All published articles of this journal are available on ScienceDirect.

Effectiveness of Surgical versus Conservative Treatment for Distal Femoral Growth Plate Fractures: A Systematic Review
Abstract
Background and Objective:
The objective of this review was to determine whether surgery, in comparison to conservative treatment, is a safe and effective intervention for the management of distal femoral growth plate fractures.
Methods:
A systematic literature review was performed using a three-step search strategy. The PubMed, Embase and Scopus databases were utilized to identify current studies from 1 January 1990 to 8 January 2017. Papers selected for retrieval were assessed by two independent reviewers for methodological validity prior to inclusion in the review using standardized critical appraisal instruments. Primary outcomes of interest were rates of growth arrest and angular deformity.
Results:
Of the 7740 studies identified with the search, 15 case studies with data inclusive of outcomes of interest were selected for inclusion. A total of 466 patients were included.
The rate of complication in the surgical population was 37.8%. In the conservative population the rate of complication was 34.0%. Five of the 15 papers showed Salter-Harris (SH) classification to correlate with prognosis, three papers showed the presence of displacement to correlate with prognosis which would have had an influence on the results of these higher graded injuries likely to have been managed operatively. A high rate of position loss and subsequent growth abnormalities was observed when conservative management was instituted.
Conclusion:
The rate of complication was marginally higher in the surgical population than that in the conservative population. This study also identified that higher severity distal femur physeal fractures, determined by the amount of displacement and Salter Harris grade, may associate a poorer outcome. It appears that managing higher severity distal femoral physeal injuries conservatively would be less likely to achieve and maintain reduction and therefore associate higher risks of malunion with subsequent growth arrest, leg length discrepancy and angular deformity as compared with surgical intervention. Further studies with higher patient numbers and comparable cohorts are needed to compare surgical and conservative interventions for the lower severity distal femoral physeal fractures.
1. INTRODUCTION
The physis of the distal femur is inherently weaker than the ligaments of the knee. Therefore, if an injuring force is applied to this area, a physeal fracture will more readily be produced rather than a disruption to the surrounding ligaments of the knee [1, 2]. A fracture to the distal femoral epiphyseal plate injury is frequently the result of high-energy forces. Common mechanisms of injury include motor vehicle accidents (including pedestrians and cyclists), sports-related injuries and falls [3-5].
A distal femoral physeal injury in children is fraught with numerous potential complications [4, 6-9]. Complete or partial growth arrest is commonly seen, which may manifest clinically in leg length discrepancy and angulation deformity [9]. Additionally, limitation on knee motion, quadriceps atrophy, osteomyelitis or osteoarthritis may result from this injury [9-11]. A meta-analysis by Basener [23] studying distal femoral physeal fractures reported an incidence of 52% in growth disturbance, with 22% of the growth disturbance greater than 1.5cm. Arkader et al. [22], similarly reported a complication rate of 40% following distal femoral physeal fracture with growth arrest being the most common
In treating distal femoral physeal fractures, surgery is thought to have less risk of re-displacement of the facture, yet this treatment modality is not without risks [12]. Potential surgical complications include osteomyelitis, injury of surrounding structures including vascular injury, nerve injury and growth plate injury [3, 9, 12]. For conservative treatment, complications relate to re-displacement of the fracture [5].
Previously published case studies show a degree of inconsistency in implementing surgical and conservative treatments for similar fractures and presentations. Generally, current practice for distal femoral physeal fractures is for non-displaced SH I fractures to be managed conservatively in a full-length leg cast or hip spica. If displacement does exist, closed manipulation with a cast may be used. Internal fixation involving K wires or pinning through the epiphysis offers another option for this fracture type. Non-displaced SH II fractures may be managed non-surgically but must be monitored closely for loss of reduction. Displaced SH II as well as SH III and IV have been managed surgically, although exact methods of surgical approach and devices vary [4, 6, 7, 11, 13].
In a search of available literature, no systematic literature review was located evaluating the most effective treatment methods for distal femoral physeal fractures. The purpose of this review was to use available evidence to identify the best treatment for these injuries.
2. MATERIALS AND METHODS
A three-step search strategy was utilized in this review to identify both published and unpublished studies from 1 January 1990 until 8 January 2017. An initial limited search of PubMed, Embase and Scopus was undertaken followed by an analysis of the text words contained in the title and abstract, and of the index terms used to describe the article. A second search using all identified keywords and index terms was then undertaken across all included databases. Thirdly, the reference list of all identified reports and articles was searched for additional studies. Studies were considered from any country with the article available in English. Studies published from 1990 onwards were considered for inclusion in this review to ensure comparable and up to date treatment modalities.
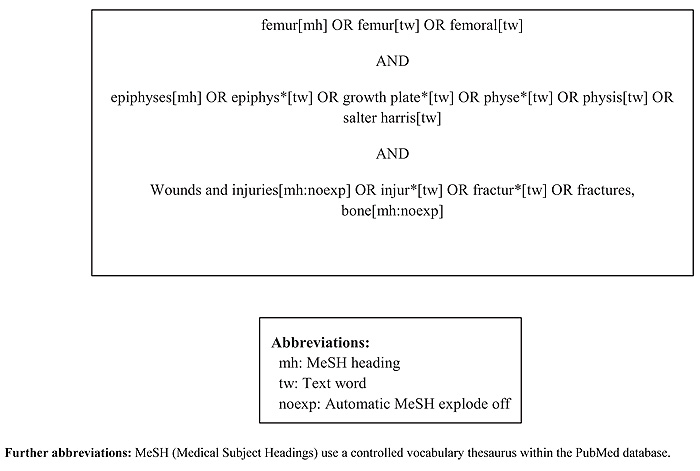
An initial search strategy was developed for the PubMed database (Appendix I). It was then minimally modified to apply to the other selected databases. The databases searched included: PubMed, Embase and Scopus. Grey literature was searched through the Scirus database. Papers that met inclusion criteria presented at conferences or meetings hosted by state or national orthopaedic associations were also considered for inclusion.
This review considered studies that evaluated surgical and conservative treatments for distal femoral growth plate fractures in the acute hospital setting. Surgery was defined as a treatment either by incision or physical manipulation with hardware fixation by a surgical doctor in a surgical theatre, for example, open reduction internal fixation. In contrast, conservative treatment was defined as any treatment for a distal femoral physeal fracture not involving hardware fixation such as closed reduction and application of a splint.
This review considered studies that included the following outcome measures:
- Rate of growth of the distal femur with different treatment strategies determined by the presence or absence of Harris growth arrest lines on X-ray or measured by absolute or relative leg length discrepancy.
- Angular or rotational deformity, measured radiographically in accordance with the appropriate technique described by Dror Paley [14].
- Secondary outcomes: return of function, pain levels, non-union, complications of surgery and length of hospital admission
Full texts of potentially relevant studies were retrieved and further assessed against the review inclusion criteria to determine final eligibility. Eligible studies were assessed for methodological validity by two independent reviewers. Reviewers discussed any differences and discrepancies upon completion of their independent review. Following discussion, there were no outstanding disagreements between the reviewers and as such discussion with a third reviewer was not required.
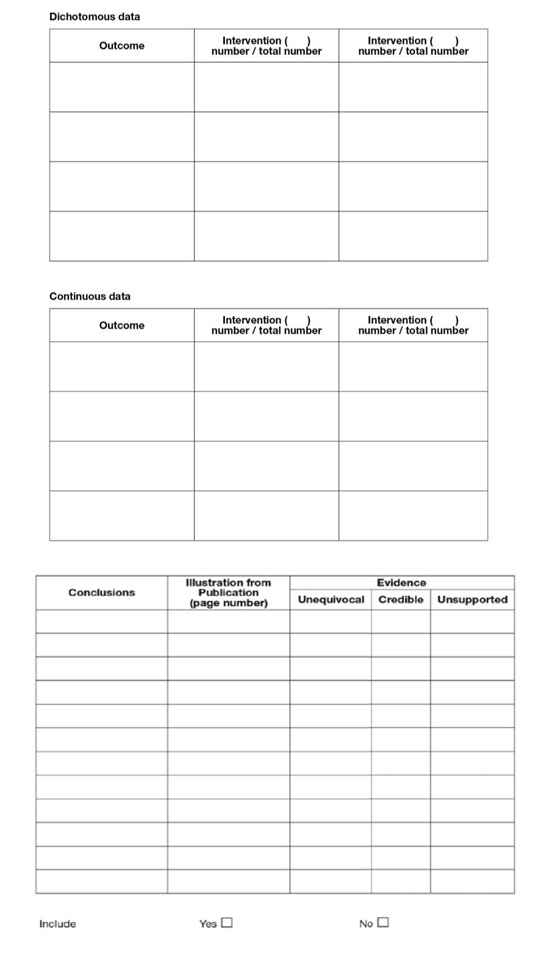
Data were extracted from the studies and integrated into a standardised data extraction proforma, modelled on the Joanna Briggs Institute quantitative data extraction tool from JBI-MAStARI (Appendix II). This provided a structure for comparisons to be made between studies.
The data extracted included inclusion and exclusion criteria and patient factors such as age, sex and mechanism of injury. Where possible, individual patient data were extracted. Injury factors such as SH classification, grading of displacement, associated primary injuries including vascular injury, nerve injury, compartment syndrome and other bony injuries were considered. Treatments provided were recorded. Outcomes evaluated included normal growth, function or complications such as growth arrest, post-surgical infection, loss of reduction and patient limitations. The type of statistical analysis used was recorded, where described.
The methods were detailed in an a priori protocol, published in the Joanna Briggs Institute Database of Systematic Reviews and Implementation Reports [15]. Despite this, there were insufficient studies with comparable patient characteristics and outcome measures to pool data for individual SH distal femoral physeal fractures. It was therefore not possible to perform meta-analysis on this dataset. Instead, a narrative synthesis accompanied by tabular presentation of the results was performed.
3. RESULTS
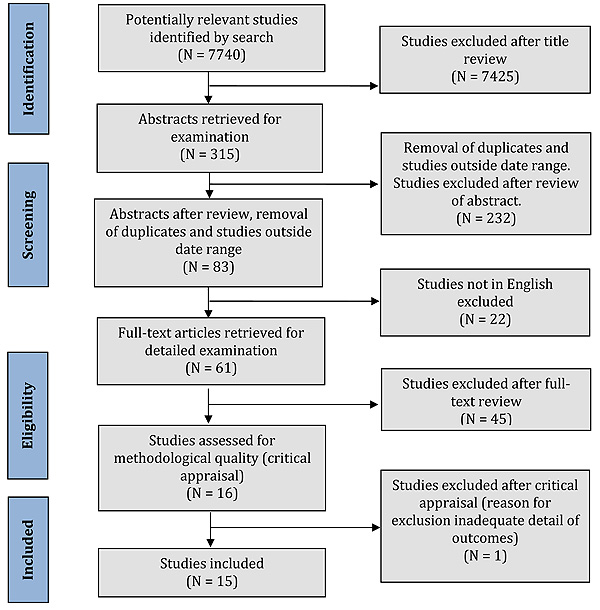
From the search of databases and for grey literature, 7740 studies were identified. From these, 7425 were omitted after review of the title. There were 315 abstracts reviewed to determine eligibility. After review of the abstracts, removing duplicates, studies outside the date criteria, or not in English, 61 studies remained. After review of these full text articles, 45 studies were excluded as they did not satisfactorily meet the inclusion criteria. Sixteen case series studies were appraised, of which one study was excluded at this stage as there was inadequate detail of primary outcomes [16]. The process of study identification, selection and inclusion is illustrated in (Fig. 1).
All 15 studies were retrospective case series with patient numbers of between six and 151 patients. All were Level 4 evidence, according to the JBI Levels of Evidence [17]. There were no higher-level evidence papers identified by the search. Although typically containing a small number of subjects, this study design allowed moderately detailed descriptions of the subjects, injuries and outcomes.
Patients were followed up between two months to 19 years post injury but follow-up durations also included until skeletal maturity or the conclusion of growth [18].
Overall, from the 15 included studies, 466 patients were evaluated. Patients ranged in age, from 0 to 18 years. The majority of patients were male (213 males, 64 females). Exact participant demographics could not be determined as not all studies listed their patients’ sex, others included data from other physeal fractures, and also patients lost to follow-up were not accounted for in the demographic data.
The injuries studied were generally due to high-energy mechanisms of injury and were of low incidence within tertiary paediatric hospitals. The most common mechanisms of injury included motor vehicle accidents, motor cycle accidents, sport related accidents including American Football, bicycle injuries, winter sports such as skiing and crush injuries. Two obstetric injuries were also included.
There were 70 cases of SH I, 276 of SHII, 58 of SHIII, 45 of SH IV, three of SHV and eight of SHVI injuries (Appendix III). Ten open fractures were included. Sixteen cases had neurovascular injuries on presentation. This included 12 peroneal palsies and four vascular injuries.
In total, of the 466 patients, 206 were listed as being managed conservatively and the remaining 233 were managed surgically. Details of the type of intervention in studies evaluating both surgical and conservative therapies are available in Table 1. Twenty-seven patients did not have their specific treatment listed.
There appeared to be little change in treatment methods throughout the studied period, with the exception of traction which is now used less frequently in Western countries [5]. Where possible, factors which might influence the outcome of the treatment were noted.
This review set out to assess outcomes for treatments of distal femoral physeal fractures. Due to inadequate patient data, it was not possible to assess the primary outcomes (rate of growth, angular or growth deformity, and incidence of complications) for each SH type of distal femoral physeal fracture, according to the specific surgical or non-surgical treatment provided. Secondary outcomes such as the return of function, pain levels, non-union, specific complications of surgery and length of hospital stay were not provided in sufficient detail to enable assessment.
Rates of complications were not specifically reported for each follow-up frequency and duration in any of the papers. However, this was on occasion attainable when individual patient data was reported. For X-ray investigations, there did not appear to be any clear radiographic protocol for how the X-ray was taken. None of the studies described the presence of Harris growth arrest lines – the widely accepted method of radiologically diagnosing growth arrest. For leg length discrepancy, no studies differentiated between absolute or relative leg length discrepancies. The method of measuring an angular deformity was not described throughout. Length of stay in hospital and a comment on the cost and resources required to perform certain treatments were not provided.
Whilst one of the 15 papers showed that surgical intervention was associated with a better outcome than conservative means, another showed a trend towards this [3, 12]. Three other papers contradicted this, indicating that an operation would yield a worse outcome [19-21]. Given these papers had very small patient numbers and insufficient patient detail, no conclusions can be drawn to suggest a superior management strategy.
Throughout the total population of surgical and conservatively managed patients, leg length discrepancy was noted in 55 cases; there were 122 cases of angular deformity present in 122 cases and radiological evidence without clinical signs was seen in 37 patients. Growth arrest that might have had angular deformity, leg length discrepancy or both was seen 87 times.
Overall, across the 15 studies, the complication rate in the surgical population was 37.8% in comparison to 34% in the conservatively managed patients with distal femoral physeal fractures.
Of all cases reported, 15 predominantly conservatively managed cases lost reduction. In total, 34 of the cases required further corrective surgery. Five cases of significant pain were reported and infection arose in five cases of the surgically managed patients. There were 57 cases of knee limitation in range of motion, 22 cases of ligamentous laxity, and 42 cases of thigh atrophy. It is not understood at which point these outcomes were measured and what further treatment for the knee stiffness, thigh atrophy and ligamentous laxity was undertaken to make further comment on its effect on the patient.
Of the 15 papers, five showed SH classification to correlate with prognosis [3, 13, 18, 19, 22]. In contrast, only one paper highlighted a varying outcome based on displacement whilst another paper showed the injury mechanism related to the outcome [13]. Patient age was also seen by another paper to influence the result for patients [4] (Appendix IV).
Follow-up ranged from three months to 36 years. From the study by Plánka et al., that followed patients for three months only, six of their 31 patients were noted to have complications of leg length discrepancy and angular deformity [21]. This represented a complication rate of 19.3%. In contrast, Caterini et al.., that followed patients for 12 to 36 years, reported a complication rate of 71.4% [22]. Caterini et al.. also noted that some cases of growth arrest were only evident many years after initial injury [22]. Specifically, one patient’s LLD was 1 cm at nine years of age; at 15 years, this LLD had progressed to 6 cm [22].
| Study | Surgical Interventions | Conservative Interventions | Outcomes Reported | Based on Reported Outcomes, was Surgical Management Associated with Better/Worse Outcomes†? |
|---|---|---|---|---|
| Arkader A., Warner W., Horn, D., Shaw R., Wells L., 2007 [6, 19] | Closed reduction (CR) with percutaneous crossed Steinman pins Annulated screws Multiple pin fixation External fixation |
Long leg cast +/- pelvic band Posterior splint Cylinder cast |
Complications: Growth arrest, LLD, angular deformity, need for surgical correction, loss of reduction, superficial Steinman pin infection | Worse |
| Ilharreborde B., Raquillet C., Morel E., Fitoussi F., Bensahel H., Penneçot G., Mazda K., 2006 [23] | ORIF of the metaphyseal fragment by cortical screws Debridement for open fracture followed by open reduction and osteosyntheis |
Plaster cast immobilization only CR + plaster cast |
LLD, Angular deformity, limitation in ROM, epiphysiodesis, ligamentous laxity | Worse |
| Plánka L., Skvaril J., Stary D., Jochymek J., Gál P., 2008 [21] | Repositioning, transfixion by K wires or 1-2 cannulated tension screws. | Spica cast | Angulation, shortening, development of porosis, limitation in hip and knee ROM, re-dislocation, re-surgery, damage to neurovascular plexus, complete healing of epiphysiolysis | Worse |
| Eid A., Hafez M., 2002 [4] | ORIF with 2 K wires or cancellous screws which do not cross the physis | Immobilised in long leg cast CR + long leg cast CR + hip spica |
Subjective complaints, gait, lower limb deformity, range of movements in the knee, ligamentous laxity, thigh atrophy, limb length discrepancy clinically, angular deformity clinically, premature growth arrest or angular deformities on XR, limb length discrepancy on XR | Worse* |
| Garrett B., Hoffman E., Carrara H., 2011 [13] | CR + internal fixation with 2 smooth percutaneous K wires or Steinmann pins (1.8 to 3.2mm) crossing the physis ORIF with above K wires/ pins or screws |
Cast only Closed reduction |
Physeal bar formation | Worse (trend only) |
| Buess-Watson E., Exner G., Illo O., 1994 [24] | Open Reduction Internal Fixation (ORIF) CR + percutaneous pinning |
Cast immobilization CR + cast immobilization |
Asymmetric growth arrest/axis deviation, LLD, (re)operation, stability | Worse for secondary operations only |
| Caterini R., Farsetti P., d’Arrigo C., Ippolito E., 1991 [22] | ORIF with K wire + hip spica cast | None (no treatment) Bilateral hip spica cast for 8 weeks Hip spica cast |
Symptoms, physical examination findings, XR examination of complications | [Sample size too small for comparison. 1/7 patients surgically managed] |
| Lippert W., Owens R., Wall E., 2010 [25] | Closed reduction percutaneous pinning ORIF |
Cast Knee immobilizer |
LLD/ growth disturbance, ROM deficit, pain, physical limitations | No difference reported/ detected |
| Edmunds I., Nade S., 1993 [3] | Closed reduction and percutaneous fixation with wires or screws Closed reduction and traction Open reduction and internal fixation (fixation with K wires, AO screws, Herbert screws) |
Robert Jones bandage only Plaster of Paris only Closed reduction and Robert Jones Closed reduction and cast |
LLD, angular deformity, limitation in ROM, osteomyelitis, lost position, further treatment required | Better |
| Thomson J., Stricker S., Williams M., 1995 [12] | Reduction, internal fixation with screw or pin | CR in Emergency Room or theatre | LLD, malalignment, loss of ROM, loss of reduction, further bony surgery | Better (trend only) |
4. DISCUSSION
With a range of treatment strategies, the rate of complication in the surgical population was 37.8%. In the conservative population, the rate of complication was marginally lower at 34.0%. A reason that the complication rate was higher in the surgical group could be that a higher energy mechanism of injury would distribute a more violent force and disruption to the growth plate, resulting in fracture displacement. Displaced fractures are more commonly treated by open reduction as a closed reduction would be less successful in placing the fragments back in their original position. A systematic review by Basener et al.. found that displaced fractures were associated with a four-fold higher risk of growth arrest than non-displaced fractures [7].
Another factor contributing to the poorer prognosis of surgically managed patients could be the SH classification of the fracture. As noted in Section 3.4, five of 15 papers showed that SH classification was correlated with prognosis, again potentially impacting the results if not factored in. An example of the reasoning is that a conservatively managed SH I injury is likely to have an improved outcome in comparison to a surgically managed SH V injury and should not be compared. This is in line with the literature for SH I injuries which also suggests that SH I injuries have a low complication rate [29].
The higher complication rate with longer follow up observed suggests the importance of long term follow-up until skeletal maturity to ensure complications are detected and therefore able to be addressed. The review did not, however, identify sufficient data for comparisons of follow-up frequency to be made.
One study demonstrated that the presence of displacement, not direction, as well as the SH classification, did influence the patient’s outcome in terms of growth or angular deformity [6]. They also demonstrated a trend, without statistical significance, that Steinmann pins across the physis led to double the number of complications compared to a physeal sparing approach. However, in 2011 another study showed that smooth pins across the physis were not statistically associated with physeal bar formation [13].
The largest number of Type VI physeal injuries in the literature was included in this review [26]. Of their eight minimally displaced distal femoral physeal fractures, the focus was on conservative management with minimal issues noted. In contrast, a different study with varying types of growth plate fractures, demonstrated a 75% complication rate in four patients managed with a closed reduction in an emergency department [12].
With respect to imaging modalities, one study demonstrated that X-ray, in comparison to higher order imaging such as Computed Tomography (CT) or MRI, significantly underestimated the displacement of a fracture [25]. Magnetic resonance imaging is advantageous in also detecting ligamentous, soft tissue injuries and early bar formation [25, 29, 30, 31].
From this review, due to the lack of quantitative evidence, it appears that the best management of fractures of the distal femoral physis is based on the following principles, supported by expert opinion.
Patients with tenderness over the distal femoral growth plate and are unable to weight bear should be treated as an undisplaced SH I injury with a full leg cast for four weeks, a grade B recommendation according to the Joanna Briggs Grades of Recommendations (79). Magnetic resonance imaging is required for confirmation. If the child is obese or has a muscular thigh, a hip spica cast may provide improved stability across the fracture site [4]. The risk of joint stiffness is less of an issue in the paediatric population.
Children with a displaced SH I fracture should be managed with a gentle closed reduction and cast in theatre with image intensifier validation of adequate joint reduction, a grade B recommendation [12]. These fractures are more stable than SH II and over, thus they may not need any fixation. If there is concern about re-displacement, retrograde crossed physeal wires are suggested. These ‘pins’ are associated with a low risk of growth arrest and may be supplemented with a cast [13].
Undisplaced SH II fractures may be managed in a cast with repeat X-ray in one week (grade B recommendation) (79). At one week, if displacement exists, options include closed reduction and K wires or open reduction internal fixation (grade B recommendation) (79). If the displacement is detected beyond a week after the injury, mild displacement is better left to remodel.
For displaced SH II fractures, reduction and K wires are sufficient if it is a small metaphyseal fragment. For larger metaphyseal fragments, one to two cannulated screws may be used, supplemented by a long leg cast (grade B recommendations) (79).
Salter Harris III and IV fractures should all be managed surgically with fixation to prevent displacement from their inherent instability, a grade B recommendation. Higher order imaging is suggested to better appreciate displacement and articular step, and for pre-operative planning [25]. For screw placement, a ‘safe triangle’ exists between the physis, the roof of the intercondylar notch (Blumensaat’s line) and the trochlear groove [25].
Salter Harris V fractures are difficult to detect and in the largest case series, all six of the SH V fractures were initially missed [4]. These have also been labelled as Peterson Type 6 injuries (14). One must therefore have a high index of suspicion with these injuries and obtain higher order imaging such as CT or MRI for further evaluation. It is suggested that these injuries are managed with initial surgical debridement before a physeal bar is to be expected (grade B recommendation) [14] (79). The management is then directed at addressing of the angular and leg length discrepancy in the medium term.
The study by Havranek, the largest SH VI cohort published, suggested that for minimally displaced SH VI injuries of the distal femur, patients faired adequately with immobilisation in a plaster cast [26].
CONCLUSION
It appears that more severe fractures, determined by the amount of displacement and Salter Harris grade, are associated with a less favourable outcome. This review did not identify any comparative studies that deviate from standard practice and manage the more severe distal femoral physeal injuries conservatively. It appears that managing higher severity distal femoral physeal injuries conservatively would be less likely to achieve and maintain reduction and therefore associate higher risks of malunion with subsequent growth arrest, leg length discrepancy and angular deformity, as compared with surgical intervention. Further studies with higher patient numbers and comparable cohorts are needed to compare surgical and conservative interventions for the lower severity distal femoral physeal fractures.
The diversity of paediatric injuries and clinician training suggests that each case must be assessed and treated on an individual basis with available resources in mind.
LIST OF ABBREVIATIONS
| PRISMA | = Preferred Reporting Items for Systematic Reviews and Meta-Analysis |
| † | = Based on descriptive studies only |
| CR | = Closed Reduction |
| ORIF | = Open Reduction Internal Fixation; |
| LLD | = Leg Length Discrepancy |
| ROM | = (Knee) Range Of Motion |
| K wire | = Kirschner wire |
| AO screws | = Arbeitsgemeinschaft für Osteosynthesefragen screws |
| No | = Number |
| mh | = MeSH heading |
| tw | = Text word |
| noexp | = Automatic MeSH explode off |
| MeSH | = Medical Subject Headings |
| Avg | = Average |
| F/u | = Follow-up |
| MVA | = Motor Vehicle Accident. |
| - | = Association between factor and patient outcome not investigated by paper |
| Y | = Association between factor and patient outcome found |
| N | = Association between factor and patient outcome not found |
| T | = Trend only, not statistically significant |
| a | = Presence, not direction of displacement |
| b | = Worsening prognosis from SH I, III, IV, II, V. |
STANDARDS OF REPORTING
PRISMA guidelines and methodology were followed.
CONSENT FOR PUBLICATION
Not applicable.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors would like to acknowledge Associate Professor Eduardo Aromataris and Dr Catalin Tufanaru for their expert advice and suggestions regarding inclusion criteria, outcome measures and in the refinement of this research. Further acknowledgement is extended to Maureen Bell for her input and feedback regarding the search strategy.
APPENDIX

| Study | |
| Year published | |
| Country | |
| Institution | |
| Years studied | |
| How patients selected | |
| Methods | |
| No. of patients initially | |
| No. of patients studied | |
| Sex | |
| Age range | |
| Average age at injury | |
| Aetiology of injuries | |
| SH I | |
| SH II | |
| SH III | |
| SH IV | |
| SH V | |
| SH VI | |
| Open fractures | |
| Neurovascular injuries | |
| Grading of displacement | |
| Conservative treatments: | |
| Surgical treatments | |
| Follow-up | |
| Outcomes measured | |
| Grading of complications | |
| Statistical analysis | |
| Results | |
| Further notes/ Classifications |
| Study | SH I | SH II | SH III | SH IV | SH V | Type VI | Males | Females | Total no. of Patients | Aetiology of Injuries | Age Range | Avg. Age at Injury |
F/u Range (avg. f/u) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Arkader A., Warner W., Horn, D., Shaw R., Wells L., 2007(21) | 18 | 43 | 4 | 7 | 1 | 0 | 67a | 16a | 73 | MVA including pedestrian vs. motor vehicle Sports related (most common American Football) |
0.41 to 17 years | 10 years | 1.5 to 7 years (2 years) |
| Buess-Watson E., Exner G., Illo O., 1994(48) | 1 | 9 | 4 | 0 | 0 | 0 | 28b | 15b | 14 | High energy trauma at winter-sports Bicycle Athletics/pedestrian/fall |
6.25 to 14.75 years | 11.75 years | - (13 years) |
| Caterini R., Farsetti P., d’Arrigo C., Ippolito E., 1991(49) | 1 | 4 | 0 | 2 | 0 | 0 | 5 | 2 | 7 | 2/7 obstetric injuries, otherwise not mentioned | Birth to 14.5 years | 8.77 years | 12.08 to 36.67 years (22.69 years) |
| Edmunds I., Nade S., 1993(15) | 0 | 16 | 4 | 2 | 1 | 0 | 23a | 10a | 23 | Motor vehicle vs. pedestrian or cyclist Fall Motorcycle accident Motor vehicle accident Sporting accident |
4 to18 years | 12 years | ‘1 year minimum’ (4.8 years) |
| Eid A., Hafez M., 2002 (16) | 39 | 65 | 19 | 22 | 6 | 0 | 129 | 22 | 151 | Sports-related activities Road traffic accidents Various falls |
0.83 to 16 years | 12.3 years | 2 to 19 years (not provided) |
| Garrett B., Hoffman E., Carrara H., 2011(29) | 4 | 46 | 2 | 3 | 0 | 0 | - | - | 40 | Motor vehicle accident, including those involving a pedestrian or cyclist Crush injuries Falls Sports-related |
- | 10 years (median) | 2 years until skeletal maturity (not provided) |
| Graham J., Gross R., 1990(17) | 2 | 7 | 0 | 1 | 0 | 0 | 9 | 1 | 10 | (American) Football Other sports Auto-pedestrian accident |
Nil provided | 13 years | - (not provided) |
| Havranek P., Pesl T., 2010(36) | 0 | 0 | 0 | 0 | 0 | 8 | 21b | 15b | 8 | All Type VI bony injuries of body: Athletic sports, Soccer, Gymnastics Stumbling/ fall from height Traffic injuries Gunshot wounds |
4 to16 years | 11.6 years (median) | 2 to 4 years (not provided) |
| Ilharreborde B., Raquillet C., Morel E., Fitoussi F., Bensahel H., Penneçot G., Mazda K., 2006(50) | 0 | 20 | 0 | 0 | 0 | 0 | 16 | 4 | 20 | MVA versus pedestrian or cyclist Sports related (ski, soccer, judo) Fall |
8 to 15 years | 11 years | 0.25 to 11 years (4.08 years) |
| Kritsaneepaiboon S., Shah R., Murray M., Kleinman P., 2009(51) | 0 | 6 | 0 | 0 | 0 | 0 | 6 | 0 | 6 | Hyper-extension injury Direct injury to the knee |
8 to 16 years | 12.5 years | 0.15 to 1.5 years (not provided) |
| Krueger-Franke M., Siebert C., Pfoerringer W., 1992(52) | 2 | 4 | 2 | 2 | 0 | 0 | 60b | 25b | 10 | Soccer Skiing Gymnastics Other |
4 to 17 years | 12.3 years (male), 12.9 years (female) | ‘Conclusion of growth’ (not specifically provided) |
| Lippert W., Owens R., Wall E., 2010(53) | 0 | 0 | 14 | 0 | 0 | 0 | 2 | 12 | 14 | Fall/ fall down stairs/ from bicycle Tombstone fell on leg (American) football |
7.67 to 17.92 years | 13.87 years | 0.167 to 3.92 years (1.79 years) |
| Partio E., Tuompo P., HIrvensalo E., Böstman O., Rokkanen P., 1997(54) | 0 | 2 | 5 | 1 | 1 * | 0 | 8 | 1 | 9 | Motorbike accidents Ice hockey Fall whilst horse riding/ from bicycle |
13.42 to 16.58 years | 15.5 years | 1 to 2.83 years (1.79 years) |
| Plánka L., Skvaril J., Stary D., Jochymek J., Gál P., 2008 (28) (55) | 3 | 26 | 2 | 0 | 0 | 0 | 16 | 15 | 31 | ‘Mainly sports and traffic accidents’ | 2 to 16 years | 11.9 years | 0.25 years only |
| Thomson J., Stricker S., Williams M., 1995(19) | 0 | 24 | 2 | 4 | 0 | 0 | 22 | 7 | 29 (30 injuries) | Nil recorded | 0.5 to 15 years | 10.9 years | 1 to 8 years (3.80 years) |
| Study | Particular SH Class | Reduced or Particular Position of Fracture Displacement | Lower Energy Injury Mechanism | Patient Age at Time of Injury |
|---|---|---|---|---|
| Arkader A., Warner W., Horn, D., Shaw R., Wells L., 2007 (21) | Y | Ya | N | N |
| Buess-Watson E., Exner G., Illo O., 1994(48) | N | - | - | N |
| Caterini R., Farsetti P., d’Arrigo C., Ippolito E., 1991(49) | Y | N | - | - |
| Edmunds I., Nade S., 1993(15) | Y | - | - | - |
| Eid A., Hafez M., 2002 (16) | Nb | - | - | Y |
| Garrett B., Hoffman E., Carrara H., 2011(29) | Y | N | Y | T |
| Graham J., Gross R., 1990(17) | - | - | - | - |
| Havranek P., Pesl T., 2010(36) | - | - | - | - |
| Ilharreborde B., Raquillet C., Morel E., Fitoussi F., Bensahel H., Penneçot G., Mazda K., 2006(50) | - | Y | - | - |
| Kritsaneepaiboon S., Shah R., Murray M., Kleinman P., 2009(51) | - | - | - | - |
| Krueger-Franke M., Siebert C., Pfoerringer W., 1992(52) | Y | - | - | - |
| Lippert W., Owens R., Wall E., 2010(53) | - | - | - | - |
| Partio E., Tuompo P., HIrvensalo E., Böstman O., Rokkanen P., 1997(54) | - | - | - | - |
| Plánka L., Skvaril J., Stary D., Jochymek J., Gál P., 2008 (28) | - | - | - | - |
| Thomson J., Stricker S., Williams M., 1995(19) | N | Y | - | N |

