All published articles of this journal are available on ScienceDirect.

Radiation Exposure in The Treatment of Pediatric Supracondylar Humerus Fractures: Comparison of Two Fixation Methods
Authors Info & Affiliations
Abstract
Aim:
The study aims to determine the estimated radiation exposure of two different types of fixation (crossed vs lateral-entry K-wires) for displaced supracondylar fractures at a Major Trauma Centre in London.
Methods:
A retrospective review was performed between 2015 and 2019 in children (<16 years old) who underwent either Closed Reduction and Percutaneous Pinning (CRPP) or open reduction and K wire fixation for a displaced supracondylar fracture (Gartland II, III and IV) of the humerus.
Results:
The overall mean radiation dose and duration with crossed K-wire fixation was statistically lower when compared with two lateral K-wires. The mean radiation dose increased with increasing Gartland Grade - for Gartland Grades II, III and IV respectively.
Conclusion:
The current study showed statistically significant decreased radiation dose in crossed K-wire fixation method, compared to lateral-entry fixation. No difference was found regarding the cosmetic/functional outcome when Flynn’s criteria were applied.
1. INTRODUCTION
Supracondylar fractures are the most common elbow fractures in children, with the prevalence from 3% to 18% of all pediatric fractures [1, 2]. The vast majority of these injuries are treated with Closed Reduction and Percutaneous Pinning (CRPP). A variety of pinning configurations has been described, with crossed and lateral-entry K-wire configurations being the two most common.
In order to accurately reduce and stabilise a supracondylar fracture, the use of fluoroscopy is essential. One of the side effects is the exposure of both patient and surgeon to ionizing radiation. Calculating the radiation dose to a patient is complex (patient size, thickness of body/body composition in the plane of beam and energy of beam) [3]. Calculating the surgeon’s exposure is also challenging as exposure time to radiation, distance from the beam, quality/thickness of the shield and direct versus scatter type of radiation all influence the dose received [4]. Children have greater radiosensitivity than adults, and the mortality risk from cancer after radiation has been estimated at 5% per Sievert for adults and up to 9% for a 10-year old child, with the risk increasing for younger patients [5]. Minimizing radiation during paediatric orthopaedic procedures like supracondylar fixation is crucial.
This study aims to determine the estimated radiation exposure of two different types of fixation (crossed vs lateral-entry K-wires) for displaced supracondylar fractures at a Major Trauma Centre in London, UK, between 2015 and 2019.
2. METHODS
The study was registered with the Hospital Trust Clinical Audit and Effectiveness Group (Assigned number 9934). A retrospective review was performed of all paediatric trauma surgical theatre lists between January 2015 and September 2019 for children (<16 years old) who underwent either Closed Reduction and Percutaneous Pinning (CRPP) or open reduction and K wire fixation for a displaced supracondylar fracture of the humerus. The hospital's electronic health record system was searched for specific diagnoses, including the terms “supracondylar”, “humerus fracture”, “elbow fracture” or “medial/lateral condyle fracture”. All these additional terms were included to ensure that all supracondylar fractures were captured. Patients between one and 16 years of age with isolated displaced extension type supracondylar fractures (Gartland II, III and IV) were included in the study. Polytrauma patients, flexion type, revision of fixation, open fractures and patients with insufficient clinical or radiographic documentation were excluded. In order to achieve maximum homogeneity and strongest statistical results, we created two main groups, one with two crossed K-wires (M/L) fixation and the other with two lateral-entry K-wires (2L). Applying these criteria, a total of 185 patients were included in the study.
Emergency department documentation and pre-admission radiographs were used to establish patient demographics, mechanism of injury, laterality and grade of fracture (Gartland classification). The post-operative documentation and radiographs were used to evaluate the final clinical outcome using Flynn’s criteria (cosmetic and functional). The image intensifier was operated by a radiographer in all cases; Dose Area Product (DAP) of radiation exposure (measured in microGray per square meters (μGy.m2)) and radiation duration (in seconds) per case were recorded for all cases. The DAP was measured by an inbuilt DAP meter on the machine (Arcadis Varic image intensifier, Siemens©, Munich, Germany).
A pulsed method, one pulse per second, was used, with brightness and contrast being optimized automatically. A radiolucent table was used in all cases, and the C-arm was rotated to obtain different views of the elbow during the fixation. All operations were performed by a senior trainee (ST5+), a junior trainee (ST1-ST4) and a paediatric orthopaedic fellow or a paediatric orthopaedic consultant.
Statistical analysis of the results was performed using the Statistical Package for Social Sciences (SPSS), version 23.0 (IBM). Associations between independent variables and exposure outcomes were determined with Mann–Whitney tests or Kruskal–Wallis ANOVA. Significance for all tests was set at P <0.05.
3. RESUTLS
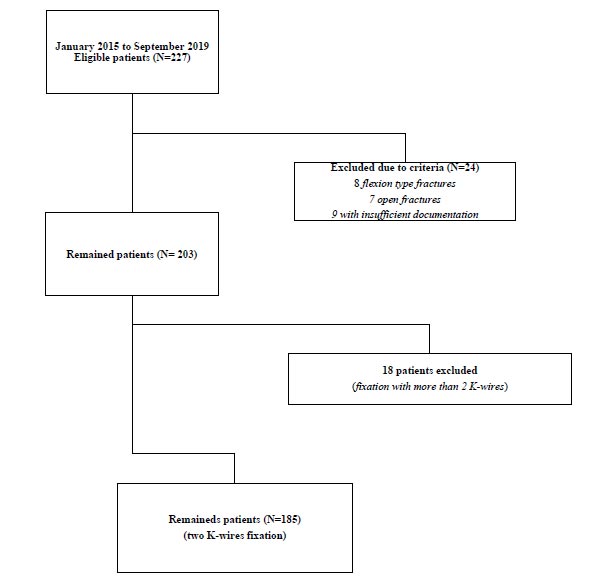
After applying the search criteria mentioned above, 227 patients were identified. 24 patients were excluded from analysis: 8 had flexion type fracture, 7 sustained an open fracture and 9 had insufficient clinical and/or radiographic documentation (Fig. 1). 18 patients were treated with more than two K-wires and they were excluded from the study. Patient demographics are presented in Table 1. The mean age of the 185 remaining patients, based on Gartland classification (Grade II, III or IV), was 5.41 (± 2.83 1SD), 5.25 (± 1.91 1SD) and 5.66 (± 1.83 1SD) years, respectively. No statistically significant differences were found regarding the age (p=0.579), gender (p=0.378), side (p=0.628), operation timing (p=0.397) and cosmetic/functional outcome applying Flynn’s criteria (p=0.032 and 0.021) between the three groups. 175 (95%) underwent CRPP, and only 10 (5%) had ORIF (Table 1). The type of fixation in every Gartland sub-group is presented in Table 1.
| Factor | Gartland II | Gartland III | Gartland IV | p-value (Between Groups) |
|---|---|---|---|---|
| Number of patients (n=185) | 54 ( 29.2%) | 98 (53%) | 33 (17.8%) | - |
| Age (years) | 5.41 ± 2.83 | 5.25 ± 1.91 | 5.66 ± 1.83 | 0.579 |
| Gender (M/F) | 25/29 | 40/58 | 18/15 | 0.378 |
| Side (L/R) | 29/25 | 46/52 | 18/15 | 0.628 |
| Operation timing | 0.61 ± 0.59 | 0.70 ± 0.61 | 0.55 ± 0.71 | 0.397 |
| Type of fixation (2L/ML) | 30/22 | 37/40 | 6/20 | 0.002 |
| ORIF (n=10) | 0 | 3 (0.16%) | 7 (3.8%) | - |
| Flynn’s Criteria Cosmetic Functional |
Excellent (95%) Excellent (94%) |
Excellent (93%) Excellent (90%) |
Excellent (89%) Excellent (88%) |
0.009 0.012 |
| Compared Groups | Radiation Dose in μGy.m2 | p-value | Radiation Duration in Sec | p-value |
|---|---|---|---|---|
| Crossed vs Lateral | - | 0.007 | - | 0.008 |
| Crossed k-wires (n=101) | 4.65 ± 2.79 | - | 32 ± 16 | - |
| Lateral k-wires (n=84) | 5.8 ± 3.07 | - | 38 ± 18 | - |
| Gartland II vs III vs IV Gartland II (n=54) Gartland III (n=98) Gartland IV (n=33) |
4.21 ± 2.53 5.32 ± 3.25 6.42 ± 2.24 |
0.003 | 28 ± 14 34 ± 17 41 ± 12 |
0.007 |
| Gartland II Crossed k-wires (n=23) Lateral k-wires (n=31) |
3.23 ± 2.33 4.87 ± 2.42 |
0.024 | 23 ± 13 33 ± 14 |
0.03 |
| Gartland III Crossed k-wires (n=53) Lateral k-wires (n=45) |
4.61 ± 3.07 6.15 ± 3.29 |
0.02 | 31 ± 15 39 ± 17 |
0.04 |
| Gartland IV Crossed k-wires (n=25) Lateral k-wires (n=8) |
5.94 ± 1.87 7.91 ± 2.74 |
0.09 | 37 ± 9 43 ± 15 |
0.12 |
| Study | Radiation Exposure (μGy.m2) |
|---|---|
| Current study | - |
| Gartland III (n=98) | 5.32 ± 3.25 |
| Gartland IV (n=33) | 6.42 ± 2.24 |
| Maempel et al. (2016) (n=54) | - |
| Gartland II | Median, 2.94; 25th percentile, 1.74; 75th percentile, 6.21; range, 0.67–17.23 |
| Gartland III | Median, 1.96; 25th percentile, 1.30; 75th percentile, 3.42; range, 0.47–8.88 |
| Li et al. (2019) | - |
| Gartland II & III (n=149) | 6.8 |
The overall mean radiation dose with crossed K-wire fixation (4.65 ± 2.79 μGy.m2) was statistically lower (p=0.007) when compared with two lateral K-wires (5.8 ± 3.07 μGy.m2). The mean radiation duration was 32 (±13 SD) seconds in crossed k-wires and 38 (±16) seconds in lateral-entry K-wire fixation (p=0.008). The mean radiation dose increased with increasing Gartland Grade - for Gartland Grades II, III and IV respectively, it was 4.21 ± 2.53, 5.32 ± 3.25 and 6.42 ± 2.24 μGy.m2 (p=0.003) (Table 2).
Comparison between the two types of fixation and Gartland Grades II and III, showed the mean radiation dose/duration was significantly lower with crossed k-wires compared to lateral-entry K-wires (Table 2). Reviewing fluoroscopy reports, it was noted in 60/84 (71%) of the lateral-entry fixation cases, the surgeon performed a live screening examination that increased the radiation exposure in these cases.
4. DISCUSSION
The current study showed a significant difference in radiation dose and duration for supracondylar fixation between two lateral-entry K-wires and crossed K-wire fixation. Crossed K-wires have shown a statistically significant decreased radiation dose. Our hypothesis that both types of fixation should have similar radiation dose was not confirmed by the results. However, the additional radiation dose may have been likely related to the dynamic rotational stability testing performed by surgeons employing the lateral-entry fixation technique. Expectedly, higher fracture severity was translated to a concomitant increase in radiation exposure/duration. To our knowledge, this is the first study comparing radiation dosage anger duration for these two different techniques in three different Gartland Classification Grades.
There have been few studies that have evaluated the radiation dose and duration during supracondylar fracture fixation. Schmucker et al. determined factors that influenced radiation exposure during fixation of supracondylar fractures [6]. No difference was found when they compared biplanar to uniplanar C-arm use, pre-operative compromise or comorbid ipsilateral fractures. Both radiation exposure and duration were increased as fracture displacement, and the number of pins was increased. This study did not classify the patients based on the fixation method as the current study did. Eismann et al. demonstrated how the C-arm position and the attending surgeon during supracondylar fixation, affect the radiation exposure to the surgeon. Fluoroscopy was significantly lower when the C-arm position was inverted when compared with the standard position (43 vs 26 seconds, p=0.034) [7]. Additionally, Esen et al. compared CRPP to ORIF for supracondylar fractures, and they found a significant increase in fluoroscopy time in patients who underwent ORIF [8]. In the current study, the number of the patients that underwent ORIF was too small for statistical analysis, however the mean radiation dose/duration was slightly increased (6.89 ± 2.45 μGy.m2) compared to the CRPP group (6.09 ± 2.65 μGy.m2). Maempel et al. tried to quantify radiation exposure in the operating theatre during paediatric upper limb fracture management. Only type-2 and type-3 (Gartland classification) supracondylar fractures were encountered, and they concluded that radiation exposure (in cGy.cm2) was higher in Gartland type-3 injuries (median values, 2.9 vs 1.96 cGy.cm2) [9]. Furthemore, Li et al. compared the radiation exposure during unstable supracondylar fixation using conventional C-arm (CCA) and mini-C-arm (MCA). The overall radiation exposure in the MCA group was much lesser compared to the CCA group (0.4 vs 6.8 mGy.cm2) [10]. Table 3 compares the amount of radiation, during supracondylar fixation that has been measured in different studies, including our study (all units have been converted to μGy.m2). Further statistical analysis between the studies was not possible due to heterogeneity.
An understanding of different radiation dose types is necessary when it comes to radiation exposure. The absorbed dose, measured in mGy, is the quantity of radiation energy an object absorbs per unit mass. The actual absorbed energy depends on the “object”, which in our case is the skin, soft tissue and bone. Any of these have their own weighting factor in order to make accurate measurements [11, 12].
Our study focuses only on the emitted radiation by the c-arm, which is the direct radiation exposure to the patient’s elbow. The surgeon’s radiation exposure is not being investigated and usually consists of two parts; the direct radiation that surgeon’s hands absorb and the scattered radiation, which is produced as photons that hit the object and scatter in different directions. Although it is crucial to focus on a surgeon’s radiation exposure, due to potential cumulative effects, rather than a one-time high dose experienced by patients, it is challenging to accurately measure it. Scatter radiation is often measured by dosimeters worn by surgeons. However, these devices do not measure the potential direct radiation and are very dependent on exactly where on the body they are being worn. Undoubtedly, the use of protective lead aprons is of paramount importance, as a 0.35mm lead gown can block 99% of the scattered radiation, and lead glasses can decrease the dose to the eyes by 10 times [13, 14].
CONCLUSION
Minimizing radiation exposure during supracondylar fixation is important not only for the patient but the surgeon too. This study demonstrates that the use of crossed k-wire configurations results in less radiation exposure compared to lateral k wire configurations. But this may be related to the additional dynamic screening to test rotational stability of the construct employed by surgeons using this fixation technique. In addition, both radiation dose and duration increased significantly as the Gartland Grade of the fracture increased.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
There is no funding source.
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

