All published articles of this journal are available on ScienceDirect.

Audit of Orthopaedic Audits in an English Teaching Hospital: Are We Closing the Loop?
Abstract
Background:
Clinical audit is an important tool to improve patient care and outcomes in health service. A significant proportion of time and economic resources are spent on activities related to clinical audit. Completion of audit cycle is essential to confirm the improvements in healthcare delivery. We aimed this study to evaluate audits carried out within trauma and orthopaedic unit of a teaching hospital over the last 4 years, and establish the proportions which were re-audited as per recommendations.
Methods:
Data was collected from records of the clinical audit department. All orthopaedic audit projects from 2005 to 2009 were included in this study. The projects were divided in to local, regional and national audits. Data regarding audit lead clinicians, completion and presentation of projects, recommendations and re-audits was recorded.
Results:
Out of 61 audits commenced during last four years, 19.7% (12) were abandoned, 72.1% (44) were presented and 8.2 % (5) were still ongoing. The audit cycle was completed in only 29% (13) projects.
Conclusion:
Change of junior doctors every 4~6 months is related to fewer re-audits. Active involvement by supervising consultant, reallocation of the project after one trainee has finished, and full support of audit department may increase the ratio of completion of audit cycles, thereby improving the patient care.
INTRODUCTION
Delivery of high quality patient care is essential in modern NHS (National Health Service). Clinical audit is an important tool to improve and safeguard patient care. National Institute for Clinical Excellence (NICE) published principles for best practice in clinical audit [1] which defined clinical audit as “a quality improvement process that seeks to improve patient care and outcomes through systematic review of care against explicit criteria and the implementation of change. Aspects of structure, process, and outcomes of care are selected and systematically evaluated against explicit criteria. Where indicated, changes are implemented at an individual, team, or service level and further monitoringis used to confirm improvement in healthcare delivery”. A substantial sum of funding and time has been spent establishing audit practice in the NHS [2]. It has become a key component of clinical governance framework [3]. Recently there has been a move from “optional” clinical activity to more “obligatory” approach. All clinical staff is required to actively take part in clinical audit. Concerns have also been raised on loss of clinical time and money on auditing too many events without clear goals [2, 4].
A good clinical audit can provide objective evidence of improvement of quality of patient care and outcomes. This is only possible through completing audit cycle [1]. There are multiple studies showing substantial improvements through completion of audit cycle [5-7]. According to above mentioned definition, an audit project will be regarded as completed only after further monitoring (re-audit) has been performed following implementation of improvement. Therefore, 100% of the projects should complete an audit cycle. Without completion of an audit cycle, a sound evidence of quality improvement in health care can not be provided. However, there have been reports of poor proportion of completion of audit cycle across the NHS [8-10]. We aimed this study to analyse the last 4 years clinical audits performed in trauma and orthopaedic unit of local teaching hospital to evaluate the completion of audit cycle.
MATERIALS AND METHODOLOGY
This was a retrospective review of all clinical audits performed in trauma and orthopaedic department of local teaching hospital from Apr 2005 to Apr 2009. Data was collected from the records of clinical audit department. We divided these projects into local, regional and national. We analysed the overall audit proposals, projects abandoned, leading clinicians, audits completed and the ratio of re-audits. We also investigated into the reasons for premature abandoning of some of the audit projects and potential reasons for not completing the audit cycle.
In our hospital, like many others in the NHS, there is a dedicated clinical audit department which overlooks all the audit projects being performed in the hospital. It provides support for designing the data collection tools, collection of case notes and database design/analysis. We also have an audit facilitator in our department who is an orthopaedic consultant with special interests in audit and research. Every clinical audit project starts with defining a topic, based on clinical issues in delivery of high quality care to patients. The audit lead is responsible for literature search to define standard criteria, against which, the findings of the study will be compared. All of this is written on an official form which needs to be approved by the facilitator before submission to the audit department.
Fig. (1) presents the flow chart of the audit process in our hospital. The audit gets started only after approval from the audit department. After completion and presentation of audit findings in the departmental or hospital audit meeting, a feedback form is filled by the audit lead, explaining the implementation of recommended changes and plans for future re-audit to complete audit cycle. This is stored in the audit department data base for future reference. All of this process is time consuming but essential to monitor and streamline the audit activity in the hospital.
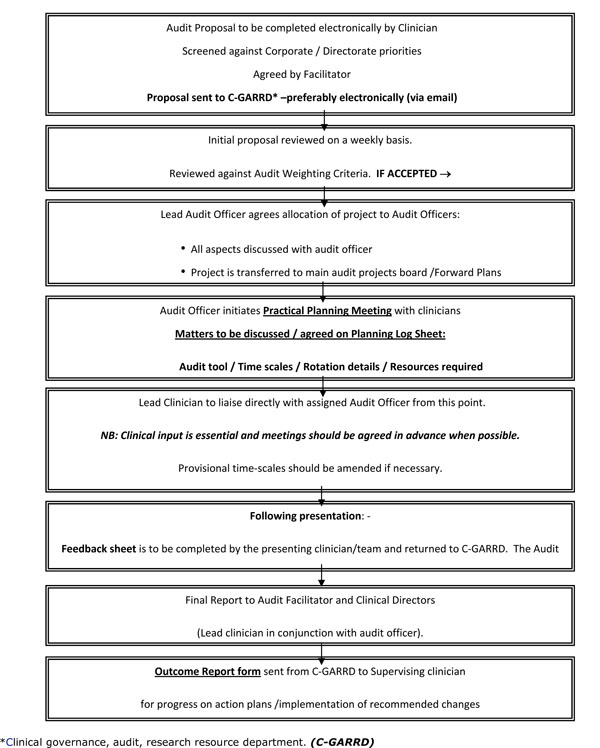
Process Flow Chart for Registration and Accessing Support of Audit Projects at our Hospital.
RESULTS
On the whole, 61 audits were commenced over the 4 years period. Most of these (59) were local, one project was part of the regional audit (Management of patients with Neck of Femur fractures in Trusts across the North West of England) and another audit was a part of national audit (National Comparative Audit of the use of Blood in patients undergoing Hip replacement). A consultant was either a leading clinician or was a supervising person in 59% (36) of the audits. SpR (Specialist Registrar) and staff grade surgeon each were the leaders of 16% projects. An SHO (Senior House Officer) alone was leading clinician in 7% (4) projects (Fig. 2).

The leading clinicians and audit projects.
Overall, a variety of topics were covered in these audit projects. Almost 20% projects were related to management of patients with hip fractures. This is consistent with practice in other trauma and orthopaedic units [9]. Other favourite topics were related to outcome after arthroplasty, infection and fracture management. Table 1 provides a summary of the areas covered and examples of important audit projects.
Summary of Audit Projects and Areas Covered (Total = 61 Audits)
| Audit Topics and Examples of Salient Projects | % (No.) |
|---|---|
Neck of Femur Fractures
|
19.7% (12) |
Outcome Following Surgical Procedures
|
13.1% (8) |
Audit of Infection
|
6.5% (4) |
Audit of Fracture Management
|
9.8% (6) |
| Audit of Record Keeping in Orthopaedics | 9.8% (6) |
Revision Hip Surgery Audit
|
4.9% (3) |
Audit of Incidence of DVT
|
3.2% (2) |
| Audit of the Requirement of Blood Transfusion After Primary Total Hip and Knee Arthroplasty | 6.5% (4) |
Other Audit Projects
|
26.2% (16) |
Out of 61 audit projects, 12 (19.7%) were abandoned, 44 (72.1%) were completed and presented in audit meetings and 5 (8.2%) audits were still ongoing. Only 13 (29%) projects had audit cycle completed by re-audits. Table 2 shows year by year audit performance in trauma and orthopaedic unit of local teaching hospital. Table 3 illustrates the reasons why some of the audits were abandoned.
Yearly Audit Performance
| Audit Year | 2005/06 | 2006/07 | 2007/08 | 2008/09 | Overall | % |
|---|---|---|---|---|---|---|
| Total audit proposals | 15 | 16 | 17 | 13 | 61 | 100% |
| Number abandoned | 4 | 4 | 3 | 1 | 12 | 19.7% |
| Number still live/ongoing | 5 | 5 | 8.2% | |||
| Number presented | 11 | 12 | 14 | 7 | 44 | 72.1% |
| Total Re-audits completed | 3 | 4 | 2 | 4 | 13 | 29.54% |
Audits Abandoned and Reasons
| Reasons for Abandoning | No of Audits |
|---|---|
| No Reason recorded | 7 |
| Clinician left trust | 2 |
| Unable to get sufficient sample size | 1 |
| Unable to identify relevant patients | 1 |
| Audit not started | 1 |
| Total | 12 |
DISCUSSION
Clinical audit has now become an essential part of clinical governance. A well conducted audit provides an objective way to review the quality of care, within a supportive and developmental approach. In trauma and orthopaedic unit of this teaching hospital, almost 15 audits were commenced every year over the last 4 years. Approximately 20% of the audits were abandoned due to either poor planning or the junior doctor, who was conducting the audit, moved to other hospital. Of the other 80% projects, 72% were completed and presented in the departmental meetings while 8% were still ongoing. This ratio of completion is much better than the other similar published studies [8, 10, 11]. Just completion of audit does not provide guarantee to improve the health care. It is the process of re-audit after implementation of change which ensures that standards of clinical care are continuously improved and maintained. Surprisingly, only 29% of the projects completed the audit cycle by process of re-audit. Gnanalingham et al. [8] and Guryel et al. [11] found even worse results in their studies. In their studies, 24% and 20% of the audits respectively, completed the audit cycle.
There have been concerns about audit being waste of money and time [4]. This could be true for those audit projects which are started without appropriate planning and either get abandoned or do not generate any action plan to improve the quality of care. Appropriate planning is therefore essential for any audit project. This involves carefully selecting a topic, relative literature search, definition of standard criteria, involvement of supervising consultant and signed undertaking by the audit lead to complete the project or handover to someone else in case they leave the department before completion of the audit.
Although audit is considered as an integral part of junior doctors training in NHS, issues of inadequate supervision and support have also been raised in some studies [12, 13]. Guryel et al. [11] found that if an audit was led by a named consultant or a nurse, there was a greater chance of audit cycle being completed. In our study, 61% of the projects were supervised by named consultant or a nurse. In spite of this, the percentage of re-audits has not changed significantly. Reallocation of the project to new trainee after one trainee has finished could lead to improve the ratio of audit cycle being completed. Active involvement of audit department and supervising consultants is very important in this regard. A system of reminder, e.g. an automatic email warning to the supervising consultant regarding re-audit dates may be helpful to improve re-audit ratios.
A uniform quality of care throughout the NHS is the aim of health department. National and regional audits could ensure that high standards of health care are being maintained across the country. However, we found that this particular trauma and orthopaedic unit has been part of only one regional and one national audit over the last 4 years. More resources and coordination between different hospitals is required for successfully conducting the regional and national audits. Table 4 presents some recommendations to improve the overall audit process.
Recommendations
|
In conclusion the overall percentage of completion of audit cycle is low. Good preparation, adequate resources, active involvement and supervision by the senior members of the staff and audit department are paramount to successful completion of the audit cycle which can ensure improvement in the quality of care.

