All published articles of this journal are available on ScienceDirect.

Characteristic MRI Findings of Epidermal Cysts Categorized by Size
Abstract
Background:
Epidermal cysts are lined with stratified squamous epithelium and filled with keratinous material.Magnetic resonance imaging (MRI) findings can be used for the diagnosis of epidermal cysts, but characteristic MRI findings related to cyst size in particular go unreported.
Objective:
To analyse characteristic MRI findings of epidermal cysts categorized by size.
Materials and Methods:
Unruptured epidermal cyst cases were analyzed according to 3 cyst size categories: large (≥4 cm), medium (≥2 to <4 cm), and small (<2 cm). MRI assessments focused on the keratinized material using low signal intensity on T2-weighted images because of intracystic diffuse foci (a sign of intracyst debris) and serpentine structures at the periphery (a sign of a peripheral lining) of cysts.
Results:
Thirty-three patients (26 males and 7 females; average age, 52.2 years; 33 cases) were grouped by cyst size: large (13 cases), medium (12 cases), and small (8 cases). MRIs revealed cyst walls via low signal intensity on T1- and T2-weighted images. On T1-weighted images, the signal intensity of cysts relative to that of muscle was hypointense (1 case, 3%), isointense (4 cases,12%), and slightly hyperintense (28 cases, 85%). On T2-weighted images, cysts were hyperintense in muscle relative to adipose tissue (20/33 cases, 61%) and isointense relative to adipose tissue (7/33, 21%) or hyperintense relative to adipose tissue (6/33, 18%). Overall, signal patterns were similar among groups. Signs of inner debris were observed in all large (13, 100%) and medium (2/12, 17%) cysts, but not in small cysts (0/8). Large, medium, and small cysts had signs of peripheral linings (12/13, 92%; 9/12, 75%; and 4/8, 50%, respectively).
Conclusion:
Slightly hyperintense signals on T1-weighted images were characteristic, even in small epidermal cysts. Signs of intracyst debris and a peripheral lining reflect the pathology and were considered useful for diagnosis. Larger cysts were more frequently positive for keratinous debris.
1. INTRODUCTION
Epidermal cysts, or epidermoid cysts, are common, benign, intradermal, or subcutaneous lesions [1, 2]. They are lined with stratified squamous epithelium and filled with keratinous debris originating from the squamous epithelium [1, 2]. Cyst pathogenesis has been proposed to be the result of a migration of epidermal cells into the dermis, aberrant embryogenesis during cellular differentiation, transplantation of epidermal cells into the dermis following trauma, or inflammation of pilosebaceous structures causing a cystic reaction [2].
Epidermal cysts are frequently asymptomatic [3] and grow via the accumulation of epithelial and keratinous debris [1, 4]. Surgical excision of the lesion is a frequent curative treatment [5]. The size of most epidermal cysts ranges from 1 to 4 cm [3]. Rarely do these cysts exceed 5 cm in diameter, but when they do they are referred to as giant epidermal cysts [1, 6-8]. Malignant transformation of epidermal cysts has been observed, although the reported frequency of a squamous cell carcinoma arising from epidermal cysts is low, ranging from 0.011 to 0.045% [9, 10].
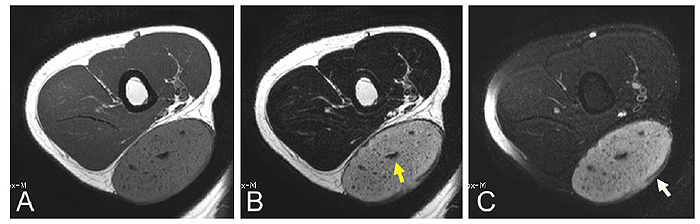
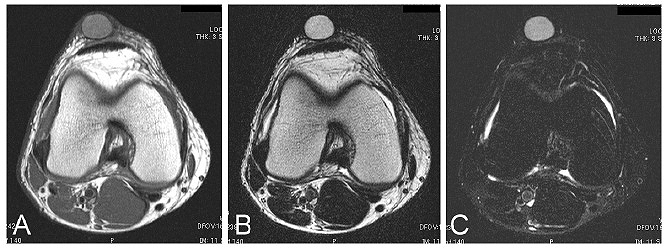

Magnetic Resonance Imaging (MRI) can reveal an epidermal cyst as a well-demarcated oval-shaped mass with a cystic wall [11]. On T1-weighted images, epidermal cysts are reported to demonstrate isointense to slightly hyperintense signals, and on T2-weighted images the signals are of intermediate to high signal intensity [11]. The variable amount of keratinous debris, that is, lower signal foci or serpentine structures, on T2-weighted images has been reported to be 43% [11] and 58% [5] Fig. (1 and 2).
The purpose of this study was to analyze the characteristic MRI findings of epidermal cysts categorized by size in the current cases.
2. MATERIALS AND METHODS
Surgically resected epidermal cysts were evaluated in our analysis. Diagnosis of epidermal cysts was histopathologically confirmed in all resected cases. Epidermal cysts with a history of rupture were excluded from this study. Using MRIs, cysts were evaluated by size and assessed using low signal intensity on T2-weighted images for keratinous materials which included intracystic diffuse foci and serpentine structures at the periphery, or signs of “intracyst debris” and “peripheral lining” respectively. Lesions were divided into 3 size categories as follows: large (≥4 cm), medium (≥2 to <4 cm), and small (<2 cm).
3. RESULTS
Clinical data are shown in Table. (1). Overall, the patients included 26 males and 7 females of mean age 52.2 ± 16.8 (range 12 to 87) years. Mean cyst size was 3.5 ± 2.1 (range 0.6 to 12) cm. Cyst locations included the shoulder (9 cases, 27%), back (5 cases, 15%), finger (5 cases, 15%), thigh (5 cases, 15%), knee (2 cases, 6%), foot (2 cases, 6%), upper arm (2 cases, 6%), and hand (1 case, 3%).The MRIs showed all cases demonstrated a well-demarcated oval-shaped mass and a cystic wall with a low signal intensity on T1- and T2-weighted images. MRI findings are shown in Tables. (2 and 3). Among the 33 cases, on the T1-weighted images, 28 cases (85%) had signals that were hyperintense for cystic content relative to muscle, 4 cases (12%) were isointense relative to muscle, and 1 case (3%) was hypointense relative to muscle. On T2-weighted images, 20 cases (61%) had signals that were hyperintense relative to muscle, 7 cases (21%) were isointense relative to adipose tissue, and 6 cases had signals that were hyperintense relative to adipose tissue (18%). Among all cases, intracyst debris was observed in 15 cases (45%), and a peripheral lining was detected in 25 cases (76%).
| Cyst Size (cm) | Cases (n) | Mean Age ± SD [range] (years) | M:F | Mean Cyst Size ± SD [range] (cm) | Location of Cysts and Cases (n) |
|---|---|---|---|---|---|
| Large (≥4) | 13 | 57.9 ± 16.5 [27 to 79] |
10:3 | 5.8 ± 2.2 [4.0 to 12] |
Buttock (6), thigh (2), knee (n=2), upper arm (1), back (1), and foot (1) |
Medium ( 2 to <4) 2 to <4) |
12 | 48.7 ± 11.6 [31 to 68] |
9:3 | 2.5 ± 0.49 [2.0 to 3.5] |
Back (3), buttock (2), foot (2), upper arm (1), nucha (1), thigh (1), knee (1), and hand (1) |
| Small (<2) | 8 | 48.0 ± 22.7 [12 to 87] |
7:1 | 1.1 ± 0.42 [0.6 to 1.5] |
Finger (5), back (1), buttock (1), and thigh (1) |
| Total | 33 | 52.2 ± 16.8 [12 to 87] |
26:7 | 3.5 ± 2.1 [0.6 to 12] |
Buttock (9), back (5), finger (5), thigh (4), knee (3), foot (3), upper arm (2), and hand (1) |
|
Case size (cm) |
MRI Signal Intensity of Cyst |
T1-WI [n (%)] |
T2-WI [n (%)] |
|---|---|---|---|
| Large (≥4) | - | 13 | 13 |
| Hypointense relative to muscle | 1 (8) | – | |
| Isointense relative to muscle | 3 (23) | – | |
| Hyperintense relative to muscle | 9 (69) | 9 (69) | |
| Isointense relative to adipose | – | 2 (15) | |
| Hyperintense relative to adipose | – | 2 (15) | |
| Middle (≥2 to <4) | - | 12 | 12 |
| Hypointense relative to muscle | – | – | |
| Isointense relative to muscle | 1 (8) | – | |
| Hyperintense relative to muscle | 11 (92) | 7 (58) | |
| Isointense relative to adipose | – | 3 (25) | |
| Hyperintense relative to adipose | – | 2 (17) | |
| Small (<2) | - | 8 | 8 |
| Hypointense relative to muscle | – | – | |
| Isointense relative to muscle | – | – | |
| Hyperintense relative to muscle | 8 (100) | 4 (50) | |
| Isointense relative to adipose | – | 2 (25) | |
| Hyperintense relative to adipose | – | 2 (25) | |
| Total | - | 33 | 33 |
| (3.5) | Hypointense relative to muscle | 1 (3) | – |
| (range, 0.6 to 12) | Isointense relative to muscle | 4 (12) | - |
| Hyperintense relative to muscle | 28 (85) | 20 (61) | |
| Isointense relative to adipose | – | 7 (21) | |
| Hyperintense relative to adipose | – | 6 (18) |
|
Case Size (cm) |
Keratinous Debris |
Intracyst Foci* <sign> [n (%)] |
Peripheral Lining* <sign> [n (%)] |
|---|---|---|---|
| Large (≥4) | - | 13 | 13 |
| - | Positive | 13 (100) | 12 (92) |
| - | Negative | 0 (0) | 1 (8) |
| Middle (≥2 to <4) | - | 12 | 12 |
| - | Positive | 2 (17) | 9 (75) |
| - | Negative | 10 (83) | 3 (25) |
| Small (<2) | - | 8 | 8 |
| - | Positive | 0 (0) | 4 (50) |
| - | Negative | 8 (100) | 4 (50) |
| Total | - | 33 | 33 |
| (3.5) | Positive | 15 (45) | 25 (76%) |
| (range, 0.6 to 12) | Negative | 18 (55) | 8 (24) |
For cases with large-size cysts, the patients included 10 males and 3 females of mean age of 57.9 ± 16.5 (range 27 to 79) years. Mean cyst size was 5.8 ± 2.2 (range 4.0 to 12) cm. Cyst locations included the buttock (6 cases), thigh, knee (2 cases each), upper arm, back, and foot (1 case each). Among these 13 cases, on T1-weighted images the signal for cysts was hyperintense relative to muscle (9 cases, 69%), isointense relative to muscle (3 cases, 23%), and hypointense relative to muscle (1 case, 8%). On T2-weighted images, the signal was hyperintense relative to muscle (9 cases, 69%), isointense relative to adipose tissue, and hyperintense relative to adipose tissue (2 cases each and 15% for both). Intracyst debris was observed in all 13 cases (100%) of large cysts. A peripheral lining was detected in 12 cases (92%).
There were 12 cases with medium-sized cysts. The patients in this category included 9 males and 3 females of mean age 48.7 ± 11.6 (range 31 to 68) years. Mean cyst size was 2.5 ± 0.49 (range 2.0 to 3.5) cm. Tumor locations were the back (3 cases), buttock, foot (2 cases each), upper arm, nucha, thigh, knee, and hand (1 case each). Among these 12 cases, on the T1-weighted images the signal for cysts was hyperintense relative to muscle (11 cases, 92%) and isointense relative to muscle (1 case, 8%). On T2-weighted images, the signal was hyperintense relative to muscle (7 cases, 58%), isointense relative to adipose tissue (3 cases, 25%), and hyperintense relative to than adipose tissue (2 cases, 17%). Intracyst debris was observed in 2 out of 12 cases (17%), and the remaining10 cases (83%) were negative for keratinous debris. A peripheral lining was detected in 9 out of 12 cases (75%), and the remaining 3 cases (25%) were negative for keratinous debris.
There were 8 cases of small-sized cysts in patients that included 7 males and 1 female of mean age 48.0 ± 22.7 (range 12 to 87) years. Mean cyst size was 1.1 ± 0.42 (range 0.6 to 1.5) cm. Cyst locations were in the finger (5 cases), as well as back, buttock, and thigh (1 case each). Among these 8 cases, on T1-weighted images the signal for cysts was hyperintense relative to muscle (100%). On T2-weighted images, the signal was hyperintense relative to muscle, but lower than adipose tissue (4 cases, 50%), isointense relative to adipose tissue and hyperintense relative to adipose tissue (each had 2 cases, 25%). Intracyst debris was not observed in any of these 8 cases, but a peripheral lining was detected (4 cases, 50%).
4. DISCUSSION
In the current cases, characteristic MRI findings of epidermal cysts by size category were analyzed. MRIs showed the epidermal cysts as well-demarcated and oval-shaped lesions in all cases. The signal intensity of the cystic wall shows low signal intensity on T1- and T2-weighted images [8], which is consistent with what was observed among all our cases. The signal intensity for the content of the cyst was intermediate to slightly increased on T1-weighted images and of high intensity on T2 -weighted images [5, 12]. On T1-weighted images, a hyperintense signal relative to muscle was a characteristic in 85% of the cases in the current series. For the same 9 cases reported previously, T2-weighted images of the lesions were of high and intermediate signal intensity 67% and 22% of the time, respectively [11]. In our series, on T2-weighted images, 61% of the cases displayed hyperintense signals relative to muscle, but hypointense signals relative to adipose tissue, such that our results appear consistent with the previous report. Overall, the variation in signal intensity was the same among the 3 different size categories for cysts even though they had different anatomical distributions; small-sized lesions were located peripherally in the fingers whereas larger-sized cysts were located more centrally in the torso, in the back or buttock for example Fig. (3).
Epidermal cysts are filled with keratinous material. The foci of keratinous debris with low signal intensity on T2-weighted images have been reported in 43% [11] and 58% of cases [5]. Heterogeneity due to the foci of keratinous debris is reported to be useful in differentiating epidermal inclusion cysts from other fluid-filled masses such as ganglion cysts with homogeneous signal intensities [5, 12]. In our case series overall, intracyst debris was observed in 45% cases. However, in cases involving cysts categorized as large, signs of intracyst debris were present in all cases. Intracyst debris reflects the pathology of epidermal cysts and represents a useful sign to observe, not only for the diagnosis of an epidermal cyst, but it would also provide information that assists in the differentiation of this type of cyst from one that is mimicking a malignancy.Furthermore, when cyst size is large enough for sampling with a needle, we propose that cytological confirmation of keratinous material would be helpful not only in making a diagnosis, but also in excluding malignancy.
The keratinous content in epidermal cyst material originates from the cyst wall and is often in a laminated arrangement. In our case series, the peripheral lining structure of the cyst has been emphasized. In a previous study, the peripheral lining structure with its low signal intensity on T2-weighted images was observed in 4 out of 9 cases (44%) [11]. In our cases in this study, a peripheral lining was observed 76% of the time. A peripheral lining was clearly evident at a high positive rate in patients with cysts in the large size category, while only half of the cases with small size cysts presented with this sign. A peripheral lining is a more reliable sign than intracyst debris when diagnosing small-sized epidermal cysts.
CONCLUSION
Epidermal cysts are subcutaneously located, well-circumscribed lesions. The slightly higher signal intensities of cysts relative to muscle on T1-weighted images are characteristic, even in small-sized lesions. Signs of intracyst debris and peripheral lining reflecting the pathology of the epithelial cysts were more characteristic of large-sized cysts. These signs are useful in the differentiation of epidermal cysts from neoplastic lesions including those that mimic a malignancy.
ABBREVIATION
| MRI | = Magnetic Resonance Imaging |
PATIENT CONSENT
All patients represented in this study were informed that the data from their case would be de-identified and used in a journal publication.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all participants.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

