All published articles of this journal are available on ScienceDirect.

Monteggia Type IV Equivalent Injury
Abstract
Equivalent lesions of Monteggia type IV injury have not appeared so far in the literature. Two Monteggia type IV equivalent lesions, which included a fracture of the radial head associated with midshaft fractures of the radius and ulna in a 3- and in a 12-year-old girl, are reported. The lesion presented in this report could be considered as a missing piece in the puzzle of Monteggia and equivalent injuries, and it could also add towards considering type IV injury as a primary lesion and not as a variant of type I injury.
INTRODUCTION
Monteggia fracture-dislocation after its first description in 1814 was classified by Bado into four basic types and equivalent or Monteggia-like lesions [1]. His classification is also applicable in children [2-5]. Other classification schemes as well as fracture variations have also been described [6-8].
Two children with a Monteggia type IV equivalent lesion are presented and discussed. Review of the literature indicated that no equivalent lesions of the Monteggia type IV injury have been previously reported.
CASE REPORTS
Patient 1
A 3-year-old girl was admitted after a fall from a swing. She had a lateral angular deformity in the middle part of the forearm without any neurovascular abnormality. Radiographs showed displaced fractures of the middle thirds of the radius (plastic deformation) and ulna (greenstick) in association with a minimally displaced fracture of the radial head consistent with a Salter-Harris type II injury (Fig. 1a, b). The injury was considered to be a Monteggia type IV equivalent lesion, according to Bado’s classification. Anatomic reduction was achieved by closed means under general anesthesia and fluoroscopy. The arm was immobilized in an above the elbow plaster of Paris cast with the elbow in 90 degrees of flexion and neutral rotation. Radiographs showed an acceptable reduction one and two weeks after injury. Plaster was removed four weeks following injury. By that time, radiographs indicated complete healing of the fractures. Full flexion-extension and pronation-supination of the elbow was evident two months post-injury. Clinical examination of the patient 12 years post-injury revealed normal alignment of the forearm and a full range-of-motion in the elbow joint.
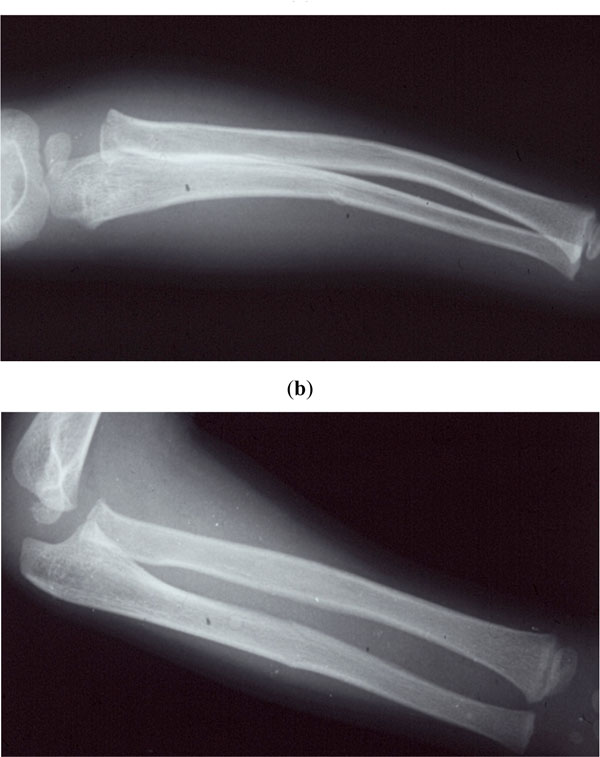
Anteroposterior (a) and lateral (b) radiographs of a 3-yearold girl at the time of injury showing fractures of the forearm bones with lateral angulation and a fractured radial head.
Patient 2
A 12-year-old girl injured her left arm after a severe fall from the high (horizontal) bar. Physical examination revealed a 2mm open wound on the ulnar aspect of her forearm caused by an angulated ulnar fracture. Radiographs of the left elbow, forearm and wrist revealed an oblique fracture of the ulna and a transverse fracture of the radius that were located in the middle third of the shaft and were displaced, as well as an undisplaced fracture of the radial head (Fig. 2a, b). The injury was considered to be a Monteggia type IV equivalent lesion according to Bado’s classification. The wound was irrigated and closed reduction was attempted under general anesthesia and fluoroscopy. The arm was immobilized in a long-arm cast with the elbow flexed 90 degrees and in neutral rotation. The patient was admitted for intravenous antibiotic therapy and elevation. Radiographs one and two weeks following injury showed an acceptable reduction (Fig. 2c). The plaster was removed six weeks post-injury and the patient was placed in a short-arm cast for two more weeks. By that time, radiographs indicated complete healing of the fractures. Four months after her injury, the patient had recovered full function in her arm with full and symmetric flexion-extension and rotation arc of the elbow. Fifteen years after the injury, the patient had normal alignment of the forearm and a full range-of-motion in the elbow joint.
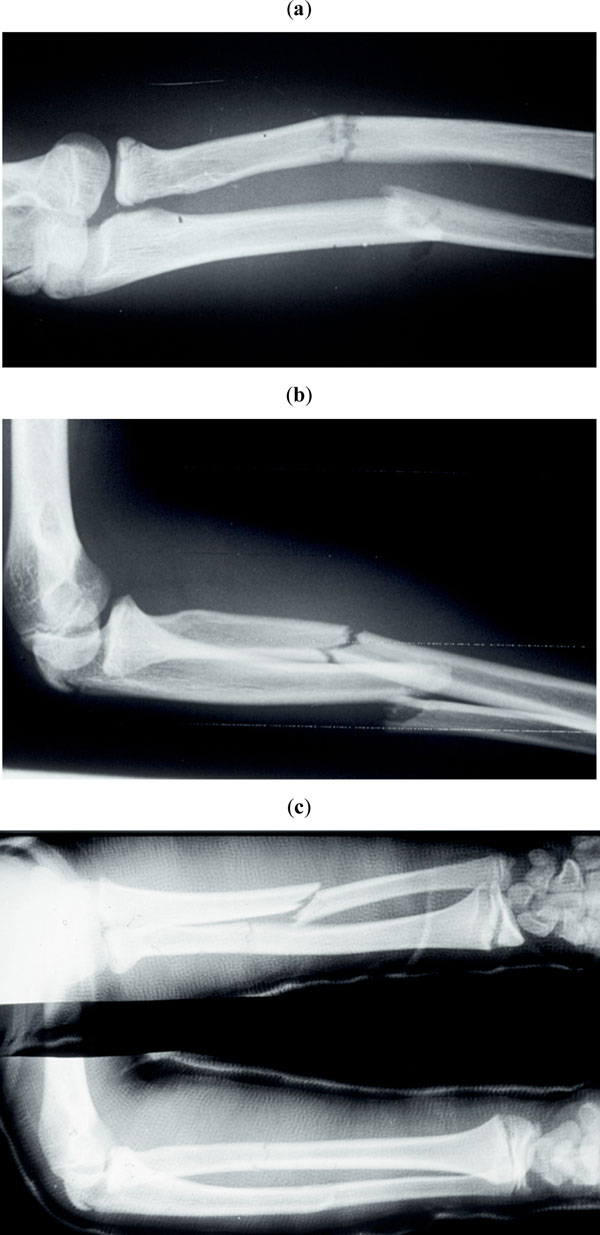
Anteroposterior (a) and lateral (b) radiographs of a 12-year-old girl at the time of presentation demonstrating concomitant fractures of the forearm bones and the radial head. Radiographs obtained 2 weeks after injury (c) confirming satisfactory alignment of the fractures.
DISCUSSION
Monteggia type IV lesion, as classified by Bado, is characterized by anterior dislocation of the radial head with a fracture of both forearm bones. It was formerly considered to be a rather infrequent lesion found exclusively in adults [1]. Few case reports referring to children have been found in world publications [9-12]. In addition, large reviews of the Monteggia lesion in children have indicated the rarity of type IV injury [8]. Olney and Menelaus [4] reported one type IV lesion out of 102 cases (frequency 1%), Wiley and Galey [3] 1 out of 46 (frequency 2%), Givon et al. [13] 1 out of 14 (frequency 7%), and Ring and Waters [5] 4 out of 36 (frequency 11%).
Other authors have considered Monteggia type IV injury to be a variant of type I injury and have excluded it from their classifications [3, 14].
Bhandari and Jindal [11] reported a type IV case with posterolateral dislocation of the radial head, so they suggested subgroups of Monteggia type IV injury. In Type IV-A lesion the fractures of the radius and ulna are associated with anterior dislocation of the radial head, in type IV-B with posterior dislocation, in type IV-C with lateral dislocation and in type IV-D there is a combination of types IV-A with IV-C or IV-B with IV-C.
Although type IV lesion is very uncommon in adults and even rarer in children, the radiocapitellar joint should be examined in all midshaft forearm fractures to avoid missing this injury complex [8]. Failure to recognize the radial head dislocation is the major complication of this lesion [15].
The level of the radial fracture is approximately the same or distal to the ulnar one [1, 8]. The type of the ulnar fracture has been estimated as incomplete (plastic deformation, greenstick and buckle) or complete (transverse, short or long oblique, and comminuted) [5].
Monteggia type IV lesions have been treated by both closed [4, 5, 13] and open techniques [1, 5, 9-11]. The degree of angulation or shortening of the forearm bones and late presentation of the patient were evaluated to estimate whether closed or open treatment modalities may be needed and to predict the final outcome [5]. The pattern of the offered treatment may depend on the ability to achieve a prompt, stable and anatomical reduction of the fractures and on the type of the ulnar fracture [5].
On the other hand, equivalent lesions of the Monteggia type IV injury have not been previously reported as case presentations, in large reviews [3] and major text-books [8].
Considering equivalent injuries to other types of Monteggia lesions, in which the dislocation of the radial head is replaced by a fracture of the radial head or neck, the association of the fractures of both forearm bones with a fracture of the radial head in our patients was considered to be a Monteggia type IV equivalent lesion.
The mechanism of injury in our patients was most likely a fall on an outstretched hand with some degree of pronation. The sequel of events from radial head injury to ulnar fracture and, finally, to radial fracture may be similar to that of a Monteggia type IV lesion [8]. The injury may be the result of severe high-energy trauma, it could be also due to a significantly longer period for energy absorption or to a combination of both. That could be the only explanation for the rarity of Monteggia type IV and equivalent lesions in both adults and children. Moreover, it seems reasonable to consider that, like type IV injury, equivalent lesions may also occur by any of the three proposed theories including hyperpronation, hyperextension and direct blow [1, 8, 10, 16].
In our younger case (patient 1), the fractures were incomplete with the radial (plastic deformation) located distal to the ulnar (greenstick) one. In the older case (patient 2), the fractures were complete with the radial located proximal to the ulnar one. They were both treated conservatively, since an acceptable reduction was achieved by closed means.
In both our patients, full range-of-motion of the elbow joint was soon restored, since there was no significant displacement of the fracture of the radial head.
Failure to diagnose a displaced fracture of the radial head is the major potential complication of the lesion.
CONCLUSION
Equivalent lesions of Monteggia type IV injury have not appeared so far in the literature. The lesion presented in this report could be considered as a missing piece in the puzzle of Monteggia and equivalent injuries, and it could also add towards considering type IV injury as a primary lesion and not as a variant of type I injury.
CONFLICT OF INTEREST STATEMENT
The author certifies that he has no commercial associations (such as consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article. The author received no financial support for this study.

