All published articles of this journal are available on ScienceDirect.

Characteristic Movement of the Ribs, Thoracic Vertebrae while Elevating the Upper Limbs - Influences of Age and Gender on Movements
Abstract
Background:
The rib cage, such as the thoracic spine and ribs, influences glenohumeral mobility and the development of shoulder disorders.
Objective:
To evaluate movements of the ribs, thoracic vertebrae during bilateral arm elevation and to clarify the characteristic influences of age and gender.
Methods:
Subjects comprised 33 healthy individuals divided into a young group (10 males, 7 females; mean age, 25 years) and a middle-aged group (8 males, 8 females; mean age, 52 years). Chest CT was performed with two arm positions: arms hanging downwards; and arms elevated at 160°. Images were three-dimensionally reconstructed to evaluate rib movement, extension angle of thoracic vertebrae.
Results:
Maximal movement was observed at the fifth rib, and rib movement decreased with increasing distance from the fifth rib in both the groups. In males, movement of the second to fourth ribs was smaller in the middle-aged group than in the young group (p < 0.05). Movement of the first to ninth ribs was smaller in females than in males (p < 0.05). No significant difference in the extension angle of the thoracic vertebrae was found.
Conclusion:
Fifth rib movement is the largest among all ribs during bilateral arm elevation. Reduction of upper rib movement initially arises as an age-related degradation in males. Women exhibit less rib movement during bilateral arm elevation.
1. INTRODUCTION
The influence of the rib cage, such as the thoracic spine and ribs, on glenohumeral mobility and the development of shoulder disorders are interesting clinical and biomechanical topics. However, neither thoracic spine and ribs movement during elevation of the upper limbs nor the mobility changes with the influence of ageing and gender have been adequately investigated in the clinical practice. The biomechanical properties of the human ribs and thoracic spine during arm elevation are also largely unknown, since many studies have mainly focused on movements of the glenohumeral and the scapulothoracic joints.
Humeral, scapular, and thoracic segments demonstrate synchronous interactions during arm elevation [1]. When healthy individuals elevate their arms, the humeral head is rotated externally, and the scapula is elevated, rotated upwardly and internally, and tilted posteriorly, adjusting the positional relationship between the humeral head and the glenoid cavity [2, 3]. The upper thoracic spine shows extension, side flexion, and axial rotation during unilateral arm elevation, however during bilateral arm elevation in the sagittal plane produces thoracic extension but no axial rotation and side flexion [1, 4].
Flexibility decay of the trunk and shoulder joint accelerates over middle age in both males and females [5]. A scapular restriction of depression, downward rotation, and posterior tilt was described in comparison between healthy individuals in their 20s and in their 50s, and which may be a critical cause of frozen shoulder [6]. A disturbance of scapular motion that generates stress under the acromion and malalignment in the glenohumeral joint leads to shoulder disorders [7, 8]. Thus, regression of scapular and thoracic spine movement leads to decreased shoulder joint motion, and consequently results in shoulder disorders such as impingement syndrome, frozen shoulder, and degenerative rotator cuff tears.
Analysis of ribs movement has not been sufficiently conducted due to the anatomic characteristics of the rib cage and the complexity of the rib movement, which includes the sternum and the 24 ribs consisting of the rib bone and costal cartilage. If we are able to investigate the amount of movement in each rib or the level of thoracic spine movement during arm elevation, the kinematic properties for shoulder disorders could be interpreted further. The purposes of this study were to evaluate the elevation of each rib and the extension of the thoracic vertebrae during bilateral arm elevation in healthy individuals and to clarify the characteristics with the differences of age and gender.
2. MATERIALS AND METHODS
2.1. Participants
With the approval of the hospital ethics committee, this study was conducted after obtaining informed consent from the subjects (IRB number: 2805). Participants were recruited from the medical staff of Okubo Hospital. Subjects were healthy individuals (18 males, 15 females) with no history of trauma or disorders of the shoulder. We classified subjects into two groups to evaluate the movement of the ribs, thoracic vertebrae during arm elevation and compare differences in terms of age and gender. The young group comprised of 10 males and 7 females in their 20s (mean age, 25 years; range, 21-29 years). The middle-aged group consisted of 8 males and 8 females (mean age, 52 years; range, 43-64 years). Chest computed tomography scanning (CT) (64-row multi-slice CT, AquilionTM64; TOSHIBA, Tokyo, Japan) was carried out during inspiration in the supine position using two arm positions: upper limbs hanging downwards; and upper limbs elevated at 160° (Fig. 1). The resulting images were three-dimensionally reconstructed into anterior-posterior and lateral views of the skeletal structure to evaluate the distance of rib movement, extension angle of the thoracic vertebrae. For the position when the upper limbs were elevated, the subject elevated both their arms forward to the most comfortable position up to 160°, and then underwent measurement from the sagittal plane. In addition, women wore hospital gowns without their underwear for the examination and while taking images. The methods for measuring rib movement, extension angle of the thoracic vertebrae are shown below.
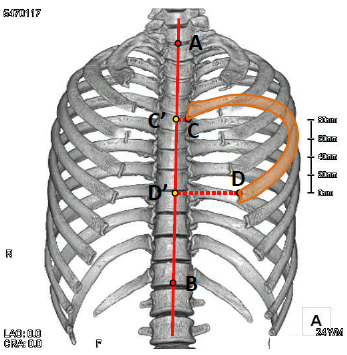
2.2. Movement of the Ribs (Fig. 2)
Although the measurement method of the left fifth rib is shown as an example in Fig. (2), all ribs were also measured by the same method. In the anterior-posterior view, with the center of the line between the seventh cervical vertebra and the first thoracic vertebra designated as Point A and the center of the line between the twelfth thoracic vertebra and the first lumbar vertebra designated as Point B, the straight line AB was drawn. Point C is the proximal end on the caudal side of each rib, while Point D is the distal end on the cranial side of each rib. The designated location of Point C was on the caudal side because the proximal ends of the first and second ribs were inclined toward the horizontal, making the cranial side difficult to evaluate. The designated location of Point D was on the cranial side because age-related ossification of the costal cartilage starts caudally, which may make evaluation on this side difficult. Perpendicular lines were drawn from Points C and D to the straight line AB, with the intersections taken as Points C' and D', respectively. Distance C'D' was measured. Based on distance C'D' with the upper limbs hanging downwards, the change to C'D' with the upper limbs elevated up to 160° was taken as the movement of the ribs. To correct for differences in the size of the thorax between subjects, a correction value was calculated for evaluation by multiplying the distance of rib movement by the ratio of length AB for each subject to the mean of length of AB for all subjects.
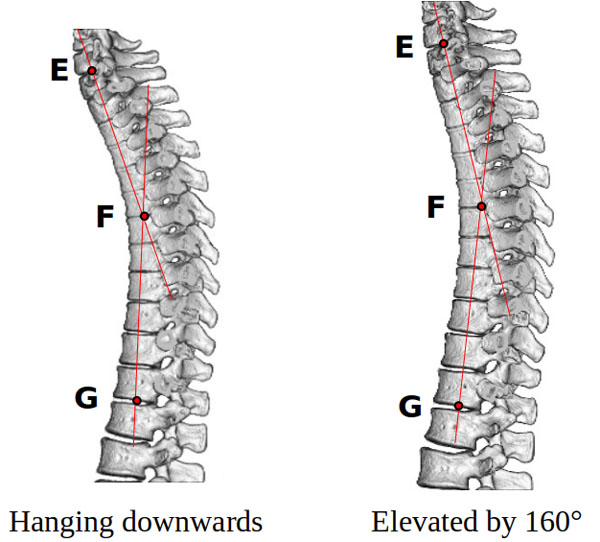
2.3. Extension Angle of Thoracic Vertebrae (Fig. 3)
In the lateral view, Point E is the center between the seventh cervical vertebra and the first thoracic vertebra, Point F is the midpoint between the sixth thoracic vertebra and seventh thoracic vertebra, and Point G is the center between the twelfth thoracic vertebra and first lumbar vertebra. Based on the value of angle EFG (<EFG) with the upper limbs hanging downwards, the change in <EFG at the position with bilateral arm elevation of up to 160° was taken as the extension angle of the thoracic vertebrae.

2.4. Reliability of Measurements
Intraclass correlation coefficients (ICCs) were calculated as indicators of intra- and inter-rater reliabilities of measurements of rib movement, angles of extension of the thoracic vertebrae. Measurements were made by one orthopedic surgeon and two physiotherapists. Three members of both the young and middle-aged groups were selected at random, and rib movement, angle of extension of the thoracic vertebrae were each measured twice, and the ICCs were calculated.
2.5. Statistical Analysis
For statistical analyses, Mann-Whitney's U test was used, with values of p < 0.05 regarded as indicating a significant difference. One- or two-way analysis of variance (ANOVA) was used to calculate intra- and inter-rater ICCs for movement of the ribs, extension angle of the thoracic vertebrae. All statistical analyses were conducted using the SPSS software package (version 25; SPSS, Chicago, USA).
3. RESULTS
3.1. Reliability
Intra-rater ICC (1,2) was 0.97 for movement of the ribs, 0.91 for extension angle of the thoracic vertebrae. Inter-rater ICC (2,3) was 0.92 for movement of the ribs, 0.85 for extension angle of the thoracic vertebrae. All reliability coefficients exceeded 0.8, indicating that the measurement methods used in this study were reliable.
3.2. Movement of the Ribs
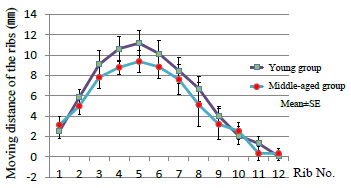
Mean movement of each rib (the first to twelfth ribs) when elevating bilateral arm up to 160° from the position with the upper limbs hanging downwards was 6.0 mm in the young group (maximum, 11.2 mm at the fifth rib) and 5.2 mm in the middle-aged group (maximum, 9.4 mm at the fifth rib) (the first to twelfth ribs: p = 0.62, fifth rib: p = 0.12). Regardless of age, the largest movement was observed at the fifth rib and the farther from the fifth rib, the smaller the movement of the rib (Fig. 4).
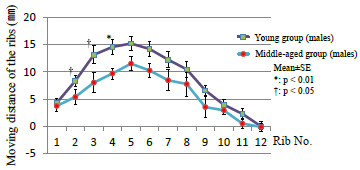
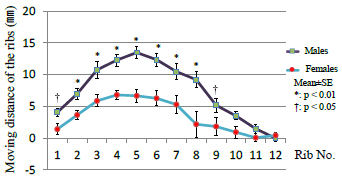
No difference was present between the age groups overall. When comparing groups in terms of gender, regarding males, mean movements of the second to fourth ribs in the young group were 8.4 mm, 13.2 mm, and 14.6 mm, respectively, compared to 5.4 mm, 8.1 mm, and 9.7 mm in the middle-aged group. Movements of the second to fourth ribs were thus significantly smaller in the middle-aged male group than in the young male group (p < 0.05) (Fig. 5). No difference was found between the female age groups (p = 0.089). A comparison between males (young and middle-aged men) and females (young and middle-aged women) found that mean movements by the first to ninth ribs were 4.1 mm, 7.0 mm, 10.8 mm, 12.3 mm, 13.5 mm, 12.4 mm, 10.5 mm, 9.2 mm, and 5.2 mm, respectively, in males, and 1.4 mm, 3.6 mm, 5.9 mm, 6.8 mm, 6.7 mm, 6.3 mm, 5.3 mm, 2.2 mm, and 1.8 mm, respectively, in females (p < 0.05) (Fig. 6). Women thus exhibited smaller rib movements when compared with men.
3.3. Extension Angle of the Thoracic Vertebrae
Mean extension angles of thoracic vertebrae during bilateral arm elevation of up to 160° from the starting position, were 3.4° in the young group and 3.8° in the middle-aged group, showing no significant difference (p = 0.96). When comparing groups in terms of gender; males showed mean angles of 4.1° in the young group and 3.9° in the middle-aged group, while females showed angles of 2.2° in the young group and 3.7° in the middle-aged group, again showing no significant differences (male: p = 0.23, female: p = 0.18). Comparison by gender between male and female groups found no significant difference (p = 0.15), with mean angles of 2.6° in men and 2.8° in women. The extension angle of the thoracic vertebrae displayed no differences in terms of age or gender.
4. DISCUSSION
This study provides the first evidence that the fifth rib shows the largest amount of movement during bilateral arm elevation and the ribs located farther from the fifth rib indicate a lower value of elevation regardless of age or gender. The ribs and the thoracic vertebrae forming the thorax generate coordinated movements as a single unit, and the scapula forming the shoulder joint with the humeral head floats on the rib cage. Rib movement would therefore influence shoulder joint motion. Chest wall procedures were postoperatively associated with shoulder dysfunction, severely affecting joint mobility and the activities of daily living [9]. Thoracic spine and upper rib manipulative therapy improved shoulder pain and joint mobility in patients with the primary complaint of shoulder joint pain [10, 11]. The studies suggest that the ribs and the shoulder joint demonstrate synchronous interactions; however, no standard protocols to observe rib movement during shoulder motion have been established. The bone structure of the thorax, consisting of the 24 ribs, 12 thoracic vertebrae, and the sternum, highlights that there are many difficulties in defining a standard for motion analysis of the ribs, thoracic spine, and shoulder joint [12]. A costovertebral joint and a costotransverse joint are present between the thoracic vertebrae and the ribs, with the rib neck between these two joints acting as the axis of rib motion [13, 14]. During extension of the thoracic vertebrae, posterior rotation of the ribs and the elevation of the anterior segment are described, with this axis of motion as the center; however, the motion of the ribs during bilateral arm elevation was not revealed [15]. A recent study, which analyzed the correlation between rib motion and the variation of thoracoabdominal volumes during breathing in swimmers, indicated that the angle of rib rotation was largest at the fifth rib, and this strongly corresponds with our investigation [16].
The maximum movement of the fifth rib may relate to the anatomy of the bone structure and muscles attaching to the ribs. A normal human subject study demonstrated the maximum segmental extension angle is not between the fourth and fifth thoracic vertebrae, but between first and second ribs [17]. The fifth rib, forming an articulation to the superior costal facet of the fourth thoracic vertebra and the inferior costal facet of the fifth thoracic vertebra, would provide the largest amount of motion in comparison to that of other ribs. Additionally, Holcombe et al. found that the shorter ribs showed greater stiffness than the longer ribs, and that the fifth rib was the least stiff [18]. This evidence coincides with our result. With the fifth rib as the boundary, the pectoral minor muscles (attached to the 3rd, 4th and 5th ribs) on the cranial side, the rectus abdominis muscles (attached to the 5th, 6th and 7th ribs) and the external obliques (attached to the 5th through to the 12th ribs) on the caudal side are attached, and force acts on a vector in the opposite direction with the fifth rib as the center [19]. Therefore, as these groups of muscles cause spasms or contract, the mobility of the middle thoracic vertebrae decreases via a decrease in rib motion [8]. We should pay attention to the fifth rib and thoracic vertebrae in the evaluation of thorax movement and during the treatment of shoulder disorders.
In this study, movements of the second to the fourth rib was significantly decreased in the middle-aged male group compared the young male group. The natural aging process affects all elements of the trunk including the thoracic spine, ribs, scapula, spinal inclination (the degree of forward positioning of the trunk), and trunk movement [5, 20]. Total movement of the trunk and thoracic spine, extensor muscle strength, and spinal inclination decrease, while the thoracic kyphosis angle increases with age [20, 21]. Lower mobility of the trunk may relate to less rib motion in the older age group. In the current study, the loss of thoracic vertebra extension movement does not result in a lower amount of rib motion due to aging, because the extension angle of the thoracic spine is not significantly different between the groups in their 20s and in their 50s. The mean range of thoracic spine extension is measured as 12º in end-range of bilateral shoulder elevation, on the contrary, the angle is approximately 4° in our study [1, 22]. The different measurement method and the standing or supine position can explain the lower extension range in the current study; the thoracic spine on the standing position greatly extends when compared with the supine position during bilateral arm elevation. The effect of age on structural properties of rib bone and costal cartilage also negatively influence rib motion and the mobility of the thorax. The thickness of the cortical bone in the ribs tends to decrease with age, decreasing the cross-sectional area of the rib cortical bone after the age of 25 [23]. The costal cartilage often undergoes progressive calcification with age, which has a substantial effect on the stiffness of the costal cartilage [24]. Increasing stiffness of the costal cartilage can consequently increase overall stiffness of the thorax, in which ribs provide stability to the thoracic spine. Thus, rib stiffness and lower mobility of the thorax relating to age may result in shoulder pain or shoulder disorders.
Considering the development and treatment of shoulder disorders, the largest mobility of the fifth rib and reduced mobility of the ribs relating age and/or gender are valuable information for clinical practice. Unknown pathophysiology of frozen shoulder or rotator cuff tears that are more susceptible over 50 years of age appears to correlate with a loss of motion in the shoulder joint and the trunk that also develops over 50 years old [5]. Many clinicians who have treated shoulder disorders occasionally observe a kyphosis or slouched posture, corresponding to a reduction in mobility of the thoracic spine, especially during its extension movements [25]. In an asymptomatic population, the biomechanical effects of reduced mobility in the thoracic spine revealed a strong relationship between the range of arm elevation and the range of thoracic spine extension [26]. In clinical practice, Bergman et al. assessed the benefits of applying cervicothoracic and rib manipulation and mobilization to a standardized treatment regimen for patients with shoulder pain and dysfunction. The additional manipulative therapy to usual medical care resulted in a significant improvement in the short- and long-term recovery rates and the symptom severity for these subjects [27]. Patients who underwent a single session of manipulation for the thoracic vertebrae and the upper ribs, and who had restricted range of motion of the shoulder joints and had positive impingement signs, showed improved flexion and abduction angles by 38°, the rotatable range by 30°, and the visual analog scale by 51% [28]. These studies indicate the importance of physical therapy involving the thorax in the treatment of the shoulder disorders. From the current findings, we would be effective to provide manual therapy in order to preserve the rib and thoracic spine motion to patients with shoulder disorders.
There are several limitations in this study. First, the 3-D CT imaging of the thorax was taken in the supine position, but we raise bilateral arms in the standing position. Rib kinematics recorded in this study may differ from those during bilateral arm elevation in the standing position. Secondly, we analyzed the rib movement as motion of the distal end of rib bone; however, all ribs 3-dimensionally elevate, retract, and posteriorly rotate during arm elevation. Therefore, our ribs kinematics do not provide complete ribs kinematics. Further, recent 3-D motion analysis of arm elevation and scapular motion using an electromagnetic device indicates good reliability and validity, while our arm and ribs motion were completed using 2-demensional analysis. And finally, a motion analysis protocol for evaluating the synchronized movement between the ribs, scapula, and the humeral head has not been determined. An appropriate biomechanical system for an accurate analysis will be necessary to identify the evidence concerning the ribs movement, the shoulder joint movement, and the pathophysiology of shoulder disorders.
CONCLUSION
The movement of the ribs and thoracic vertebrae during bilateral arm elevation in healthy individuals was evaluated. The largest movement distance was observed at the fifth rib and the ribs located farther away from the fifth rib, the smaller the rib movement distance. Ageing and gender influenced the amount of rib movement; movement of the upper ribs in the middle-aged males was smaller than those in the young group and mobility of the first to ninth ribs was less in females than in males. No significant difference in the extension angle of the thoracic vertebrae was found between the four groups. The findings of this study show that physical therapy applied to the thoracic spine and the upper ribs is important in the treatment of shoulder disorders.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The research was reviewed and approved by the Ethics Committee of Okubo Hospital.
HUMAN AND ANIMAL RIGHTS
All the procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with Helsinki declaration.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all participants.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Not applicable.

