All published articles of this journal are available on ScienceDirect.

Epidemiology of a Femur Shaft Fracture in an Acute Critical Care Center in a Rural Area of Japan
Authors Info & Affiliations
Abstract
Purpose:
Japan has the most rapidly aging population in the world. As of 2017, the number of people ≥65 years of age in Japan was 35.1 million, constituting 27.7% of the total population. The purpose of the study was to investigate the epidemiology in patients with a femur shaft fracture in a rural area with a super-aging population.
Methods:
Electronic medical charts from January 2011 to March 2019 were retrospectively reviewed for all patients with the main disease of ‘femur shaft fracture’ who had been transported to Numazu City Hospital. Subjects were divided into two groups based on the mechanism of injury: a Low-Energy (LE) group, which included patients who had been injured by falling down or suffered a fracture while walking; and a High-Energy (HE) group, which included patients who had been injured by traffic accidents or free fall from a high place (over 3 m). The variables were compared between the two groups.
Results:
During the investigation period, there were 58 patients with the femur shaft fracture, including 28 patients in the HE group and 30 in the LE group. The male ratio, injury severity score and ratio of open fracture in the HE group were significantly greater than in the LE group. The age and systolic blood pressure in the HE group were significantly lower than in the LE group.
Conclusion:
Among patients with femur shaft fracture in the acute critical care center in a rural area of Japan, where the population is super-aging, the frequency of HE and LE femur shaft fracture was almost the same. The fragility of the femur shaft in elderly people may explain this tendency.
1. INTRODUCTION
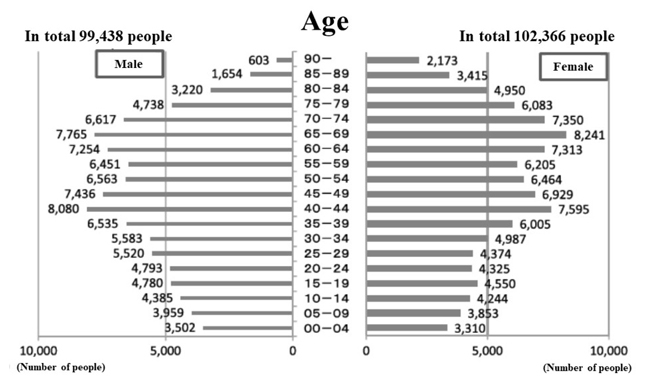
Shizuoka Prefecture is located near Tokyo and comprises 23 cities, 5 counties and 12 towns. The eastern region of Shizuoka Prefecture, including the Izu Peninsula and Mt. Fuji, is approximately 4,090 km2 in area, with a population of approximately 2 million. There are only two acute critical medical care centers in eastern Shizuoka Prefecture: Juntendo Shizuoka Hospital and Numazu City Hospital. Numazu City Hospital is a hospital with 426 beds and a medical emergency center in eastern Shizuoka Prefecture. A shortage of medical resources, including Emergency Room (ER) physicians, is a problem at Numazu City Hospital, so staff members from the Department of Acute Critical Care Medicine at Shizuoka Hospital of Juntendo University (Shizuoka, Japan) support this hospital [1]. In addition, the physician-staffed helicopter of Shizuoka Hospital of Juntendo University evacuates severely ill or traumatized patients based on information obtained at the first call to a fire department, such as a critical condition and/or a high-energy accident, even in Numazu City [2]. Accordingly, Numazu City Hospital mainly treats people living in Numazu City, the population of which is super-aging (Fig. 1). Numazu City has 7 hospitals with a department of orthopaedical surgery and 23 orthopaedical clinics. Among these seven hospitals, the Department of Orthopaedic Surgery at Numazu City Hospital has the highest activity for operation.
A femoral shaft fracture is a severe injury and is often associated with a high-impact trauma mechanism, being frequently seen in younger male patients with multiple injuries [3]. The management of femoral shaft fracture is therefore often directed by any additional injuries the patient has incurred [3]. However, for elderly patients, a hip fracture is much common than a femoral shaft fracture [4]. Recently, bisphosphonates have been reported as an atypical femur fracture in elderly people [5]. .
Japan has the most rapidly aging population in the world. As of 2017, the number of people ≥65 years of age was 35.1 million, constituting 27.7% of the total population and marking record highs in terms of both numbers and percentage [6]. https://www8.cao.go.jp/kourei/whitepaper/w-2018/html/zenbun/s1_1_1.html Aging induces osteoporosis, which is a brittle bone disease that can cause fractures and typically affects older men and women. We often experience cases of femur shaft fracture even in low-energy impacts, such as falls in the elderly.
In the present study, we conducted a retrospective investigation in order to determine the epidemiology of patients with the femur shaft fracture in a rural area with a super-aging population.
2. METHODS
The protocol of this retrospective study was approved by the review board of Numazu City Hospital and Juntendo Shizuoka Hospital on May 1st, 2019, and all examinations were conducted in accordance with the standards of good clinical practice and the Declaration of Helsinki. The corresponding protocol/approval number is [298].
Electronic medical charts from January 2011 to March 2019 were retrospectively reviewed for all patients with the main disease of ‘femur shaft fracture’ who had been transported to Numazu City Hospital, and these patients were included in the present study. Femoral shaft fracture was defined as a fracture of the middle portion of the femur, which extends from the lesser trochanter to the femoral condyle. We collected the data on each patient's sex, age, mechanism of injury, an open or closed fracture, vital signs on arrival (Glasgow Coma Scale, systolic blood pressure, heart rate), value of fibrin degradation product on arrival, fracture type based on fracture and dislocation classification compen- dium-2018 [7], surgical operation status, methods of operation, operation day, transfusion status, post-operative infection, duration of admission, final outcome (survival discharge or not), and non- or mal-union after discharge at Numazu City Hospital. The Department of Orthopedic Surgery at Numazu City Hospital did not measure the vitamin D level of admitted patients routinely. Patients were then divided into two groups based on the mechanism of injury: a Low-Energy (LE) group, which included patients who had been injured by falling down or spontaneously injured; and a High-Energy (HE) group, which included patients who had been injured by traffic accidents or free fall from a high place (over 3 m). The variables mentioned above were compared between the two groups.
Statistical analyses were performed using a non-paired Student’s t-test, a chi-square test, and a contingency table analysis as appropriate. A P value less than 0.05 was considered to indicate a statistically significant difference. All of the data are presented as the mean ± standard deviation or median with quartile.
3. RESULTS
During the investigation period, there were 58 patients with the femur shaft fracture, including 28 patients in the HE group and 30 in the LE group. There was one patient who spontaneously pathologically fractured their femur shaft due to post-osteomyelitis while walking. This patient was classified into the LE group.
The results of the analysis of the two groups are shown in Table 1. There were no significant differences concerning Glasgow Coma Scale, heart rate, value of fibrin degradation product, type of a fracture, ratio of surgical operation, transfusion, post-operative infection, duration of admission, or final outcome between the two groups. However, the male ratio, injury severity score and ratio of open fracture in the HE group were significantly greater than in the LE group. The age and systolic blood pressure in the HE group were significantly lower than in the LE group. Concerning the operation method, antegrade intramedullary nailing in the HE group and plating in the LE group were predominant.
Non- or mal-union could not be evaluated as most patients were lost to follow-up after being transferred to rehabilitation or nursing facilities.
4. DISCUSSION
This is the first study to demonstrate that, among patients with a femur shaft fracture in the acute critical care center in a rural area of Japan, where the population is super-aging, the frequency of HE and LE femur shaft fracture was almost the same. In addition, patients with the femur shaft fracture induced by HE accidents tended to be younger and more severely traumatized than those involved in LE accidents. However, the final outcome, including the duration of hospitalization and survival ratio, did not differ significantly between the groups.
Femoral shaft fracture in elderly patients is thought to be relatively uncommon, with hip fractures being more common in this population. Femoral shaft fracture in elderly patients may thus have a special etiology (e.g. bisphosphonates inducing atypical femur fracture [5]). However, according to our medical chart review, none of our patients had atypical femur fracture induced by bisphosphonates.
A previous report revealed that femoral shaft fracture could occur in elderly patients because such patients tended to have osteoporosis [3, 8]. The present study also found that patients with the femur shaft fracture induced by LE accidents tended to be older than those injured in HE accidents. Elderly people have a wide variety of medical problems and need multi- disciplinary care in order to be discharged from the hospital [9, 10]. The management of the femoral shaft fractures in the elderly is therefore often directed by co-morbidities and the patient’s medical condition. Such issues may thus induce a delayed discharge even if the injury was only an isolated femur shaft fracture. Because of the crisis of health care costs facing aging societies and falls in the elderly being a major source of injury, resulting in disability and hospitalization, fall preven- tion measures should be strengthened based on risk factors, such as sarcopenia/frailty, polypharmacy, multimorbidity, vitamin D status and home hazards [11]. Unfortunately, there are no standard prevention programs for falls in Japan, and each hospital is left to attempt to draft guidelines for prevention.
| - | High Energy N=28 |
Low Energy N=28 |
P Value |
|---|---|---|---|
| Sex (male/female) | 20/8 | 7/23 | <0.001 |
| Age (years) | 41.8 ± 18.2 | 76.5 ± 19.4 | <0.001 |
| Close (yes/no) | 21/7 | 28/2 | <0.05 |
| Injury severity score | 11.8 ± 3.7 | 10.1 ± 0.7 | <0.05 |
| Glasgow Coma Scale | 15 (15,15) | 15 (15,15) | n.s. |
| Systolic blood pressure (mmHg) | 125.0 ± 20.9 | 146.0 ± 29.2 | <0.01 |
| Heart rate (beats per minute) | 84.4 ± 13.3 | 81.6 ± 12.6 | n.s. |
| Fibrin degradation product(mg/L) | 26.9 ± 24.0 | 24.3 ± 33.9 | n.s. |
| Type of fracture 32A | 14 | 18 | n.s. |
| 32B | 11 | 9 | - |
| 32C | 3 | 3 | - |
| Operation (yes/no) | 28/0 | 28/2 | n.s. |
| Operation day | 3.6 + 2.2 | 4.1 + 3.1 | n.s. |
| Operation method | - | - | <0.05 |
| Antegrade intramedullary nailing | 18 | 9 | - |
| Retrograde intramedullary nailing | 4 | 4 | - |
| Plating | 4 | 13 | - |
| Others | 0 | 2 | - |
| Transfusion (yes/no) | 7/21 | 12/18 | n.s. |
| Infection (yes/no) | 0/28 | 1/29 | n.s. |
| Duration of admission (day) | 29.5 ± 22.0 | 31.5 ± 27.5 | n.s. |
| Survival ratio (%) | 100 | 100 | n.s. |
In the present study, patients stayed in the hospital for 29.5 days in the HE group and 31.5 days in the LE group, which may be a relatively long duration [12]. However, the average operation day was 3.6 days in the HE group and 4.1 days in the LE group. In Japan, rehabilitation is performed after surgery in the same department and hospital, so the duration of stay tends to be relatively long. An urban hospital in Japan reported that the average duration, until patients could go home for cases of femoral neck fracture, was more than 70 days [13, 14]. The department of Orthopedic Surgery in Numazu City Hospital attempted to transfer patients who had undergone operations without post-operative complications to rehabilitation facilities. However, this process took time depending on the circum- stances of the receiving facilities, which have also experienced difficulty discharging patients to home care because of the aging of society (elderly individuals cannot easily care for other elderly individuals with comorbidities).
This study was limited by its retrospective nature and small patient population. The incidence of femoral shaft fracture might have been low (58 cases in an 8-year period in a 0.2-million population city), and some patients with femoral shaft fracture might have been evacuated by the physician-staffed helicopter or sent to another hospital. We were also unable to investigate patients who had suffered a femur shaft fracture but whose medical chart did not list ‘the femur shaft fracture’ as the main disease (e.g. cases of multiple injury or cardiac arrest). Accordingly, more severely injured patients with femur shaft fractures might have been missed. Therefore, future prospective studies involving a greater number of patients, including those with mild trauma, will be needed.
CONCLUSION
Among patients with femur shaft fracture at a local hospital in a rural area of Japan, where the population is super-aging, the frequency of HE and LE femur shaft fracture was almost the same. This tendency may be due to the fragility of the femur shaft in elderly people.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The protocol of this retrospective study was approved by the review board of Numazu City Hospital and Juntendo Shizuoka Hospital, Japan on May 1st, 2019, and all examinations wereconducted in accordance with the standards of good clinical practice and the Declaration of Helsinki protocol/approval number is [298].
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
This manuscript received financial support from the Ministry of Education, Culture, Sports, Science and Technology (MEXT)-Supported Program for the Strategic Research Foundation at Private Universities, 2015-2019 concerning.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The constitution of total researching system for comprehensive disaster, medical management, corresponding to wide-scale disaster.

