All published articles of this journal are available on ScienceDirect.

Variations in Physiological and Psychological Responses of Orthopaedic Surgeons and Clinical Fellows during Hip and Knee Arthroplasties
Abstract
Background:
Both physical and mental stress is present within the practice of healthcare professionals, which in turn negatively affects the quality of the services provided to the population and therefore, leading to mental exhaustion of the individuals involved.
Purpose:
To track physiological and psychological responses to common hip and knee surgeries, and during clinic days, in a group of orthopaedic surgeons and their clinical fellows (trainees), and to compare the physiological and psychological results with baseline physiological stress tests.
Methods:
Heart Rate (HR), Breathing Rate (BR), and self-reported anxiety were recorded in 3 fellowship trained orthopaedic surgeons and 5 clinical fellows using a wearable Equivital EQO2 physiological monitor and the State-Trait Anxiety Inventory (STAI). Data was recorded for days in surgery as well as clinic for 6-8 hours/day. This data was compared to baseline physiological stress tests.
Results:
Mean HR and percentage of heart rate maximum (%HR-max) were not significantly different between staff and fellows throughout the surgery days regardless of the role occupied during both primary Total Hip Arthroplasty (THA) and Total Knee Arthroplasty (TKA). For Heart rate variability (HRV), there was no difference noted between staff and fellows at any moment around and during THA, however, fellows had significantly higher variability during TKA and maintained this increased variability in the postoperative period. In THA, staff failed to show any statistical difference between the HRV in the cases they were assuming the role of primary surgeon compared to the cases they were assisting and the clinic days. On the contrary, fellows showed significantly higher HRV when they were assisting during THA compared to when they were assuming the primary surgeon role or during their clinic days.
Conclusion:
Different stress patterns were noted in clinical fellows compared to the staff, especially showing a higher overall HRV during TKA.
1. INTRODUCTION
Physical and mental stress is present within the practice of healthcare professionals affecting negatively the quality of the services provided to the population [2-3] and leading to mental exhaustion of the individuals involved [17]. Medical training exposes the different level trainees to similar stressors leading to high incidence of stress and stress-related psychiatric conditions such as depression [8]. Although some of those factors have been identified [10-12-16] and attempts have been made to minimize them, this problem is still actively present [18]. This stressful environment can potentially affect negatively the ability to acquire new skills adequately [5].
It has always been difficult to quantify stress objectively. One of the methods that has been shown to be the most efficient to assess the activity of the autonomic nervous system and, therefore, quantify the effect of stress has been the evaluation of Heart Rate Variability (HRV) [13]. HRV has been demonstrated to be one of the best methods for autonomic stress assessment [13]. HRV can be calculated using frequency domain analysis of the beat-to-beat variation in Heart Rate (HR). Within the frequency domain analysis, the Low Frequency (LF) component is associated with sympathetic and vagal modulation of the heart while the High Frequency (HF) component is representative of vagal modulation of the heart. Consequently, the ratio of low to high frequencies (LF/HF ratio) is representative of the balance between sympathetic and vagal activity. A higher ratio represents a predominant sympathetic response, and therefore a period of higher stress while a lower ratio represents a predominantly parasympathetic response. Measuring HRV provides greater sensitivity than measuring HR alone, as an elevated HR alone may be due to physical exertion in the absence of other types of stresses (e.g. anxiety) [13]. This type of observation has been used in sports training in order to identify stressors and optimize the athlete’s training and overall performance [11, 19-24]. Few studies have been done in surgery [4-7]. Consequently, the aims of these study were 1) to track physiological and psychological responses to common hip and knee surgeries, and during clinic days, in a group of orthopaedic surgeons and their clinical fellows (trainees), and 2) to compare the physiological and psychological results with baseline physiological stress tests.
2. METHODS
2.1. Ethical Approval
Ethical approval was secured through the Western University Health Sciences Research.
2.2. Ethics Board
2.2.1. Inclusion/Exclusion Criteria
Adult hip and knee reconstruction specialized surgeons and the clinical fellows training in a single institution were included. Participants that had cardiovascular medical comorbidities such as cardiac arrhythmias, other cardiac or respiratory diseases requiring to take medications influencing cardiovascular parameters were excluded from the study. Other exclusion criteria included participants unable to wear the monitors and participants with BMIs lower than 18 or higher than 35.
2.2.2. Baseline Stress Testing
The participants underwent a baseline stress test at some point during the study depending on their time availability. The test was performed in a hospital setting under the supervision of an independent physician. The participants were asked to refrain from drinking caffeine on the day of the test. Once participants arrived at the hospital, they first completed a health check questionnaire. Their height and weight were then obtained using a stadiometer. Three initial baseline blood pressure measurements were recorded with a 2-minute interval between each reading prior to the start of the test in a sitting position. A 12-lead EKG was then placed on the participants and they started to exercise on the treadmill in an increasing difficulty fashion using the Bruce protocol (Appendix A). At each difficulty level, the participant was required to evaluate how they were feeling using the Borg scale as a reference (Appendix B). The treadmill part of the test was stopped at the moment the participant requested to stop. The reason for stopping was recorded in the participant’s chart. Maximum heart rate was recorded at that moment. The participant was seated at that point and serial EKG and blood pressure measurements were taken every 2 minutes for a total of 10 minutes post exercise. Maximum heart rate was calculated and used to calculate the percentage of maximal effort (%HRmax) reached during the different activities evaluated as a marker of intensity of the procedure.
2.2.3. Measure of Physiological Responses
The Equivital EQO2 HRV holter monitor (Vivonoetics, San Diego, California) was used for 6-8 hours on surgery workdays and on clinic workdays for the entirety of the respective workdays. We collected data including electrocardiogram (EKG) and respiratory rate (using strain gauge technology). An independent research assistant was responsible for collecting the data. The heart rate and breathing rate were stored on the device. The calculation of HR and HRV was performed using VivoSense® Software (Vivonoetics, San Diego, California). Determining the HRV was achieved by assessing the ratio of low-frequency of 0.04-0.15 Hz (LF) to high-frequency of 0.15-0.4Hz (HF) calculated power spectral density components of recorded tachograms (i.e. a graphical representation of the beat to beat differences in heart rate) [19].
2.2.4. Measure of Psychological Responses
To assess physiological responses, the participant completed the State-Trait Anxiety Questionnaire (STAI, Y1 and Y2) immediately prior to each surgery and after individual surgeries were completed. The STAI is a validated tool designed to quantify the subjective level of state (i.e. how anxious a subject is in the present situation) as well as trait (i.e. the tendency to perceive a given situation as stressful) anxiety. [20] It includes 40 questions (20 question for state and 20 questions for trait anxiety) that measure self-reported scales of feelings of apprehension, tension, nervousness, and worry. Higher scores on this measure signify higher levels of anxiety as a stable trait (STAI-Y1) or acutely (STAI-Y2).
2.2.5. Statistical Analyses
The data collected from staff and fellows from the monitoring included heart rate, respiratory rate and heart rate variability was compared using T-test to identify for differences in the mean levels recorded. Difference between the data recorded while performing different roles was analysed using one-way ANOVA. Post-hoc analysis was also performed. Pearson correlation coefficients (r) was used to compare the strength of association between the data collected from the questionnaire and the physiological responses noted with the monitoring. The absolute value for the strength of correlation (r) using the guide suggested by Evans 1996 were: < 0.20 “no correlation”, 0.20-0.39 “weak”, 0.40-0.59 “moderate”, 0.60-0.79 “strong”, 0.80-1.00 “very strong”. Analyses were performed using IBM SPSS Statistics software version 22.0 and a significance level of p≤0.05 was considered statistically significant.
3. RESULTS
A total of three joint reconstruction orthopaedic surgeons working in a single academic institution and five orthopaedic surgery clinical fellows training in the same institution from July 2015 to June 2016 were included in the study. No participants were excluded from the study. Data from the stress test was collected from all the participants. Data was collected for a total of 32 days, including 7 clinic days and 25 surgery days. Data was recorded from 11 Total Hip Arthroplasty (THA) and 20 Total Knee Arthroplasty (TKA) cases.
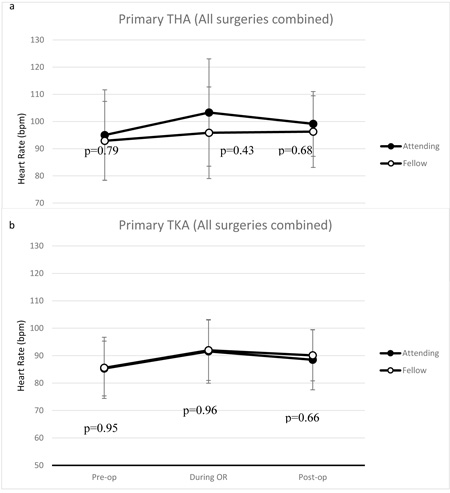
Mean Heart Rate (HR) and %HRmax were not significantly different between staff and fellows throughout the surgery days regardless of the role occupied during both primary THA and TKA (Fig. 1).
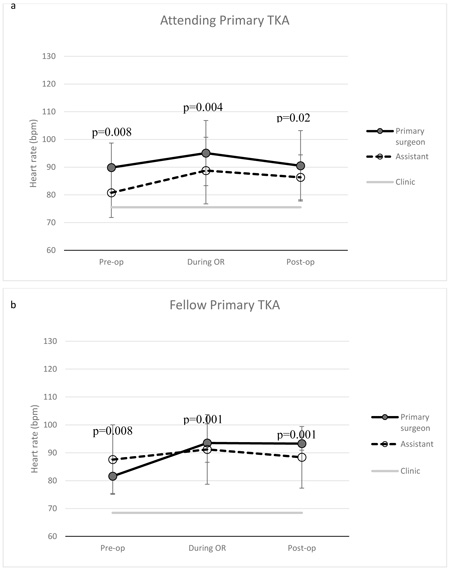
In a similar fashion, there was no significant difference between staff (mean 75 bpm, SD 6.0) and fellows (mean 68 bpm, SD 11.9) during clinic days (p=0.19). Analysis of the HR results by role assumed by surgeons and trainees during primary THA and primary TKA are indicated in Figs. (2 and 3), respectively.
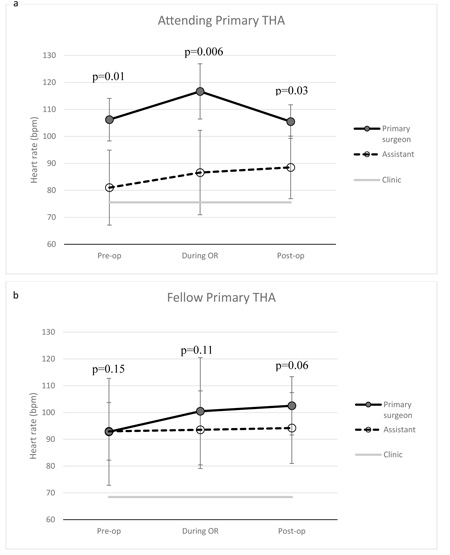
In THA, post-hoc analysis revealed that staff surgeons had significantly increased heart rates in the primary surgeon role compared to assistant role and clinic days. This was true when doing the analysis of the HR during the surgery but also in the preoperative and postoperative period. Moreover, staff tend to show a higher %HRmax while performing the surgery as primary surgeon (mean 77%, SD 17.3) compared to assisting (mean 56%, SD 15.4) and clinic days (mean 54%, SD 18.0) without statistical significance (p=0.08). In comparison, fellows involved in a THA case did not show significant difference between the assistant, the primary surgeon role and clinic days, with a tendency of increased heart rate during OR days compared to clinic days. Similarly, %HRmax was overall statistically similar between primary surgeon role (mean 74%, SD 26.6), assistant role (mean 69%, SD 20.1) and clinic days (mean 60%, SD 18.9). When analyzing the data obtained during TKA, staff also had significantly increased HR while performing those cases as primary surgeon compared to assisting to the surgery or during clinic days. Analysis of the %HRmax showed similar results with primary surgeon role (mean 73%, SD 23.6) presenting significantly higher intensity than during an assisting role (mean 49%, SD 4.8, p=0.006) and non-significantly higher than clinic days (mean 54%, SD 18.0, p=0.08). Post-hoc analysis showed tendency towards increased heart rate in the preoperative (p=0.09) and postoperative period (p=0.12) between the different roles assumed during TKA but no difference noted intraoperatively. On the other hand, post-hoc analysis of the data obtained from the fellows supported a difference between clinic days and OR days. However, when separating the data on the basis of the role that was assumed by the fellows during those cases, no difference was noted then. This was true for all time period including the preoperative, intraoperative and postoperative period. Similarly, no statistical difference (p=0.83) was noted in %HRmax between primary surgeon role (mean 63%, SD 3.8), assistant role (mean 59%, SD 16.8) and clinic days (mean 60%, SD 18.9).
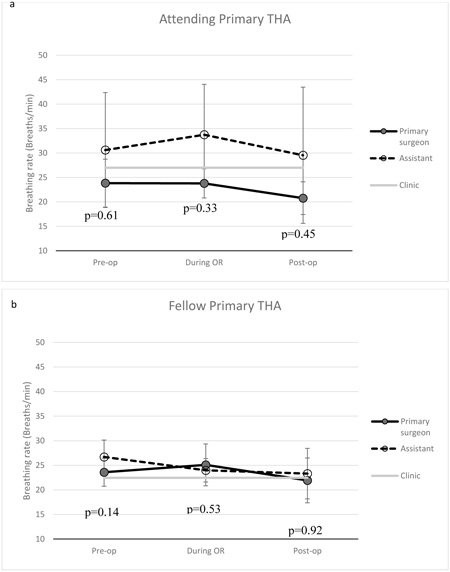
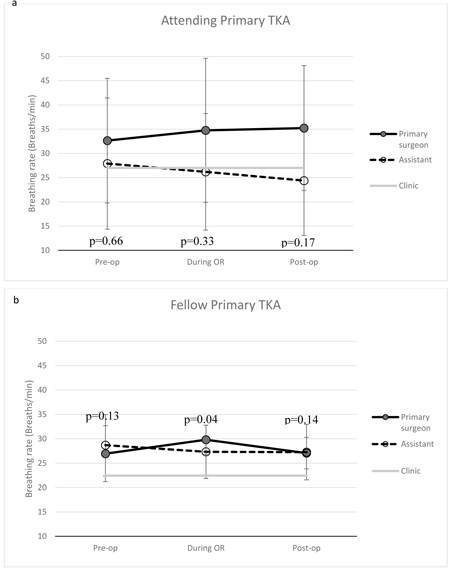
Respiratory rate results during THA and TKA are shown in Figs. (4 and 5) respectively. For THA, staff failed to show any significant difference in their breathing rate when comparing OR days and clinic days. Assuming a primary surgeon role did not show any significant difference compare to an assistant role or clinic days throughout the analyzed period. Fellows also did not show any significant difference between their respiratory rate during clinic days and OR days, even after analysis of the data based on the role assumed during those cases throughout the recorded period. For TKA, staff also failed to show any significant difference in their breathing rate when comparing OR days and clinic days. A role-based analysis also failed to show any difference between the assumed role during those type of cases. On the other hand, fellows showed significantly higher breathing rate in the primary surgeon role compare to clinic days only during the surgery itself. Post-hoc analysis showed that they had a tendency towards higher breathing rate when they were assisting a TKA case (p=0.12). The preoperative and postoperative periods around a TKA failed to show statistical significance in breathing rate compared to clinic days.
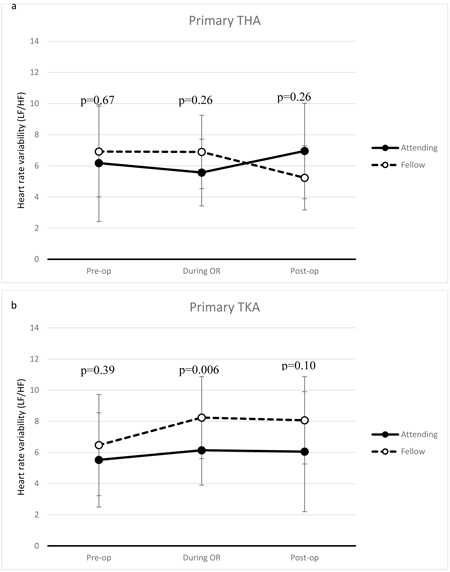
Heart Rate Variability (HRV) comparison between staff and fellows, independent of surgical roles, is shown in Fig. (6). Overall, there was no difference noted in the variability between staff and fellows at any moment around and during THA when combining all data collected. On the contrary, fellows had significantly higher variability during TKA and maintained this increased variability in the postoperative period.
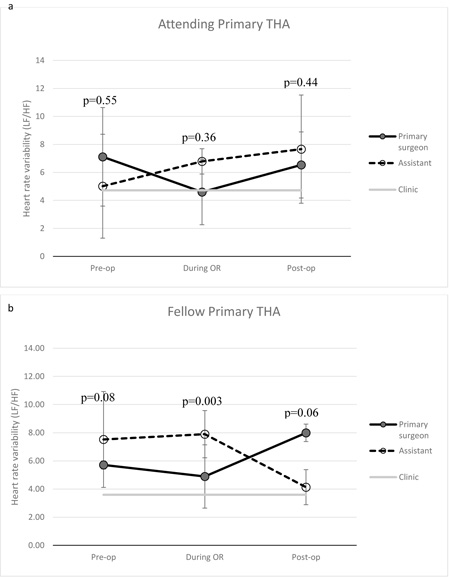
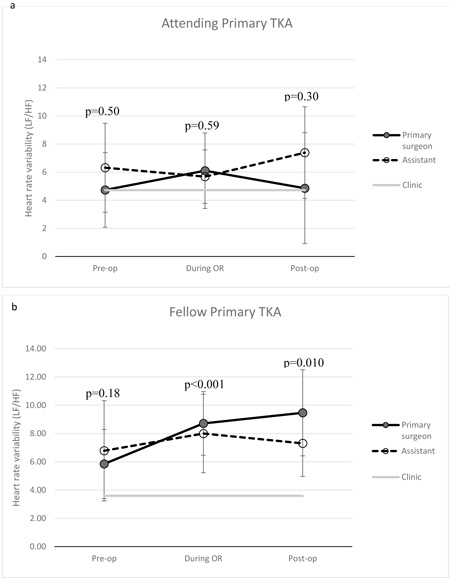
Analysis of the HRV results dependent on the role performed (surgeon or primary assistant) by staff and fellows during primary THA and primary TKA are shown in Figs. (7 and 8) respectively. In THA, staff failed to show any statistical difference between the HRV in the cases they were assuming the role of primary surgeon compared to the cases they were assisting and the clinic days. On the other hand, fellows showed significantly higher HRV when they were assisting during THA compared to when they were assuming the primary surgeon role or during their clinic days. In the preoperative period prior to THA, post-hoc analysis did not show increased variability in the assistant role compared to clinic day (p=0.07). No statistical difference was noted between the different roles assumed in the preoperative period. In TKA, staff also failed to show any statistical difference between the HRV throughout the data collection period regardless of the role assumed and the clinic days. Fellows showed no significant difference between the roles during TKA.
STAI questionnaires did not show any difference between staff and fellows in both the preoperative and postoperative period (Table 1). There was no correlation noted between the STAI scores and physiological responses like HRV (r = -0.14).
| Staff | Fellow | p-value | |
|---|---|---|---|
| Pre-op | 45.4 | 46.2 | 0.22 |
| Post-op | 45.7 | 45.3 | 0.58 |
| p-value | 0.60 | 0.15 | - |
4. DISCUSSION
The aim of this study was to track physiological and psychological responses to common hip and knee surgeries, as well as during clinic in a cohort of surgeons and their fellows. This study is the first to our knowledge involving common orthopaedic surgery procedures and physiological responses, since only questionnaire-based studies have been done in this field [9]. It is logical to state that some of the common orthopaedic surgical procedures are unique since they involve an added degree of physical effort compared to other surgeries such as general surgery. The physicality of these surgeries adds to the physiological responses experienced by the surgeon to the stressors surrounding the surgery itself. This makes it even more important to use HRV as our measurement tool to perform such analyses.
Physiological responses tended to be different between the staff and the fellows regardless of the procedures performed. Specifically, staff had overall a higher HR in the role of primary surgeon while the fellows showed no difference in HR regardless of the role assumed. Similarly, staff seemed to maintain no significant differences between their breathing rate in the OR compare to the clinic days while fellows showed a tendency towards increased respiratory rate during OR days compare to clinic days, especially during TKA where the difference reached statistical significance. Moreover, staff maintained a HRV similar between OR days and clinic days compared to fellows who showed higher variability during OR days compared to clinic days. Interestingly, fellows had higher variability while assisting in THA, while there was no difference noted between roles during TKA.
Multiple factors could potentially explain such results. First, the staff are more experienced in the type of cases that were performed in the study compared to the clinical fellows. Second, there might be a difference in the complexity of cases that each group had. Fellows might be assigned from their staff to perform more complex type of primary THA and TKA for an education purpose. Third, fellows have the extra task of learning the habits of each staff separately which might be accentuating the stress experienced by the fellows. Unfortunately, the data obtained do not permit the analysis of differences in physiological responses between early rotation cases and late rotation cases for the fellows. Future larger studies will help to further explore this issue.
Intensity noted during the cases for each role and during clinic days from staff and fellows were not different and followed similar patterns to HR changes, however this was different than what was observed with HRV. This accentuates the importance of the HRV analysis for our study since HR changes seemed more affected by the intensity of the procedure itself.
Data collected from the STAI questionnaire did not show any correlation with the physiological parameters that were collected. This questionnaire is a validated questionnaire that has previously been used to evaluate stress levels in surgeons. However, some of the results obtained from those questionnaires could be affected by the acute repetition of data with the high number of questionnaires that the participants had to fill during a single day. Moreover, some questions present in that form might be interpret by the participant in a way that would lead them to answer the question in a way that adds some bias in the collection of results (i.e. A surgeon would not feel comfortable to admit that he “feels indecisive” just before starting a procedure). Therefore, it might influence the results obtained.
There are some limitations to this study. First, noise in the EKG tracing collected might have interfered with the results obtained. We anticipate this effect would be small as the Vivosense software uses automatic filters to diminish the effect of the noise on the collected data as much as possible. Second, as mentioned above, STAI questionnaire results might be influenced by different factors making those results less interpretable. Third, the results might have been blunted by the fact that the trainees evaluated during this study were certified orthopaedic surgeons undergoing extra training for those common orthopaedic procedures. Fourth, the sample of staff and fellows were selected within a single institution, therefore limiting the number of participants and in the same way the statistical power of the study. Lastly, given the stress test was not performed at the beginning of the study but rather at any point during the period where data was collected. Nevertheless, since there was no planned exercise program for the participants in the study, there is very little change expected in maximal exercise capacity over a year as it has been previously shown in other studies and maximal heart rate is better predicted by age [11]. Therefore, timing of the baseline stress test is not expected to have any effect on our results.
Overall, this study represents a first step in the evaluation of physiological changes during common orthopaedic surgery procedures by both staff and fellows involved in those surgeries. Since we are able to show that these procedures can be more stressful for the trainees, this could be used as a basis to expand this type of analysis by evaluating the different steps involved in a procedure and evaluating specific events that could represent stressors for the trainees. The study could also expand to trainees with less experience including junior year residents. Implementation of the new models of surgical training which are competency-based, it will become increasingly important to improve the learning environment.
CONCLUSION
This study is the first study evaluating the physiological and psychological changes experienced by a cohort of orthopaedic surgeon and their trainees. Different stress patterns were noted in clinical fellows compared to the staff, especially showing a higher overall HRV during TKA. Further investigation to evaluate and identify specific steps intraoperatively which constitute stressors, identify their effect on learning and practice, and to provide interventions to optimize the environment for both the surgeon as well as other members of the health care provider team and trainees is required. Moreover, further investigation should expand to include orthopaedic surgery residents and medical students in addition to the clinical fellows.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was secured through the Western University Health Sciences Research.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Written informed consent for publication has been obtained.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.
APPENDIX
Appendix A
| Stage | Speed(km/h) | Speed(mph) | Gradient |
|---|---|---|---|
| 1 | 2.74 | 1.7 | 10 |
| 2 | 4.02 | 2.5 | 12 |
| 3 | 5.47 | 3.4 | 14 |
| 4 | 6.76 | 4.2 | 16 |
| 5 | 8.05 | 5.0 | 18 |
| 6 | 8.85 | 5.5 | 20 |
| 7 | 9.65 | 6.0 | 22 |
| 8 | 10.46 | 6.5 | 24 |
| 9 | 11.26 | 7.0 | 26 |
| 10 | 12.07 | 7.5 | 28 |
Bruce RA, Kusumi F, Hosmer D (1973). Maximal oxygen intake and nomo-graphic assessment of functional aerobic impairment in cardiovascular disease. Am Heart J, 85:546-582.
Appendix B
| Score | Exercise intensity | Intensity perception |
|---|---|---|
| 0 | None | |
| 0.5 | Very, very weak | (Just noticeable) |
| 1 | Very weak | |
| 2 | Weak | (Light) |
| 3 | Moderate | |
| 4 | Somewhat strong | |
| 5 | Strong | (Heavy) |
| 6 | ||
| 7 | Very strong | |
| 8 | ||
| 9 | Very, very strong | (Almost maximal) |
| 10 | Maximal |
Borg GA. Psychophysical bases of perceived exertion. Medicine and Science in Sports and Exercise. 1982; 14:377-381.

