All published articles of this journal are available on ScienceDirect.

Tibiotalar Arthrodesis Using a Hybrid Technique with a New Low-profile Anatomic Plate and Two Compression Screws: First One-year Results of Twenty Patients
Abstract
Background:
The aim of this prospective study was to evaluate and analyse the first clinical results of a recently developed low-profile anatomic plate in combination with two headless compression screws for tibiotalar arthrodesis.
Methods:
The case series involved 20 consecutive patients who underwent ankle arthrodesis using a hybrid technique. Radiographs were obtained at 6 and 12 weeks and 1 year postoperatively. The outcome was evaluated by using AOFAS and SF 12-questionnaire. Any complications related to the arthrodesis were recorded.
Results:
The follow-up rate was 100%. Patients mean age at the time of surgery was 60.1 years (range, 40-79). Arthrodesis with full weight-bearing occurred in every patient within 12 weeks postoperatively. There were no patients with delayed union, non-union, infection or implant failure. AOFAS Score and SF-12 scores increased considerably compared to preoperatively.
Conclusion:
The hybrid technique for ankle arthrodesis is a tibiotalar compression with screws in combination with rigid anterior plate fixation. Our clinical results demonstrated no implant failure, no infection and fusion in any of the 20 patients. Further studies are necessary to support our first results.
1. INTRODUCTION
Tibiotalar arthrodesis is the most common surgery for the treatment of end-stage ankle arthritis [1]. Despite an increase in total ankle replacement, patients with medical comorbidities are more likely to undergo arthrodesis [2]. More than 40 techniques for ankle arthrodesis have been described [3]. External fixation demonstrated inferior union rates compared with internal fixation and is recommended only for complex and severe cases [4]. Internal fixation can be performed using compression screws, as describedby Zwipp et al. and Mann et al. [5, 6]. Other techniques are anterior plating [7-10] or screw fixation in combination with a plate (hybrid arthrodesis) [11]. Biomechanical analyses have shown that the latter technique offers greater stiffness and rigidity [12, 13]. In clinical studies, this fusion technique showed similar complication rates as screw fixation only, but improved fusion rates [3, 14]. In our study, we used a recently developed low-profile anatomic plate in combination with two headless compression screws for ankle arthrodesis. The aim of this prospective case series was to evaluate and analyse our first clinical results of this hybrid technique by a prospective follow-up of 1-year postoperatively.
2. PATIENTS AND METHODS
Between 2015 and 2017, a total of 20 consecutive patients underwent open ankle arthrodesis using a hybrid technique. Within this period, no other arthrodesis techniques were performed. The fusions were performed by the senior author or under his supervision.
2.1. Surgical Technique
The same surgical technique was used for any patient. The patients were placed on a radiolucent table in a supine position, with straightened ankles at the distal end of the table. An intravenous single-shot antibiotic (Cefuroxime 1.5g) was given before incision. The leg was elevated, and a tourniquet was applied on the thigh. The surgeon was positioned in the front of the foot in standing position. All surgeries were performed using magnifying glasses with head-lights. Each surgery started with a longitudinal anterior skin incision of approximately 10 cm. Nerve- and vessel-sparing approach was used after the incision of the retinaculum. Langenbeck hooks or Hohmann retractors were used for tissue retraction. A sharp wound retractor was never used. Resection of the anterior joint capsule was performed, followed by the visualisation of the anterior joint cavity. Then, resection of the anterior tibial crest was performed with a chisel. The cartilage was completely removed from both joint surfaces, and sclerotic bone portions were resected using an arthrodesis spreader, chisels, sharp spoons, and Luers. Electronic devices (e.g. drillers) were never be used as these can produce bone necrosis through heat.
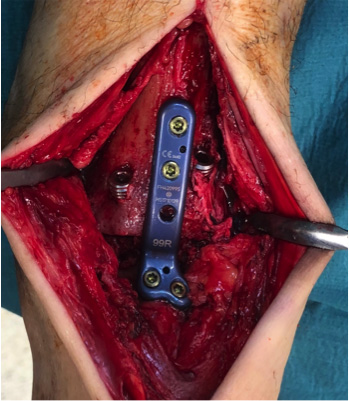
The same procedure was used for the medial and lateral ankle recesses. Both joint surfaces were reconstructed under multiple subcortical drills with a 1.8-mm K-wire. Irrigation was performed to prevent heat. The interposition of autologous cancellous bone taken from the ipsilateral iliac crest for the restoration of an orthograde joint configuration was optional but commonly performed. After manual joint positioning (90° neutral position, external rotation 5-10°), both target wires for the cannulated screws were inserted from the anterior-medial and anterior-lateral tibia into the body of the talus. A slight inward convergence was selected, but without crossing the screws within the talus. X-ray image converter verification in two standard planes (anterior and lateral) and repositioning was performed based on the requirement. It was followed by length measurements, over drilling, and insertion of the headless compression screws (HCS; Merete®). The HCS are self-drilling/self-tapping, dual pitched screws with a threaded head which can be countersunk into the bone. The diameter was always 6.5 mm in various lengths (about 44 to 55 mm). Then, the new anatomical plate (Tibiatalar fusion plate; Merete®; right or left plate design, 99° angle) was attached anteriorly (Fig. 1). The plate is made of a titanium alloy. Each plate was fixed with 2 or 3 screws of appropriate length in the distal tibia (mono- or bicortical) and talus (mono-cortical), respectively. The final step included X-ray verification for documentation, drainage without suction, closure of the retinaculum with resorbable sutures, subcutaneous sutures, skin closure with simple interrupted sutures, sterile dressing, deactivation of tourniquet, and fitting of a Vacuped-Walker® (OPED, Valley, Germany) in a neutral position.
2.2. Follow-up Treatment
Postoperative treatment included the immobilisation of ankle joints in a Vacuped Walker for 6 weeks, with a partial weight bearing of 20 kg using forearm crutches and accompanied by lymphatic drainage. After 6 weeks, the load was gradually increased to achieve full weight-bearing in the case of regular radiological findings. Full weight-bearing in ready-made shoes started about 12 weeks postoperatively. All patients received daily injections of low-molecular-weight heparin until full-weight bearing was achieved.
2.3. Clinical and Radiological Evaluation
All patients were investigated and evaluated with a validated translation version of the American Orthopaedic Foot and Ankle Society (AOFAS) scale [15] approximately one week before surgery. The pain, function and clinical alignment of the foot were evaluated using this scale. The function includes daily recreational activity, maximum walking distance, walking on different surfaces, gait abnormalities, sagittal motion, hindfoot motion and ankle-hindfoot stability. Moreover, we evaluated the physical and psychological status using the SF12-questionnaire, a self-administered general health outcome form. We used a validated translation version [16]. Arthritis (Fig. 2a) was graded according to the Bargon and Henkemeyer scale [17]. After surgery, all patients were examined with a clinical and a radiological follow-up (ankle antero-posterior and lateral) 6 weeks and 12 weeks postoperatively.
The final follow-up for this study including radiographs was done exactly one year postoperatively (Fig. 2b, 2c). At this time, the patients received examination again, and patients related outcome measurements were re-elevated. Computed tomography for the evaluation of a suspected non-union was not necessary for any patient.



2.4. Statistical Analysis
Statistical analysis was performed using SPSS for Windows (version 24.0; SPSS, Inc., Chicago, IL). Metric variables and measures of dispersion are reported as mean values. All tests of significance were bilateral, and p< 0.05 was statistically significant.
The study was approved by our institutional review board and performed according to the standards of the Declaration of Helsinki. All patients gave their informed consent for this study.
3. RESULTS
The mean age of the patient at the time of surgery was 60.1 years (range, 40-79), and 10 patients were women. The mean body mass index was 31.3 kg/m2 (range, 20-59). The indications for arthrodesis were post-traumatic arthritis (n=14), degenerative arthritis (n=5) and post-septic arthritis (n=1). Moreover, 7 patients had varus deformity, and 3 patients had valgus malalignment. The mean American Society of Anesthesiology (ASA) Score [18] was 2.3. Comorbidities included nicotine abuse (n=7), diabetes mellitus (n=4), 1x sarcoidosis (n=1), renal transplantation (n=1) and multiple sclerosis (n=1). Further descriptive data are shown in Table 1.
A total of 14 patients also received autologous spongiosa from the ipsilateral side of the anterior ilia wing. Application of the new plate after insertion of both compression screws was associated with no complications. The average duration for complete plating was 10 to 15 minutes. The mean duration of the surgery (incision to skin closure) was 108 min (range, 60-177), and the mean hospital stay was 7.2 days (range, 4-9).
All wounds healed primarily within 14 days, and no infection was detected until the end of this study. However, one patient required a postoperative revision for hematoma at the pelvic donor side. Fusion without suspected non-union was achieved with native radiographs in any patient between 6 and 12 weeks postoperatively.
The overall mean AOFAS Score [15] significantly increased from 52.2 points preoperatively to 72.4 points postoperatively (p= 0.032) (Table 2). The physical subscore of the SF 12 questionnaire [16] showed a significant improvement from 27.0 preoperatively to 37.8 postoperatively (p= 0.042) (Table 1). The mental subscore of the SF 12 questionnaire [16] was without significant difference (p= 0.824).
4. DISCUSSION
This study was conducted to summarize the results of a recently implemented anatomic low-profile plate in combination with two headless compression screws for the treatment of tibiotalar arthrodesis.
Up to date, there are only two biomechanical studies that have investigated the stability of a hybrid arthrodesis. Tarkin et al. used a human anatomical specimen and showed that an additional anterior plate increases the rigidity of arthrodesis with screws only [13]. Clifford et al. used an artificial bone model and compared screws, plate, and hybrid arthrodesis, with the latter showing the highest rigidity [12]. Based on these results, we conducted this clinical study to investigate the effects of this hybrid technique with a low-profile anatomic plate in situ. Therefore, we also reported any possible complications in relation to the arthrodesis.
Most clinical studies have investigated arthrodesis with screws or plates [19]. In detail, those studies demonstrated a fusion rate of 98% for isolated anterior plate arthrodesis [19], and 88-100% for isolated screw arthrodesis, depending on the technique and the number of screws. Only three studies have investigated the combination of both techniques (Table 2). Overall, high fusion rates in these studies were also reported from 92% to 100% [3, 11, 14], which confirm our results with a fusion rate for any of the patients (100%).
| Age | Sex | BMI |
Time to Fusion Weeks |
SF12-pre Physical Subscore |
SF12-Pre Mental subscore |
SF12-Post Physical Subscore |
SF12-Post Mental Subscore |
AOFAS Pre |
AOFAS Post |
|---|---|---|---|---|---|---|---|---|---|
| 75 | f | 30.8 | 12 | 24.2 | 42.8 | 31.2 | 61.9 | 15 | 66 |
| 68 | f | 30.5 | 6 | 19.4 | 35.2 | 26.3 | 34.9 | 37 | 55 |
| 37 | f | 58.8 | 6 | 44.1 | 43.8 | 48.3 | 48.4 | 64 | 84 |
| 45 | m | 40.4 | 6 | 25.6 | 59.5 | 27.6 | 54.1 | 60 | 63 |
| 57 | f | 26.8 | 6 | 16.8 | 35.0 | 28.3 | 45.2 | 51 | 78 |
| 57 | m | 26.1 | 6 | 34.7 | 29.7 | 55.5 | 57.8 | 66 | 88 |
| 73 | m | 31.6 | 6 | 20.5 | 30.2 | 28.4 | 38.3 | 58 | 63 |
| 71 | m | 27.0 | 6 | 29.4 | 35.6 | 34.9 | 39.2 | 56 | 68 |
| 48 | m | 26.7 | 12 | 33.9 | 54.3 | 42.6 | 52.8 | 52 | 78 |
| 60 | f | 38.1 | 12 | 40.4 | 29.1 | 48.6 | 37.4 | 49 | 71 |
| 51 | m | 27.7 | 12 | 19.5 | 54.1 | 29.2 | 56.5 | 40 | 61 |
| 58 | m | 29.4 | 6 | 22.8 | 24.4 | 27.8 | 36.3 | 43 | 61 |
| 38 | m | 24.9 | 12 | 37.3 | 47.4 | 44.5 | 53.7 | 51 | 74 |
| 70 | f | 28.7 | 6 | 21.6 | 57.5 | 31.9 | 66.2 | 71 | 89 |
| 40 | f | 35.2 | 12 | 39.4 | 42.3 | 46.1 | 52.4 | 63 | 71 |
| 79 | f | 20.8 | 6 | 29.1 | 32.4 | 39.0 | 39.3 | 56 | 77 |
| 56 | m | 26.4 | 6 | 29.5 | 21.5 | 37.9 | 29.1 | 52 | 75 |
| 73 | f | 31.2 | 12 | 28.8 | 56.7 | 38.5 | 62.2 | 40 | 64 |
| 74 | m | 33.0 | 6 | 16.8 | 35.0 | 39.2 | 49.1 | 49 | 68 |
| 73 | f | 31.2 | 12 | 41.6 | 50.7 | 50.0 | 58.8 | 71 | 93 |
|
Study year |
Authors |
Patients n |
Type of Arthrodesis |
Follow-up Months |
Fusion Rate % |
Infection Rate % |
Revision Rate % |
|---|---|---|---|---|---|---|---|
| 2006 | Kakarala | 11 | Screws + non-locking plate | 26.8 | 100 | Not given | Not given |
| 2017 | Mitchell | 39 | Compression screw + anterior locking plate | 17 | 92.3 | 5.2 | 2.6 |
| 2017 | Prissel | 46 | Lag screw + anterior locking plate | 9 | 97.9 | 8.5 | 2.1 |
| 2019 | Own study | 20 | Compression screw + anterior locking plate | 18 | 100 | 0 | 0 |
In this study, the mean period of time until fusion was within 12 weeks. However, the exact time data is not available because no radiographs were performed between 6 weeks and 12 weeks. According to hybrid arthrodesis, no studies provide exact data when fusion occurred. Careful joint preparation using magnifying glasses and head torch as well as cancellous bone augmentation had positive effects on the fusion rate, but evidence is still lacking. Bone graft was performed supplementary in 75% of patients, which was considerably higher compared with two studies reporting 18% and 36% [3, 11]. However, bone graft harvesting from the iliac crest was the reason for one revision in our sample; but no patient complained about donor site discomfort at the time of follow-up.
The fusion of the arthrodesis was revealed with X-ray imaging exclusively. However, if any complication had been suspected, we would have done computer tomography at 12 weeks post-surgery or later. No case of suspected infection was observed in our sample based on laboratory values or clinical examination. Comparable studies reported infection rates of 5.2% to 8.5% with surgical revision rates of 2.1% to 2.6% [3, 14]. Both results (no infection and highest fusion rate) are important aspects when considering the morbidity of our sample. Accordingly, 75% of our patients suffered from comorbidities such as diabetes or had nicotine abuse. The study of Mitchell et al. [3] included fewer patients with diabetes or nicotine abuse (21% and 13%; respectively). Other studies provided no information according to comorbidities, or patients with severe diseases were excluded [11]. The mean body mass index (kg/m2) of 31.3 in our study demonstrated almost obese patients, but this was similar compared with the other studies (33.0 and 32.7; respectively) [3, 14]. No patient complained about device-related irritations at the final follow-up. According to those irritations, two studies with anterior plate arthrodesis revealed complication rates of 15% and 21% [3, 14]. We conclude, that this is the result of the overall low profile of the anatomic plate (Fig. 1). However, in combination with two compression screws, it provided enough stability, considering the fusion rate of 100% with no case of implant failure.
Mean AOFAS score showed a significant improvement from 52.2 preoperatively to 72.4 postoperatively. In comparison with the study of Karakala et al. [11] our mean AOFAS score was lower. Scores between 44 and 85 were reported for the different arthrodesis procedures [4, 5]. The morbid sample can be an explanation for the obtained lower scores.
Our study had some limitations. According to the small sample and the type of study design with no randomisation or control group, our case series is not generally valid. Furthermore, our study presents only short-term results; therefore, further complications such as late infections can still occur.
CONCLUSION
The hybrid technique is a combination of tibiotalar compression with screws and an anterior plate fixation. The technique in this study described two headless compression screws and a low-profile anatomical plate. The clinical results demonstrated no failure, no infection and fusion in any of the treated 20 patients. Further studies are necessary to support our first results. The only limitation of this low-profile anatomic plate is the higher cost compared with the standard open technique using only screws.
LIST OF ABBREVIATIONS
| AOFAS | = American Orthopaedic Foot and Ankle Society Scale |
| HCS | = Headless Compression Screws |
AUTHOR'S CONTRIBUTIONS
CE undertook significant involvement in manuscript construction and revisions, data collection and analysis.
BF provided mentorship and study design.
FM provided significant guidance with manuscript writing, manuscript revisions and study design.
All authors have read and approved the final manuscript
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was obtained from the local hospital ethics committee of Hospital Barmherzige Brüder Prüfeninger Germany.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all the participants.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

