, one must be aware that in case of degenerative changes the smallest sagittal diameter is mostly determined by the presence of osteophytes and therefore not necessarily has to be at the level of the anatomically smallest diameter.
Comparison between mean values of the dimensions of the transverse spinal foramens revealed that sagittal and transverse foramens’ diameters are greater in males than in females, for each level of the cervical spine. Moreover at C1 level, sagittal diameter is greater than the transverse, while for all the other levels of cervical spine (C2-C7) the transverse diameter is greater than the sagittal. This phenomenon was equally detected in the two groups of the study (males, females). The measurements showed that the left spinal foramen was found to be greater than the right one. This difference was equally observed in male and female subjects and for each level of the cervical spine, implicating a larger left-sided vertebral artery and a possible asymmetric blood supply of these arteries. This hypothesis has also been proposed by Duan et al. on their work on vertebral artery course and function at the craniocervical junction [24]. This observation could serve as an important tool for all treating physicians and especially for those performing a surgical approach on the cervical spine since it could provide important data not only for the surgical approach (selection of the side, right or left), but also for the surgical technique (size and orientation of screws) to be applied.
Mean distance of spinal canal to transverse foramens was found to be greater for males than for females. A greater mean distance between spinal canal and transverse foramen was measured on the right side than on the left side. This is in accordance with our results, indicating that the left transverse foramen is bigger than the right one. For male subjects minimum mean dSC-TF was detected at the level of C5 while for female at the level of C4.
In conclusion, CT scan can provide accurate cervical canal measurements that could serve as a useful guide in the determination of the cervical canal stenosis, replacing the old lateral plain x-ray technique. Further studies are required to apply the Torg-Pavlov ratio on the more accurate cervical CT scans. Moreover, our measurements on the transverse foramen diameters may provide important informations to the spinal surgeons on the dimensions of the foramen and on its geometrical changes according to the cervical level, thus facilitating the preoperative planning and avoiding possible trauma to the vertebral arteries during tissue dissection and instrument application.
ACKNOWLEDGEMENT
Declared none.
CONFLICT OF INTEREST
Declared none.

