All published articles of this journal are available on ScienceDirect.

Post Traumatic Diffuse Neurofibroma in the Foot: An Unusual Presentation
Authors Info & Affiliations
Abstract
Background:
Neurofibromas are benign peripheral nerve sheath tumors that present as solitary or multiple lesions. They can present alone or as part of the disease process called neurofibromatosis type 1. The etiology behind solitary neurofibromas is still poorly understood, however, trauma has been proposed to be a possible cause.
Methods:
We present a rare case of a 23-year-old male, without any known medical history, who fell and injured his left foot 3 years prior to presentation. He was treated conservatively at that time and presented to Bahrain Defence Force hospital complaining of a progressive painless swelling in his left forefoot post trauma.
Results:
The patient underwent imaging studies, which misdiagnosed the lesion as a possible lymphangioma, haemangioma, or a chronic inflammatory swelling. An excisional biopsy was taken, and the pathology specimen proved the lesion to be a diffuse neurofibroma.
Conclusion:
Trauma may possibly be a predisposing factor behind the development of solitary diffuse neurofibromas in patients that are not known to have neurofibromatosis. Further studies should be conducted to prove whether or not trauma is a predisposing factor for the development of solitary neurofibromas.
1. INTRODUCTION
Neurofibromas are benign peripheral nerve sheath tumors, formed by a wide variety of cells including Schwann cells, fibroblasts, mast cells, perineural cells, or axonal processes [1]. These benign lesions are most commonly found in the face and neck, and rarely present in the foot and ankle [2]. Less than 10% of all soft tissue tumors of the foot and ankle are neurofibromas [3]. Moreover, neurofibromas can present as solitary lesions or associated with neurofibromatosis type 1, also known as Von Recklinghausen disease. Neurofibromatosis type 1, which causes the growth of various neurofibromas in the body, is caused by a mutation in the NF1 gene [4]. However, the etiology behind solitary neurofibromas is still poorly understood. Trauma has been proposed to be a possible cause in the development of these benign lesions, however, there is insufficient evidence to support this.The following is a report of a rare case of a traumatic neurofibroma in the foot.
2. CASE REPORT
A 23-year-old male, with no past medical history and no family history, presented to the Bahrain Defence Force Hospital (BDF), in Riffa, Bahrain in October 2016 complaining of a painless lump in his left foot. The lump first appeared a few weeks after a history of a local trauma 3 years prior to presentation when the patient was exercising during military training and fell on his foot. X-rays were completed at that time and showed no signs of fractures. However, the swelling was increasing progressively since the trauma. The patient previously visited local health centers on multiple occasions and was treated conservatively with anti-inflammatories and recommendations to rest the injury.
Upon presentation, examination of the foot revealed a 4 by 3 cm lump in the dorsolateral and distal aspect of the left forefoot. The lump had an ill-defined border and was soft in consistency. It was minimally fluctuant and mobile, non-tender, irreducible, and did not trans illuminate. The skin was intact around the lesion, and the normal temperature was noted. There was a loss of extension of the left 5th toe, but normal sensation over the area of the lesion and the rest of the foot. There were no café au lait spots on the patients’ body, and no inguinal or axillary freckles. A neurologic physical exam was undertaken and showed no abnormalities. An x-ray of the foot was taken with no obvious bone changes noted. An ultrasound was conducted which showed a poorly defined swelling with a non-homogenous echo pattern and few areas of vascularity within. An MRI was also taken and showed a 50 by 35 by 25 mm lump around the 5th metatarsal and in between the interspace of the 4th and 5th metatarsal, with intense homogeneous enhancement post contrast and normal bone marrow signal intensity. The differential diagnoses at that time were a chronic inflammatory swelling, haemangioma, or lymphangioma.
The patient underwent an excisional biopsy on December 2017, as a day case procedure. Intra operatively, a white swelling was found over the dorsum and lateral aspect of the left forefoot, in the interspace between the 4th and 5th metatarsal, extending to the plantar aspect of the foot, and wrapped around the lateral dorsal cutaneous nerve. The fifth toe extensor tendon was completely torn. Excision of the mass was done, with the protection of the nerve. The patient was discharged on the same day, and the stitches were removed 2 weeks later in the clinic.
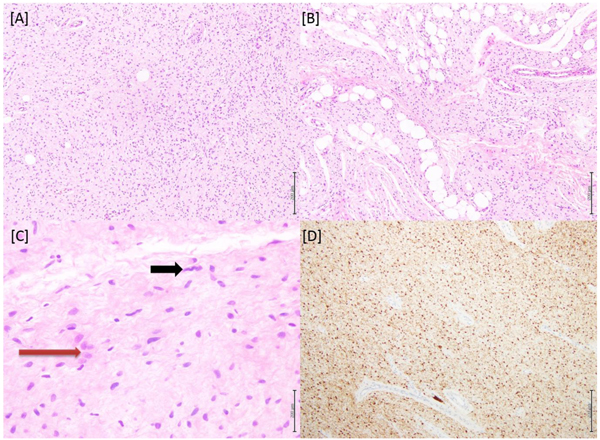
Macroscopic examination of the specimen showed a white fibrous rubbery tissue measuring 5x5x4.1 cm. Under the microscope, a benign lesion composed of diffusely arranged spindly to ovoid cells was seen, with tumor cells focally invading the included fatty tissue as seen in Fig. (1). Immunohistochemistry was done, and the tumor cells showed strong positivity to S100; but were negative to SMA, Desmin, and CD68. No atypia was noted. The tumor was present at the surgical resection margin, thus the diagnosis of an incompletely excised diffuse neurofibroma was made.
3. DISCUSSION
Neurofibromas are benign peripheral nerve tumors, formed by a wide range of cells and its processes including Schwann cells, perineural cells, and axonal processes [5]. They can occur either as sporadic lesions, such as our reported case, or part of a disease process called neurofibromatosis. Neurofibromas have been categorized into several types according to appearance, histology, and the way they present clinically. Diffuse neurofibroma is an ill-defined and infiltrative lesion, usually nondestructive, rarely undergoes malignant change and is most commonly found in the head and neck region. On histopathology, it is composed of spindle-shaped and ovoid cells with occasional Meissner bodies, and is S100 immunoreactive [6].
Although histology aids in diagnosis, it still remains difficult to correctly identify a neurofibroma clinically. Physical examination of the lesion may misidentify it as a schwannoma, traumatic neuroma, lymphangioma, or haemangioma such as in our presented case. Other differential diagnoses include lipomatosis and fibromatoses [7]. Although they may present similarly, a traumatic neuroma on histology will present with complex micro fascicles of axons, while the axons of a neurofibroma are usually dispersed [8].
It is important to correctly identify a neurofibroma prior to definitive treatment, as a misdiagnosis such as in our case may lead to an incomplete cure. If it was known that the lesion in our patient was a neurofibroma, a more exploratory approach would have been undertaken with different excision margins. It is also important to note that neurofibromas make up less than 10% of foot and ankle soft tissue tumors [3]. This made the diagnosis of a neurofibroma in our patient more difficult to ascertain. Our patient was sent abroad to a specialist center to completely resect the rest of the neurofibroma. On 3 month follow up, the patient was doing well and did not complain of any symptoms. The wound healed, and no swelling was noted at the incision site.
Although neurofibromatosis is a known cause of neurofibromas, the cause of solitary neurofibromas is still unknown. Rare cases of traumatic neurofibromas have been reported in the literature, but it is still unclear if trauma is a predisposing factor in the development of this benign tumor. Carpenter and Stickney reported a similar case to ours of a traumatic neurofibroma in the leg of a 38-year-old female patient that sustained a traumatic injury 5 years prior to presentation [2]. In addition, Choi et al., reported a rare traumatic solitary neurofibroma in the finger. It was excised completely and the patient did well postoperatively [9]. This lesion could have easily been confused with other more common finger lesions. Likewise, Da Rosa et al., reported a mental nerve solitary giant neurofibroma that was related to trauma [10]. Similarly, Chi et al., reported a facial neurofibroma after history of trauma to the cheek [11].
In addition, it is clear that cases of traumatic neurofibromas can be misdiagnosed. D’Orazi et al., reported a case of neurofibroma that was initially misdiagnosed as a recurrent Mortons neuroma [12]. Similarly, Shah et al., reported a misdiagnosed neurofibroma that presented as a vascular hamartoma after a traumatic iatrogenic intramuscular injection in the shoulder. However, trauma was not proven to be the etiological factor because the patient also had another neurofibroma in the flank [13].
CONCLUSION
Our patient presented with a progressively enlarging mass in the foot that started after a clear traumatic event. Although it is still unknown if trauma is a precipitating factor behind the development of neurofibromas, a few rare cases have been reported in the literature that associate trauma with these benign tumors. Knowing the causes and pathophysiology behind solitary neurofibromas will help in the proper diagnosis of such lesions. This should be done prior to definitive treatment, as a misdiagnosis may lead to further morbidity.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Verbal consent was taken from the patient prior to the publication of this article.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
We would like to thank Prof Khalid Alkhalifa for his continuous support for research at the BDF hospital in Bahrain. We would also like to thank Dr. Abdulla Darwish and Dr. Veena Nagaraj for reporting the pathology specimens.

