All published articles of this journal are available on ScienceDirect.

Comparison of Interface Pressure, Contact Surface Area, and Percent Area of Coverage Between Two Suture Configurations for Hill-Sachs Remplissage
Authors Info & Affiliations
Abstract
Purpose:
To compare maximum contact pressure, contact surface area, and the percent area of coverage of the bone-tendon interface in the remplissage procedure between two different suture configurations (independent mattress versus double-pulley).
Methods:
A sample size of seven specimens per group was defined by a 96% power analysis.
Hill-Sachs lesions were created in all fourteen ex vivo ovine shoulders, corresponding to a 30% defect of the axial diameter of the humeral head (significant lesion according to literature). The defects were repaired using the remplissage technique applying one of the two randomly chosen suture configurations: two independent mattress sutures or a double-pulley. The contact pressure and contact surface area, as well as percent defect coverage, were recorded using a film sensitive to these parameters. Independent nonparametric tests (Mann-Whitney) were used for the statistical analysis.
Results:
The double-pulley group exhibited an average pressure of 0.128 ± 0.018 mPa, the contact surface of 0.199 ± 0.044 cm2, and 41.97 ± 9.8% defect coverage. The independent mattress group showed an average pressure of 0.102 ± 0.01 mPa, the contact surface of 0.081 ± 0.041 cm2, and defect coverage of 15.6 ± 8.1%. All three parameters were statistically superior in the double-pulley group (p=0.038, p=0.008, and p=0.008, respectively)
Conclusion:
The remplissage technique using the double-pulley configuration, presented superior biomechanical characteristics, in terms of contact pressure, contact area, and percent coverage of the defect, compared to the simple independent mattress configuration.
1. INTRODUCTION
Humeral bone defects (Hill-Sachs lesions) are associated with failed surgical treatment in glenohumeral instability [1-5]. Various techniques have been described for the management of these defects, including the remplissage procedure, which consists of “filling” the bony defect with the infraspinatus tendon [6]. Many different configurations have been proposed for this technique, however, they have rarely been compared in biomechanical or clinical studies. For this procedure to be successful, the tendon must heal on the bony bed of the Hill-Sachs lesion and thus prevent the engagement of the humeral head on the glenoid. Previous studies have shown that pressure at the bone-tendon interface as well as contact surface area are key factors for the healing process in rotator cuff tears [6-8]. However, to our knowledge, few studies have assessed this in a remplissage model. One recent article evaluated different suture configurations, but only assessed tendon coverage in a small number of cadavers [9].
The purpose of this study was to compare maximum contact pressure, contact surface area, and the percent area of coverage of the bone-tendon interface in the remplissage procedure between two different suture configurations (independent mattress versus double-pulley). Our hypothesis was that a double-pulley suture configuration would achieve superior biomechanical bone-tendon properties compared to an independent simple mattress suture configuration.
2. MATERIALS AND METHODS
2.1. Animal Model
Fourteen fresh frozen cadaveric sheep shoulders were used in this investigation. Cadaveric ovine shoulders have been previously validated for biomechanical studies by various authors [10-13].
After meticulous dissection, the infraspinatus tendon was identified; its humeral insertion in the greater tuberosity was maintained, and the remaining structures of the rotator cuff tendons (subscapular, teres minor), biceps, and neighboring tendons, in addition to the pericapsular ligaments, were resected carefully (Fig. 1).
2.2. Hill-Sachs Lesion Model
A significant Hill-Sachs lesion is defined as at least 30% of the articular surface [14, 15]. In our model, this percentage was estimated by measuring the total articular surface in the axial plane at the union of the superior third and inferior two-thirds of the humeral head. We, therefore, estimated a significant lesion as 10 mm (axial plane), 20 mm (cephalocaudal), and 3 mm (depth).
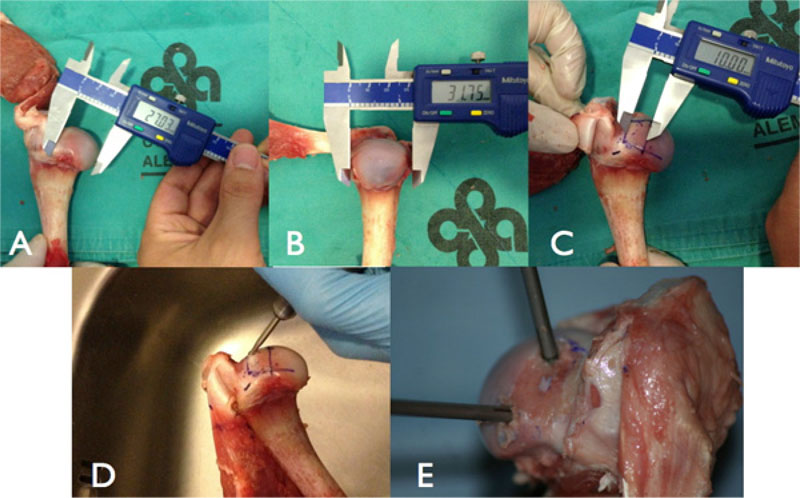
The calculated defect was created on the posterosuperior margin of the humeral head, 2 mm medial to the edge of the articular cartilage, with the aid of a digital caliper (Mitutoyo America, Aurora, IL, USA), a high-speed burr, and osteotomes (Fig. 2a, b, c, and d).
2.3. Remplissage Model
For all 14 models, two 5.5 mm anchors loaded with one N°2 FiberWire were used (Corkscrew FT: Arthrex Inc., Naples, FL, USA). Anchor placement was identical in both groups: one superior and one inferior, with ten mm between each anchor and equidistant to the edges of the previously created defect. (Fig. 2e). One of the following two suture configurations were randomly performed (seven per group):
2.3.1. Independent Simple Mattress Suture Model
The two limbs from the same anchor were tied in a mattress configuration using a Tennessee sliding knot and then blocked with a Revo knot for a total of two mattress stitches, one for each anchor.
2.3.2. Double-Pulley Suture Model
The lateral limbs of both anchors were tied to one another with a Revo non-sliding knot, and the medial limbs were then pulled taught compressing the previously tied knot against the tendon and into the defect. Finally, the medial limbs from each anchor were tied with a non-sliding knot [16].
2.4. Measurements
To evaluate the contact pressure, contact surface area, and percent coverage between the Hill-Sachs defect and the infraspinatus tendon, a pressure-sensitive film was used (Fujifilm Prescale Extreme Low Film) that consists of a sheet of micro granules that breaks as pressure is applied to it, which generates a permanent and high-resolution colored topographic map of the contact pressure and area.
A 20 x 10 mm rectangle of film, wrapped in cellophane to prevent alteration by liquids or moisture, was placed on the bone defect and tendon interface before tying the sutures. After the sutures were tied and then cut, the film was retrieved, the cellophane was carefully removed, and the film was sent out for analysis.
The films were analyzed using the Topaq computational system (Sensor Products Inc., Madison, NJ, USA), which uses the color inscriptions of the film to perform pressure and surface analysis.

The product manufacturer reports that the precision of this instrument is over 90%. The variables that were evaluated included the maximum contact pressure (mPa), contact surface area (cm2), and percent defect coverage (%) in each of the models. This instrument has been used in various similar studies, which have demonstrated its effectiveness [7, 8, 17].
2.5. Sample Size and Statistical Analysis
The sample size was determined with STATA ® v11.0, using a difference of 0.08 cm2, equal variances, statistical power of 96%, and a significance level of 0.05, data from a pilot study were used. The results indicated that seven cases per group were needed. Non-parametric Mann-Whitney tests were used for comparative analysis of the results, and a p-value of <0.05 was considered significant. Results are shown in mean, followed by the standard deviation.
3. RESULTS
The average maximum pressure obtained in the double-pulley group was 0.128 ± 0.018 mPa, which is significantly greater than that obtained in the simple mattress group (0.102 ± 0.01 mPa, p=0.038).
With respect to the contact surface, the double-pulley group exhibited an average of 0.199 ± 0.044 cm2, which was significantly higher than that in the independent simple mattress group (0.081 ± 0.041 cm2, p=0.008). The double-pulley group also exhibited a significantly higher percent coverage (41.97 ± 9.8%) than the independent simple mattress group (15.6 ± 8.1%, p= 0.008) (Fig. 3 a and b).

4. DISCUSSION
The results show that a double-pulley suture configuration is superior to a simple independent mattress configuration in terms of bone-tendon contact properties. It exhibited a significantly higher average maximum pressure, with a mean difference of 0.26 mPa. It also resulted in a greater contact surface area, with a mean difference of 0.12 cm2, exceeding the expected value of 0.08 cm2 considered significant in priori power analysis. In addition, the double-pulley configuration more than doubled the simple independent mattress configuration in percent defect coverage, reaching values of nearly 50%. These results show that the double-pulley configuration has far superior bone-tendon biomechanical characteristics. Further studies are needed in order to evaluate if the double-pulley technique improves healing and functional results.
Our cadaveric animal model has been validated in several previous studies [10-13]. Baums MH, in 2010, published a study using the same animal model and pressure film to evaluate different configurations of rotator cuff repair. They highlight the similar characteristics between sheep and human rotator cuff tendons [7].
Various alternatives have been previously described for the management of humeral bone defects or Hill-Sachs lesions, including bone graft or substitutes, the use of structural allografts, partial arthroplasty of the humeral head, and tenodesis of the infraspinatus (remplissage) [18-20]. The remplissage technique was first described by Purchase et al. [6], which consist of “filling” (the meaning of the French word remplissage) the defect with infraspinatus muscle, converting an intra-articular defect into an extra-articular one and, thus, preventing engaging and recurrence [18, 21].
The original remplissage technique has been modified by various authors regarding the location through which the sutures are passed, the number of anchors, and their location within the Hill-Sachs lesion. One such modification was described by Koo et al. [16] in which they extrapolated their double-pulley repair concept of the rotator cuff. Recently, a knotless variation was described as well [22]. This double-pulley configuration would theoretically improve tendon-bone interface biomechanics, and our study strongly suggests that it does.
In a recent study, Tan et al. compared the percent coverage between three different configurations: standard mattress, double-pulley, or Fibertape [9]. They found that the Fibertape configuration achieved the greatest coverage. Our area of coverage for the standard mattress technique was quite similar to Tan et al., 15.6% versus 13.36%, respectively. However, our study found a statistically higher coverage than theirs for the double-pulley technique, 41.97% versus 15.9%, respectively. One could suppose this far superior result is due to a difference in distance between anchors or anchor position. It should also be considered that we used a more sensitive pressure film (Fuji Film Extreme Low vs. Fuji Film Super Low), although results for the mattress configuration were quite similar. Their study did not evaluate interface pressure nor contact the surface area.
This biomechanical study has several limitations. As with any cadaveric research, results should be further assessed with clinical studies. Moreover, Effective contact pressure for adequate tendon bone healing has not been described in the current literature; thus, the clinical advantage obtained by the double-pulley model is only theoretical. Finally, mechanical stability to loading was not evaluated and compared between both configurations.
The strengths of this study consist of priori power analysis of 96% and the use of non-parametric tests, the use of a highly accurate instrument with over 90% accuracy, and the categorical nature of the obtained results. In addition, this is one of the few studies to evaluate the specified biomechanical variables in a Hill-Sachs lesion model.
CONCLUSION
In summary, the remplissage technique using the double-pulley configuration presented superior biomechanical characteristics, in terms of contact pressure, contact area, and percent coverage of the defect, compared to the simple independent mattress configuration.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
Authors have no conflicts of interest to declare. The authors and their immediate families, and any research foundations with which they are affiliated have not received any financial payments or other benefits from any commercial entity related to the subject of this article.
ACKNOWLEDGEMENTS
Declared none.

