All published articles of this journal are available on ScienceDirect.

Lateral Clavicular Autograft for Repair of Reverse Hill-Sachs Defect
Abstract
Posterior dislocations of the shoulder joint can result in an impression fracture over the anteromedial humeral head, termed the reverse Hill-Sachs lesion, the presence of which can contribute to recurrent dislocations. Methods described to repair this defect include using allografts, iliac crest and coracoid process autografts, and bone graft substitutes. We describe a novel technique using the lateral end of the ipsilateral clavicle as an autograft in a 78 year old man with a reverse Hill Sachs lesion. This graft can be harvested through the same incision and does not compromise the stability of the acromioclavicular joint or any future shoulder arthroplasty.
INTRODUCTION
Dislocation of the shoulder joint can result in soft tissue or bony injuries which, if left untreated, can predispose to recurrent dislocations. Hill and Sachs described an impression fracture over the posterosuperior aspect of the humeral head in patients following anterior dislocations of the shoulder [1]. With arthroscopic examination this fracture has been reported to be present in up to 47% of patients after an initial anterior dislocation [2]. A similar bony impression fracture over the anteromedial humeral head, termed the reverse Hill- Sachs lesion, has been reported in up to 86% of patients following a first time posterior dislocation [3]. Open reduction and bone grafting of the defect is recommended if the size of the defect is 25- 50% of the humeral head [4]. Methods described to repair this bony defect include use of allograft (femoral head, humeral head, fresh frozen allograft) autograft (coracoid process and iliac crest) or bone graft substitutes [5-8]. We describe a novel technique where we used autograft from the lateral clavicle to fill the large defect over the anteromedial humeral head with a successful outcome.
CASE REPORT
A 78 year old man with a history of atrial fibrillation, significant weight loss, and hypertension sustained a posterior dislocation of his right shoulder following a fall whilst getting off a bus. He did not have a history of any previous injury or symptoms regarding his shoulders. Following unsuccessful attempts to reduce his shoulder under sedation in the accident and emergency department, he underwent a closed reduction under general anesthesia. The shoulder joint, on examination, was found to be unstable on internal rotation beyond 10 degrees. Two weeks following a closed reduction, he sustained a recurrence of dislocation whilst putting on his shirt. X-rays demonstrated the presence of a large reverse Hill Sachs defect (Fig. 1a, b). While performing a closed reduction under general anaesthesia with fluoroscopic screening, this defect was seen engaging the glenoid on internal rotation beyond 10 degrees. Screening was performed in all degrees of rotation, both in the reduced and unreduced positions to assess the maximum volume of this defect. A decision was taken to surgically repair the defect over the anteromedial humeral head without the need for further CT scans as fluoroscopic screening suggested the defect to be of sufficient size to contribute to a recurrent dislocation. Pre-operative x-rays and intraoperative screening confirmed an arthritic acromioclavicular joint. Excision of the lateral 1cm of the clavicle is a well described procedure in the management of acromioclavicular joint arthritis [9]. The size of the excised fragment was estimated to be of sufficient size to cover the reverse Hill Sachs defect as determined using fluoroscopy. An open reduction, bone grafting and shoulder stabilization was performed.
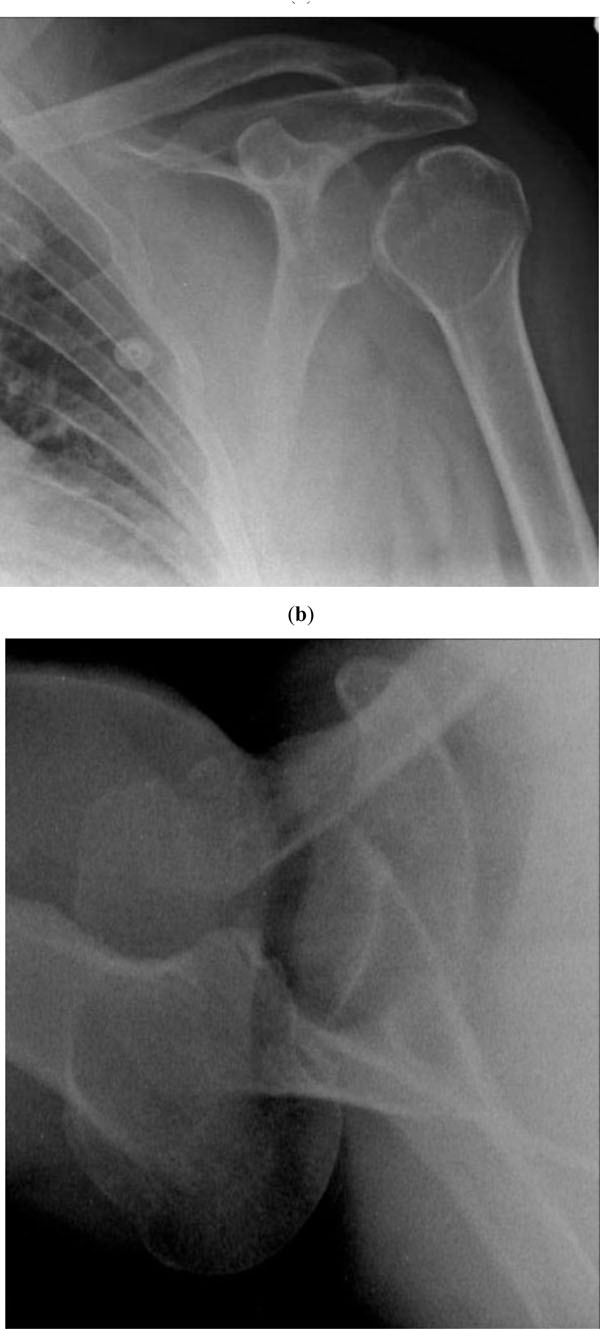
X- rays following posterior dislocation of the left shoulder AP view (a) and lateral view (b).
Surgical Technique
With the patient in a beach chair position, the shoulder joint was approached anteriorly through a standard deltopectoral approach. The subscapularis was divided in Z-lengthening pattern, and carefully dissected medial to the glenoid neck. A 3 cm X 4 cm defect was identified over the anteriomedial aspect of the head of humerus, caused by impingement of the posterior glenoid rim. The defect was debrided to reveal a bony bed and prepared for grafting. The antero-inferior aspect of the lateral clavicle was approached through the same incision, without the need for an extension or a separate incision. The curved shape and size of this section of the clavicle appeared well suited to fill the humeral head defect. A 1cm length of the lateral clavicle was excised, without disruption to the coracoclavicular ligaments and superior joint capsule. The acromioclavicular relationship under direct loading was confirmed to be maintained following excision of this fragment. The reverse Hill Sachs defect was filled with the correctly sized clavicle graft and fixed in place with a 4mm partially threaded cancellous screw and washer. The screw placement was determined to be anterior to the site of engagement of the defect and hence would not impinge upon the glenoid articular surface. Subscapularis was repaired with the shoulder maintained in 25 degrees of external rotation, to prevent over-tightening, with a No.5 non-absorbable Ethibond®. As the shoulder joint was found to be stable on internal rotation exploration of the rotator cuff was not performed. Other authors have described a very low incidence of rotator cuff injuries with posterior dislocation of shoulder [4, 10]. Following wound closure, with layered Vicryl®, the shoulder joint was braced in neutral rotation for 6 weeks.
At follow up, 2 months after surgery, the patient was able to actively externally rotate to 30 degrees, abduct to 90 degrees, and forward flex to 90 degrees. The shoulder and acromioclavicular joints were clinically and radiologically stable (Fig. 2a, b). At the final follow up 18 months following surgery, there were no reports of further dislocations. The patient had a clinically stable joint with a range of movements of 140 degree of forward flexion, 120 degrees of abduction and 60 degrees of external rotation. Internal rotation was restricted to L2 (up to T10 on the contralateral normal side).
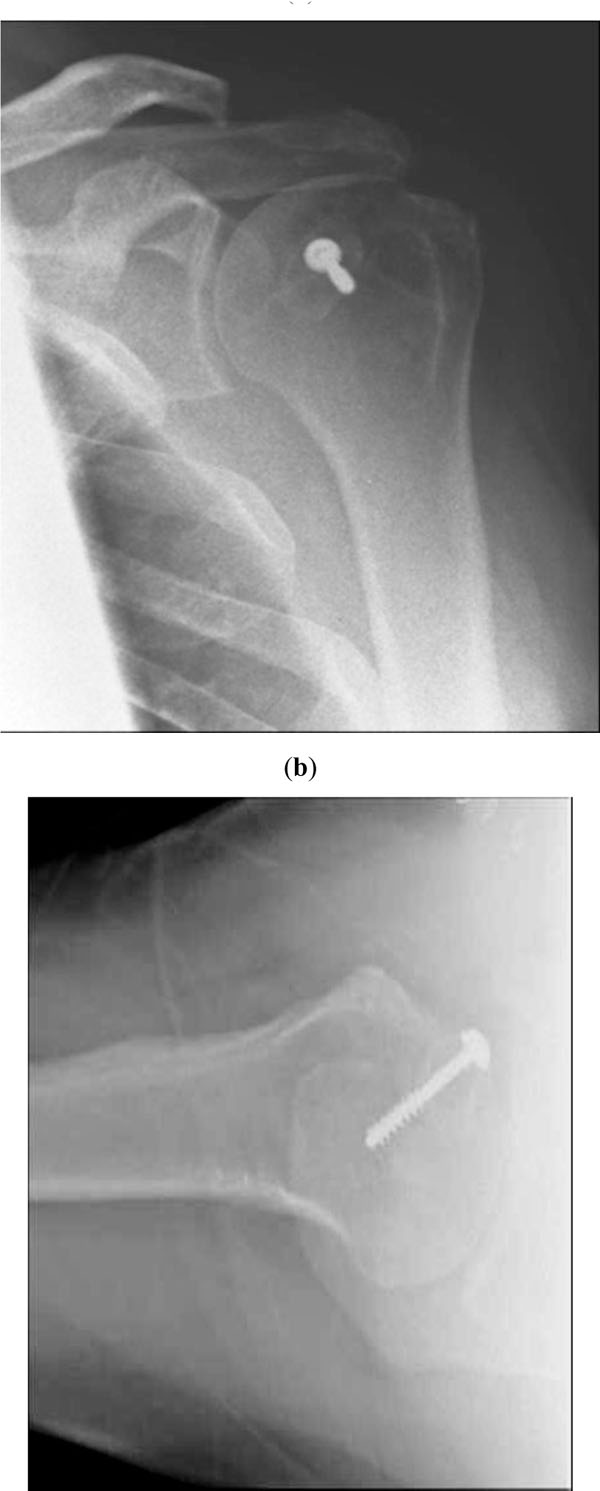
X- rays taken 2 months following reconstruction of the reverse Hill-Sachs lesion using the lateral end of the clavicle, AP view (a) and lateral view (b).
DISCUSSION
Based on the size of the defect, as a percentage of the humeral head diameter, reverse Hill Sachs lesions have been classified as small (25%), medium (25-50%) and large (>50% ) [4]. If left untreated, medium and large defects can predispose the patient to recurrent dislocations. Allograft reconstruction of these defects has the advantage of avoiding donor site morbidity seen in iliac crest autografts, but has risks of infection, potential for viral transmission, non-union, immune reactions and often needs additional resources to procure the graft material [11-13]. Good results have been described with transfer of lesser tuberosity into this defect using the Neer modification of the McLaughlin procedure [14].
We describe an alternative, previously undescribed source of bone graft which can be harvested from the same surgical field. Unlike the lesser tuberosity graft, this does not have a muscle attachment and hence has a lower chance of being disrupted by muscle contraction. Donor site morbidity, as following an addition incision for harvesting iliac crest graft is minimal. The lateral end of clavicle used is distal to attachment of the acromioclavicular ligament resulting in no risks of acromioclavicular joint dislocation. This, being fresh cortico-cancellous graft from the same patient, has the advantage of being safe with good healing potential. An additional benefit from this surgery would potentially be, in middle aged and elderly patients, in whom acromioclavicular joint arthritis is present, where this procedure would serve to remove subacromial impingement and lateral clavicle arthritic pain [9]. The technique also does not compromise any future arthroplasty procedures of the shoulder joint.
CONCLUSION
A novel technique of reconstruction of medium sized reverse Hill-Sachs lesion is described, utilizing an ipilateral host clavicle graft. Additional morbidity from this procedure is minimal and this does not compromise shoulder function, acromiocalvicular joint stability or future surgery around the shoulder.

