All published articles of this journal are available on ScienceDirect.

The Combined Lambrinudi and Ankle Arthrodesis with Ring External Fixation in the Long-term Severe Neuromuscular Equinocavovarus Deformity with Ankle and Hindfoot Osteoarthritis: The Cases Presentation and Modified Guideline of Treatment
Authors Info & Affiliations
Abstract
Background:
Severe equinocavovarus deformity develops from various causes and generally results in major disability that affects patient’s mobility and quality of life. It can be divided into neuromuscular and non-neuromuscular deformities, including two major subtypes: i.e., paralytic and spastic. In addition, ankle osteoarthritis could be caused by prolonged or progressive foot deformity.
Objective:
The present report proposes a modification of the accepted treatment algorithm and Lambrinudi’s surgical technique with ankle and hindfoot arthrodesis to correct theses challenging deformities with the long-term condition.
Results:
Two equinocavovarus cases were included, one in a 54-year old male and the second in a 63-year old female with paralaytic and spastic etiologies respectively. Patient’s deformity correction was acceptable. Each patient demonstrated improved outcomes due to a postoperative plantigrade foot and ankle position. No significant complications were encountered during the course of care and last follow-up. The mean follow-up time was 26 months.
Conclusion:
Severe long term neuromuscular equinocavovarus deformities are a challenging disability in the foot and ankle surgery. The present article proposes a modified guideline of treatment illustrated in two representative case studies of long-term paralytic and spastic equinocavovarus deformities. These conditions can be treated surgically using the stepwise approach as demonstrated in this article with acceptable outcomes.
1. INTRODUCTION
Neuromuscular disorders afflicting foot and ankle are either spastic or paralytic type. Spastic disorders involve upper motor neurons and include head injury, cerebral palsy, stroke, and spinal cord injury. Paralytic disorders involve lower motor neurons and their causes include Charcot-Marie-Tooth disease, peripheral nerve laceration, and poliomyelitis [1]. Aggressive manipulation to correct equinus in rigid equinocavovarus may lead to tibial nerve and vessel compression, which is deleterious to neurovascular structures and to the recovery of the wound [2-4]. These disorders are problematic because they cause difficulty in ambulation and in performing day to day activities. In addition to difficulty in wearing shoe wear, painful callosities and non-healing ulcer may develop due to long term condition. The deformity becomes progressive and may lead to further deterioration.
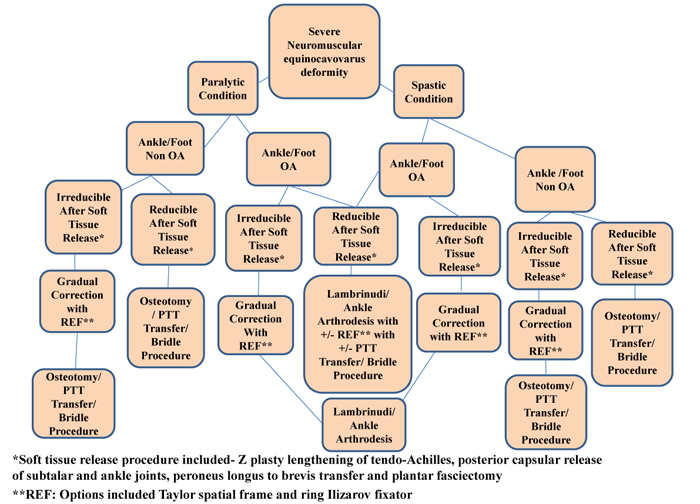
Various surgical procedures like soft tissue release, osteotomy, arthrodesis, and external fixator application have been described, but little is known about the optimal protocol for surgical treatment of severe equinocavovarus deformity in the hindfoot and ankle osteoarthritis especially in long-term conditions. The purpose of the present study was to develop and modify management guidelines described by Lee et al. (Fig. 1) Lee et al., proposed a guideline for cavovarus correction with ankle sparing treatment. In our study, we adapt their guidelines for the reduction of foot-ankle deformity to achieve more plantigrade position. If the joints cartilage has become deteriorated and arthritic due to long term deformity, we opt for joint arthrodesis. Again, if the joint cartilages are still in viable conditions, we select the ankle sparing treatment as stated by Lee et al., in their guidelines [5]. The modified guidelines discussed in the present study were also preliminarily applied in the senior authors’ previous study by Manggala et al. [6], demonstrating the effective outcome of the treatment. Therefore, the present study also aims to describe the modified guidelines in detail and the operative techniques for correcting these challenging equinocavovarus deformities with or without hindfoot and ankle osteoarthritis. All the patients gave consent to the operative procedures and publication of this report.
2. CASE DESCRIPTION
The present study describes two challenging cases with long-term equinocavovarus deformity (Table 1).
2.1. Case I
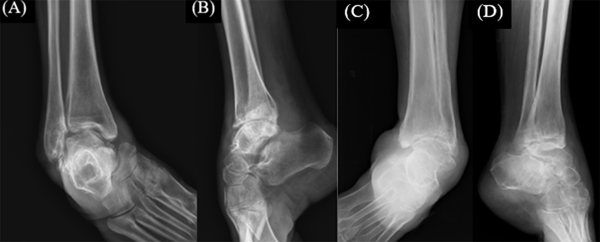
The first patient was a 54-year-old male who presented with a paralytic right foot and ankle equinocavovarus deformity. The patient complained of the onset of deformity in childhood (Fig. 2). He had normal sensation in the dermatomal distribution of his involved foot and ankle with grade 2 motor power weakness in tibialis anterior and peroneus brevis. The clinical examination revealed lower motor neuron type of palsy. The equinus deformity was 59 degrees plantar flexion, and he was diagnosed provisionally with post-polio syndrome. Preoperative X-rays revealed ankle and subtalar osteoarthritis (Fig. 3 A, B).
| Case I: Paralytic equinocavovarus deformity without spasticity Various soft tissue release procedures* Equinus not reducible Gradual correction of equinus deformity with REF** After correction of equinus to neutral Definitive internal fixation with Lambrinudi and ankle arthrodesis |
Case II: Spastic equinocavovarus deformity Various soft tissue release procedures Equinus reduced to neutral Definitive procedure with Lambrinudi and ankle arthrodesis. Internal construct supported with external REF for alignment and additional compression. Tibialis posterior tendon transfer to decrease the inversion spasm and the efforts to maintain the foot alignment in neutral flexion and mild eversion. |
|
*Soft tissue procedures consisted of Z-lengthening of tendo Achilles, posterior capsular release of the ankle/subtalar joints, peroneus longus to brevis transfer and plantar fasciectomy **REF: Ring External Fixation, options are the Ilizarov and the Taylor spatial frame |
|

A staged procedure was initially proposed, which was to be performed if equinus was not corrected following soft-tissue release. Due to incomplete correction of equinus by the soft tissue procedure alone, gradual correction of equinus was performed with a Ring External Fixator (REF) at the same time. After 38 days, REF was removed and definitive Lambrinudi and ankle-hindfoot arthrodesis was performed due to the arthritis of ankle-subtalar joints and rigid cavovarus. Triple arthrodesis was performed as described by Lambrinudi [7] in 1927, with an anteriorly based wedge resection of talus and calcaneus followed by fusion of the talus to the navicular. This was followed by subtalar and calcaneocuboid arthrodesis.
2.1.1. Operative Techniques
2.1.1.1. Double-Stage Operation
First-stage operation: Under spinal anesthesia, the patient was kept in a prone position. Tourniquet was applied. Z-plasty lengthening of the Achilles tendon was completed followed by posterior capsular release to correct equinus. Plantar fasciectomy was completed in order to correct cavus. For bony correction of cavus, a dorsiflexion osteotomy of the first metatarsal was performed along with peroneus longus to brevis transfer to assist in the correction of cavus and adduction of forefoot caused due to peroneus longus overpowering its antagonists.
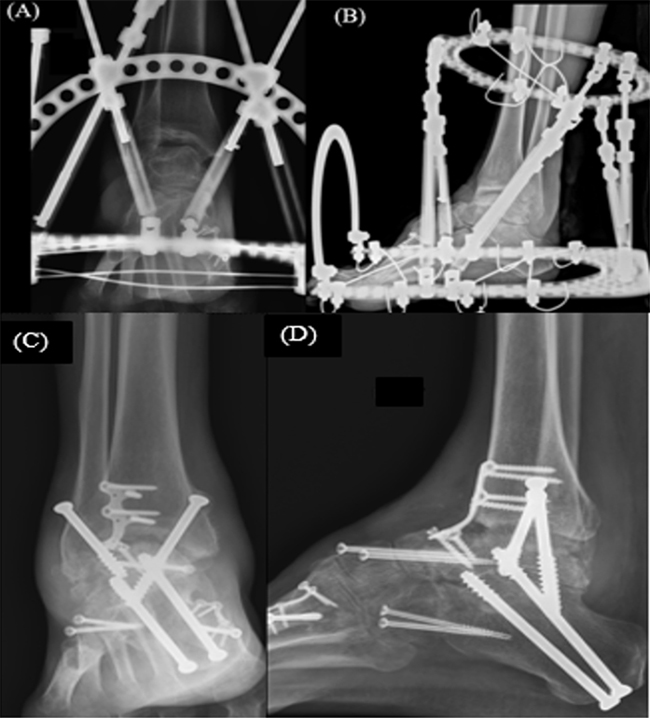
The equinus deformity to plantigrade position could not be achieved after soft-tissue release; therefore, gradual correction of equinus with a REF (Taylor spatial frame) was the next step in the treatment procedures. The patient was placed in supine position. Two olive wires were placed proximally in the tibial shaft, two in the calcaneus, and two wires were passed through all the metatarsals placed in divergent directions. A hexapod frame was applied and all the wires were tensioned to 110 Newton (Fig. 4 A, B).
Based on online software calculation, deformity correction was done which allowed daily length adjustment from the first postoperative day until all the struts completed the required length for correction. Radiographs were performed once every 2 to 3 weeks to check the correction of deformity.
Second-stage operation: This was performed 5 weeks following the first procedure after pin tract infection was ruled out.
2.1.2. Lambrinudi Arthrodesis
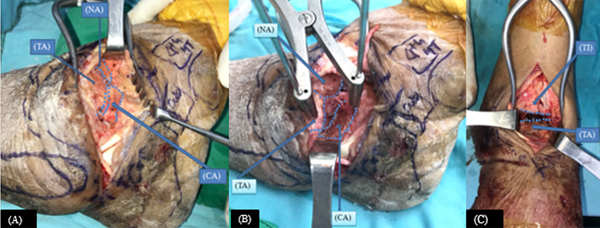
The incision for the Lambrinudi procedure extended from the tip of the fibula up to the base of the lateral cuneiform, passing over the anterior process of calcaneus and lateral aspect of talonavicular joint. Wedge resection of talus and navicular were performed including the anteroinferior aspect of the talar head and proximal surface of the navicular followed by calcaneal debridement. After visualization of cancellous bone, the remaining talar head was then inserted over the inferior edge of the navicular, which reduced the forefoot to the hindfoot. Then calcaneocuboid joint was debrided (Fig. 5 A, B). This was followed by fixation of subtalar and calcaneocuboid joints with screws.
2.1.3. Ankle Arthrodesis
An anterior approach for the ankle was used. Joint debridement was done and talus was anatomically aligned (Fig. 5 C). To assess the alignment of arthrodesis, the angle formed by the long axis of tibia and the body of talus in neutral position compared with that of normal contralateral side in neutral position should be equal [8, 9]. Attempts were made to adjust the foot into plantigrade position. Finally, tibiotalar fixation was carried out with cannulated screws augmented with the anterior compression plate. The wound was closed in layers.
2.2. Case II
The second patient’s presentation describes spastic equinocavovarus deformity. Equinus deformity of this case was partially reducible and corrected to a lesser equinus position after soft tissue release. This was followed by Lambrinudi and ankle arthrodesis. Again, the construct was further augmented with REF.
The patient was a 63-year-old woman with deformity over left foot and ankle as a complication of encephalitis at the age of 8 years. She had diminished sensation over dermatomal distribution of foot and a grade 0 motor power weakness involving the tibialis anterior and peroneus brevis. The tone of posterior compartment group of muscles was spastic. There was no availability of preoperative clinical picture. Based on lateral X-ray of her foot, the equinus deformity was 43 degrees plantar flexion. X-rays revealed hindfoot and ankle arthritis (Fig. 3 C, D).
2.3. Operative Techniques
Endoscopic gastrocnemius recession was initially performed, but Silfverskiold test was still positive. Therefore, Z-plasty lengthening of Achilles tendon was performed. This was followed by posterior capsular release and plantar fasciectomy. Dorsiflexion osteotomy of the first metatarsal along with peroneus longus to brevis transfer was performed to correct plantar flexion deformity of the first ray. We could obtain plantigrade position of foot after soft-tissue release procedure; therefore, a single-stage operation with definitive correction of deformity was planned.
Lambrinudi procedure was performed using the same technique as in the first patient with an anterolateral approach to the ankle, talonavicular, calcaneocuboid joints, and a sinus tarsi approach for the subtalar joint. Lambrinudi arthrodesis was completed and secured with locking plates and screws. Ankle and subtalar arthrodesis was fixed by retrograde intramedullary nailing (Fig. 6 A, B).

The senior surgeon preferred the use of an Ilizarov frame to augment arthrodesis and maintain alignment in patients with spastic disorders (Fig. 6 A, B).
Finally, posterior tibial tendon transfer to the lateral cuneiform was performed due to the presence of inversion spasticity. Tendon harvesting was done prior to application of the Ilizarov fixator and the transfer was completed after fixator application. Cavus was not completely corrected in this patient because there was a contracture problem which was due to extensive scar on the plantar surface of the foot as a result of a previous procedure completed at an alternate hospital. The senior surgeon decided to accept plantigrade position and not perform further corrective procedure of midfoot to correct cavus. This avoided potential soft-tissue complications of her sole. The wound was closed in layers.
2.4. Post-Operative Management and Rehabilitation
A posterior splint was applied for the next 2 weeks. Sutures were removed during the second week follow up visit (Fig. 7). Then, a removable short-leg cast was applied in the compliant patient with non-weight bearing for 10 weeks. In noncompliant patients, non-removable short leg casts were required for a period of 10 weeks. Weight bearing as tolerated was resumed if radiological (Figs. 4 C, D and 6 C, D) and clinical union was observed at arthrodesis site (Fig. 8). In case II, Ilizarov frame was removed 6 weeks after operation, when early union signs were observed at arthrodesis sites on radiographic assessment. After cast removal, the patients were taught to practice standing position, weight shift, and small periods of walking followed by increased time of walking distance 12 weeks postoperatively. Balance and proprioceptive exercises were also begun. Scar massage, heat application, and joint mobilization to unfused joints were initiated. Progressive strengthening of hip, knee and ankle along with core strengthening exercises was also encouraged.

Patient’s deformity correction in the present study was not completely perfect. However, each patient demonstrated improved outcomes in terms of acceptable plantigrade foot and ankle alignment with reduced risk of potential future pressure ulcer. The overall results showed improved Thai Visual Analog Scale Foot and Ankle (VAS-FA) (mean preoperative VAS-FA: 37; postoperative VAS-FA: 47.4), and Health-related Quality of Life via Thai Short-Form 36 (SF-36) scores (mean preoperative SF-36: 64.6; postoperative SF-36: 76.5) [10, 11]. There was a correlation between VAS-FA and SF-36 scores (Pearson Correlation Coefficient (r) = 0.684; P-value = 0.520). Patients in the present report did not report any significant complications during the latest follow-up. The mean follow-up time was 26 months. The similar guideline was also preliminarily applied in the senior authors’ previous study by Manggala et al. [6], in which residual foot-ankle deformity /injury was corrected in 14 patients. The overall result was satisfied in terms of foot and ankle outcome and quality of life scores. The authors believe that the modified guideline in this report has the potential and advantages in the management of challenging equinocavovarus deformities in the orthopedic practice.
3. DISCUSSION
Multiplanar equinocavovarus foot and ankle deformities in neuromuscular disorders are associated with or without severe joint stiffness, osteoarthritis, and soft-tissue contracture and pose a significant challenge to the use of conventional correction methods especially in the long-term condition.

In the first patient, REF was used to provide gradual correction of irreducible equinus before definitive Lambrinudi and ankle arthrodesis. Because of long term deformity in the first patient, the soft tissues around the ankle became stagnated due to which it was difficult to achieve optimal overall correction and we accepted the plantigrade position. In the second patient, REF was used to prevent the recurrence of equinus and maintain alignment. The second case had significant spasticity of all posterior compartment muscles resulting in long-term deformity. Despite soft tissue release, there was continuous spasticity of the remaining posterior muscles [3]. Thus, there was a risk of recurrent equinus in the splint postoperatively even after performing Lambrinudi and triple arthrodesis. Hence, REF construct was augmented to nullify the effect of muscle spasticity and maintain the alignment of foot, thus providing additional compression with lower complications [6, 12].
Nineteen patients were studied by Elsner et al. [13] who underwent Lambrinudi procedure and demonstrated subsequent significant improvement in their American Orthopaedic Foot & Ankle Society and Short Form-36 scores. Bernua et al. [2], demonstrated similar findings in 50 feet following Lambrinudi procedure, where 42 patients had experienced good outcome. Tang et al. [14], suggested that Lambrinudi procedure is a useful method for treating severe rigid equinus deformities. Saltzman et al. [15], studied 55 patients with neuromuscular disorder where triple arthrodesis was performed. Ninety-five percent of these patients were satisfied with the operation results. Provelengios et al. [4], studied 24 patients who underwent a one-stage pantalar arthrodesis at an average duration of follow-up at 37.2 years, with good results. Consistent with the outcomes of above-mentioned studies, the author’s previous study demonstrated satisfactory outcomes of surgical treatment using the present study’s modified guidelines of treatment [6]. In addition, the present guideline highlights the benefit of combined technique with osteotomy, arthrodesis, and REF to correct challenging equinocavovarus conditions, specifically long-lasting ones. Regarding potential complications, pseudarthrosis has been reported in up to 28% of patients following pantalar arthrodesis with ankle and talonavicular joints being the most common areas of non-union [16-18]. These potential complications were addressed and likely prevented by using the combined technique of Lambrinudi, and ankle arthrodesis with augmentation and further stabilization of arthrodesis using REF. REF likely provided additional compression and potentially reduced the probability of pseudarthrosis. Although the final results of the patient’s deformities correction in the present study were not completely perfect, each patient demonstrated improved outcomes in terms of plantigrade foot and ankle position that likely reduced the risk of future pressure ulcers. In addition to these evidence, the similar guideline was also preliminarily used in the senior author’s previous study by Manggala et al. [6], in which residual foot-ankle deformity/injury was corrected in 14 patients. The overall result was satisfactory. Thus, the modified guideline algorithm and surgical technique in the present study may be utilized as a recommended protocol in the future to achieve satisfactory results. The well-aligned corrections of deformities potentially reduce the risks of complications such as pseudarthrodesis and soft-tissue compromise.
CONCLUSION
Severe long term neuromuscular equinocavovarus deformities are a challenging disability in foot and ankle surgery. The present article proposes a modified guideline of treatment illustrated in two representative case studies of long-term paralytic and spastic equinocavovarus deformities. Both the patients in the study demonstrated acceptable plantigrade foot and improved ankle alignment during the latest follow up. There was an improvement in the various qualitative and quantitative parameters which are listed above. These conditions can be treated surgically using the stepwise approach as demonstrated in this article with acceptable outcomes.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
All thepatients gave consent to the operative procedures and publication of this report.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

