All published articles of this journal are available on ScienceDirect.

Proposal of a New Reference Point to Determine the Tibial Resection Depth during Total Knee Arthroplasty for Valgus Knees
Authors Info & Affiliations
Abstract
The tibial resection depth during total knee arthroplasty for valgus knees has been variously described and not been standardized yet. Accordingly, it has been proposed in this article, that the sulcus between the medial and lateral intercondylar tibial tubercles can be used as a reference point for the tibial resection depth. The resection can be performed 8 to 9 mm distal to the sulcus.
1. INTRODUCTION
Valgus knee deformity is a challenge in total knee arthroplasty (TKA). It was reported that preoperative valgus deformity had a 2.1-fold higher risk for revision as compared to varus deformity after TKA [1]. In addition, there have been many controversies on surgical approaches, a tibial resection depth, soft-tissue handling, and component types [2-8]. Among many articles describing TKA surgical techniques for valgus knees, only a few have mentioned the tibial resection depth [2-6]. Aglietti et al. [2] removed 10 mm of bone from the medial tibial plateau. Chou et al. [3] reported that the tibial cut level was 9 mm distal to the most proximal part of the medial tibial plateau, assuming that the articular cartilage thickness was 1 mm. Ranawat et al. [4] and Rossi et al. [5] stated that the tibial resection level should be from 6 to 8 mm in the medial compartment. Koninckx et al. [6] performed the tibial cut 2 mm under the lowest lateral point. Surprisingly, the tibial resection depth has been variously described and not been standardized yet. On the other hand, a consensus on the tibial resection depth in varus knees has been reached, that is to say, the articular cartilage surface of the lateral tibial plateau is generally used as a reference point and the tibia is usually cut 9 to 10 mm distal to the cartilage surface. Accordingly, a new reference point has been proposed to determine the tibial resection depth during TKA for valgus knees.
1.1. Our Question About the Tibial Resection Depth During Total Knee Arthroplasty for Valgus Knees
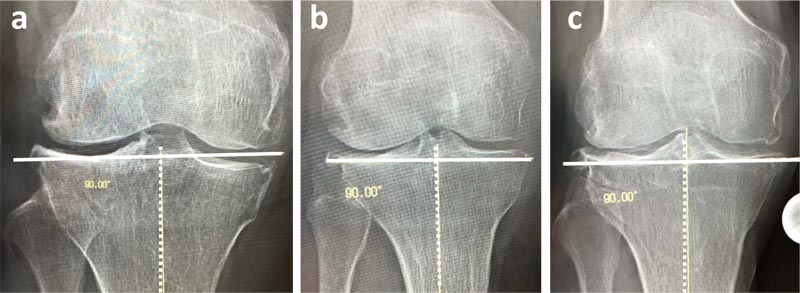
The articular surface of the medial or lateral tibial plateau has been used as a reference point for the tibial resection depth during TKA for valgus knees and the lateral tibial plateau is generally considered to locate more distally than the medial one in valgus knees [2-5]. Does the lateral tibial plateau locate more distally in all valgus knees? We examined weight-bearing anteroposterior lower extremity radiographs of 25 patients with valgus knees who underwent TKA during recent three years. A perpendicular line to the mechanical axis of the tibia was drawn at the level of the lowest portion of the lateral tibial plateau (Fig. 1a-c) to determine which plateau was located more distally. It was revealed that the medial tibial plateau was located more distally than the lateral one in six knees, the lateral tibial plateau was located more distally than the medial one in 12 knees, and both plateaus had equal height in seven knees. Thus, there were three variations in the height of the medial and lateral tibial plateaus. Therefore, it is apparent that uniformly determining the tibial resection depth in valgus knees by using articular surface of the medial or lateral tibial plateau as a reference point is not appropriate.
1.2. Our Hypotheses About the Tibial Resection Depth During Total Knee Arthroplasty for Valgus Knees
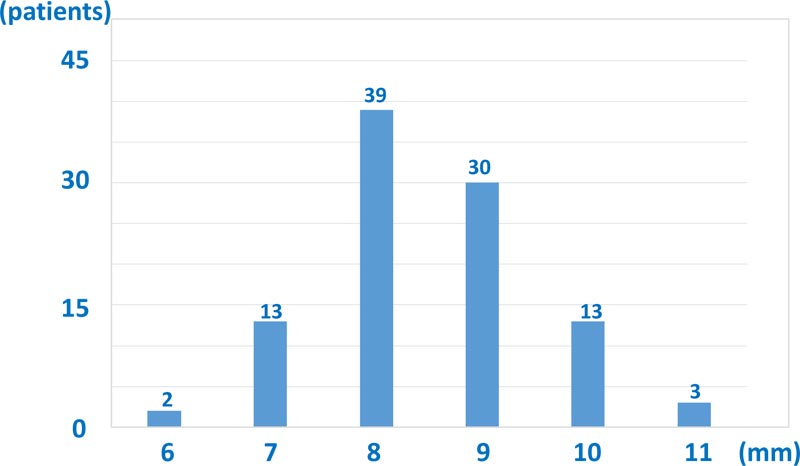
From our experience of many TKAs for varus osteoarthritic knees, in which the articular cartilage surface of the lateral tibial plateau is generally used as a reference point for the tibial resection depth and the tibia is usually cut 9 to 10 mm distal to the cartilage surface, we hypothesized that the sulcus between the medial and lateral intercondylar tibial tubercles could be used as another reference point for the tibial resection depth in varus osteoarthritic knees. During recently performed 100 TKAs for varus knee osteoarthritis, in which the tibia was cut 9 mm distal to the cartilage surface of the lateral tibial plateau, the thickness of the resected tibia was measured at the point of the sulcus (central thickness). As the sulcus is usually filled with soft tissue, it should be clearly exposed by excising the soft tissue using an electrocautery device and a curet. The average central thickness in 100 varus knees, which gained proper extension and flexion joint gaps and ligament balance during TKA, was 8.5 ± 1.0 mm (range 6–11 mm) (Fig. 2). Since the standard deviation of 1.0 mm was considered small, we thereafter utilized the average central thickness of 8.5 mm as an accessory reference during TKA for varus knees. The average height of these 100 patients was 152.8 ± 6.7 cm (range 134.8–168.0 cm).
We further hypothesized that the sulcus could be used as a reference point and the tibial resection depth could be set at 8 to 9 mm distal to the sulcus in valgus knees as well.
1.3. The Examination of our Hypothesis About the Tibial Resection Depth During Total Knee Arthroplasty for Valgus Knees
We prospectively examined our second hypothesis during 22 TKAs (out of 25 TKAs radiologically examined) for valgus knees performed from September 2017 to October 2020. Data of these 22 patients were summarized in Table (1). There were three male and 19 female patients and their average age at the time of operation was 68.7 years (range, 60–82 years). The average height was 156.7 ± 7.8 cm (range 146.2–175.0 cm). Variation in the height of the medial and lateral tibial plateaus in these 22 knees was as follows: the medial tibial plateau was located more distally than the lateral one in five knees, the lateral tibial plateau was located more distally than the medial one in 11 knees, and both plateaus had equal height in six knees.
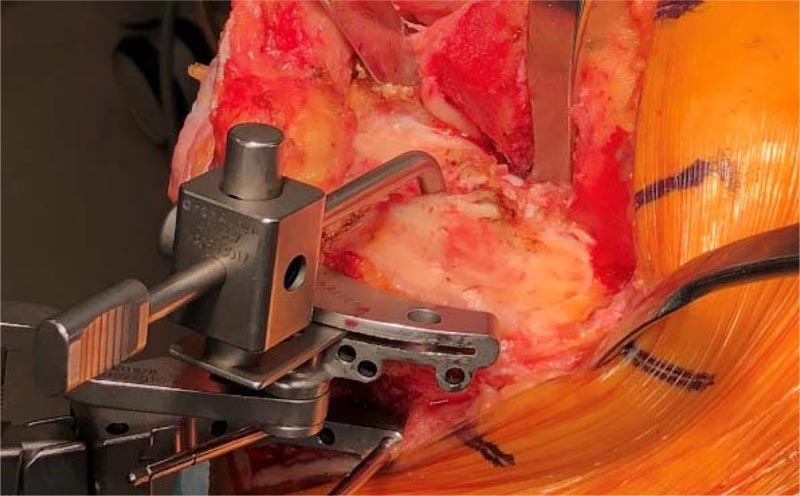
All TKAs were performed by the same surgical team. A midline longitudinal skin incision and a standard medial parapatellar arthrotomy were used. Both the distal femoral and proximal tibial cuts were performed perpendicular to the mechanical axes on the frontal plane, using an accelerometer-based computer navigation system: the KneeAlign2 system (OrthAlign Inc., Aliso Viejo, California, USA). At first, distal, anterior, and posterior femoral cuts were performed by usual manners. Next, the tibial resection depth was set at 8 to 9 mm distal to the sulcus using Persona tibial stylus (Fig. 3). The sulcus was clearly exposed by excising the soft tissue using an electrocautery device and a curet. Average thickness of the resected lateral and medial tibial plateau (lateral and medial thickness) was 2.9 ± 2.9 mm (range -2–9 mm) and 4.9 ± 2.1 mm (range 1–9 mm), respectively. Lateral thickness does not include cartilage thickness since the articular cartilage of the lateral tibial plateau is lost. Medial thickness includes cartilage thickness of the medial tibial plateau. After tibial bone resection, lateral soft tissue was released to a great extent, depending on the degree of lateral tightness, to gain proper extension and flexion joint gaps and ligament balance. Proper joint gaps and ligament balance were obtained without additional tibial resection in all TKAs examined. A posterior cruciate ligament-substituting and a constrained posterior cruciate ligament-substituting Persona prosthesis (Zimmer Biomet, Warsaw, Indiana, USA) were used in 11 and 11 TKAs, respectively. Thickness of bearing insert used was as follows: 10, 11, 12, 14, and 16 mm thick inserts were used in 14, 3, 3, 1, and 1 TKAs, respectively (Table 1). Thus, the use of a high level of constrained prosthesis and a thick bearing insert could be avoided in the presented 22 TKAs.
| Patient No | Age | Sex | Body height | Type of bearing insert used | Variation | Lateral thickness (mm) | Medial thickness (mm) |
| 1 | 68 | F | 156.8 | CPS | L | 1 | 6 |
| 2 | 77 | F | 155 | CPS | L | 0 | 6 |
| 3 | 69 | F | 157 | CPS | E | 2 | 1 |
| 4 | 78 | F | 150.6 | CPS | L | 2 | 5 |
| 5 | 60 | F | 168.5 | CPS | M | 9 | 2 |
| 6 | 63 | M | 167.7 | PS | L | 0 | 9 |
| 7 | 80 | F | 147.3 | PS | E | 0 | 2 |
| 8 | 69 | F | 153.7 | CPS | L | 2 | 6 |
| 9 | 64 | M | 175 | PS | E | 2 | 4 |
| 10 | 78 | F | 150.2 | PS | M | 5 | 2 |
| 11 | 65 | F | 150.2 | CPS | L | -2 | 6 |
| 12 | 60 | F | 160.5 | CPS | L | 1 | 6 |
| 13 | 68 | F | 156 | CPS | E | 3 | 5 |
| 14 | 69 | F | 146.2 | CPS | L | 5 | 8 |
| 15 | 82 | F | 155 | PS | M | 8 | 4 |
| 16 | 65 | F | 157.6 | CPS | L | 1 | 6 |
| 17 | 74 | F | 153 | PS | M | 7 | 5 |
| 18 | 61 | M | 169.5 | PS | E | 1 | 1 |
| 19 | 64 | F | 156.5 | PS | E | 5 | 6 |
| 20 | 66 | F | 148.6 | PS | L | 2 | 5 |
| 21 | 65 | F | 147 | PS | M | 8 | 5 |
| 22 | 67 | F | 164.7 | PS | L | 2 | 7 |
Variation, variation in the height of the medial and lateral tibial plateaus
L, the lateral tibial plateau is more distal; M, the medial tibial plateau is more distal; E, both plateaus have equal height
Lateral thickness and Medial thickness, thickness of the resected lateral and medial tibial plateau, respectively
1.4. Our Proposal of a New Reference Point to Determine the Tibial Resection Depth During Total Knee Arthroplasty for Valgus Knees
We clarified that there were three variations in the height of the medial and lateral tibial plateaus in valgus knees. Accordingly, the fact that the articular surface of the medial or lateral tibial plateau has been uniformly used as a reference point for the tibial resection; depth [2-6] should be considered inadequate and should be corrected. If the articular surface of the medial or lateral tibial plateau can be used as a reference point, the thickness of the resected medial or lateral tibial plateau must become constant. However, in all TKAs examined, proper joint gaps and ligament balance were obtained when the tibial resection was performed 8 to 9 mm distal to the sulcus, and the resected medial tibial plateau was thicker than lateral one in knees in which the lateral tibial plateau is more distally located, and vice versa (Table 1). Thus, the thickness of the resected medial or lateral tibial plateau was never constant. In addition, in knees in which the medial tibial plateau is more distally located Fig. (1a), if the tibial cut is performed 2 mm under the lowest lateral point [6], it will be impossible to cut the medial tibial plateau, and if the tibial resection level is set from 6 to 10 mm in the medial compartment [2-5], the lateral tibial plateau will be excessively removed.
CONCLUSION AND LIMITATIONS
In conclusion, we proposed that the sulcus between the medial and lateral intercondylar tibial tubercles can be used as a reference for the tibial resection depth and tibial resection can be performed 8 to 9 mm distal to the sulcus during TKA for valgus knees based on the current findings. We would like knee surgeons to try and assess our proposal.
There are two limitations in our proposal. First, the central thickness was measured during TKA for varus knees only in Japanese patients. Since the Asian population usually has a small body frame, the average thickness of 8.5 mm might not be applicable to other populations. Second, since the number of TKAs for valgus knees examined was small and follow-up period was short; therefore this proposal should be examined in many valgus knees by other knee surgeons.
ABBEREVIATION
| TKA | = Total Knee Arthroplasty |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This examination has been approved by the institutional review board of our clinic (approved number is 2019-001).
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all the participants.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial, or otherwise.
ACKNOWLEDGEMENTS
Declared none.

