All published articles of this journal are available on ScienceDirect.

An Age and Activity Algorithm for Treatment of Type II SLAP Tears
Abstract
Background:
Type II SLAP tears predominantly occur in males between their third and fifth decades of life. The mechanism of injury is often repeated overheard activity but can also occur due to direct compression loads and traction injuries. The treatment options have changed over the years and include non-operative therapy, direct labral-biceps complex repair, and labral debridement with biceps tenodesis or tenotomy.
Objective:
To review the existing literature on the management of Type II SLAP tears and provide clinical recommendations based on patient age and activity level.
Methods:
A review of the existing literature through October 2017 investigating the management of Type II SLAP tears was performed. Emphasis was placed on distinguishing the outcomes based on age and activity level to provide an appropriate treatment algorithm.
Results:
Patients with Type II SLAP tears should first be trialed with non-operative management and many patients will have a successful result with ability to return to their respective sports or activities. Surgical management should be considered if non-operative management does not provide symptomatic relief. Young, athletic, or high-demand patients should be treated with a SLAP repair while biceps tenodesis should be considered for older or worker’s compensation patients. Patients undergoing revision surgery for a failed SLAP repair should be managed with biceps tenodesis.
Conclusion:
Type II SLAP tears remain a difficult pathology to manage clinically, but the treatment indications are narrowing. The age and activity algorithm described in this review provides an effective method of managing this complex clinical condition.
1. INTRODUCTION
Tears of the Superior Labrum-Biceps Complex (SLBC) were first described by Andrews et al [1] as Superior Labrum Anterior to Posterior (SLAP) tears. Snyder et al [2] organized these SLAP tears into four major types: 1) Labral fraying with intact bicep anchor; 2) Labral fraying with detachment of bicep anchor; 3) Bucket handle tear of labrum with intact bicep anchor; and 4) Bucket handle tear of the labrum that extends into the bicep anchor. These four types of SLAP tears were later expanded by Maffet et al [3]. SLAP tears are not common injuries to the shoulder, but often result from repetitive overhead activity due to a “Peel-back Mechanism,” [4] direct compression loads, or occasionally traction injuries [5]. These lesions predominantly occur in males and are often treated in the third and fifth decades of life [6]. SLAP tears can be difficult to diagnosis as a patient’s history can be mixed, with the most common complaint of pain [5]. Overhead throwers may mention a typical history of loss of velocity or control [7]. Physical examination is also unable to diagnose SLAP tears with consistency [8-11] as most exam maneuvers may suggest but not confirm a SLAP tear. Part of the difficulty is that while SLAP tears do occur in isolation, they can also be found with concomitant pathology including rotator cuff tears, labral tears, Acromio-clavicular joint pathology, and impingement in up to 88% of cases [12, 13]. Magnetic Resonance Imaging (MRI) has been useful in identifying SLAP lesion [14] despite multiple anatomical variants [15], but MRI arthrogram remains the gold standard for imaging.
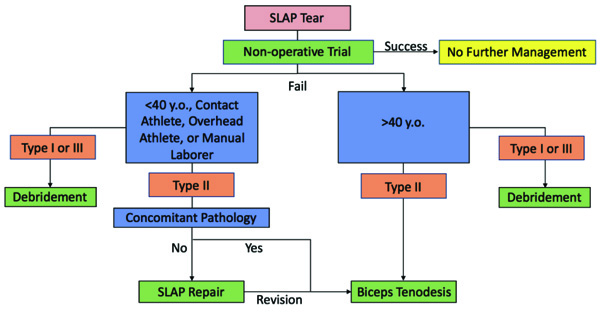
As these lesions became better defined and imaging quality improved there was an increase in diagnosis [16] and surgical treatment of slap lesions [6, 17] until the late 2000’s. However, as our understanding of the pathology, outcomes, and complications improved there has been a decreased frequency and change in approach to the surgical treatment of SLAP tears [18, 19]. Much of this change is centered upon the treatment of Type II SLAP tears. While the general consensus on the treatment of Type I and III tears centers on debridement [5, 20, 21], treatment of type II tears continues to be studied and modified. To date, numerous studies have examined treatment of type II SLAP tears [20, 22-37] including multiple systematic and database reviews [6, 16, 18, 19, 38-41]. Current treatment options for Type II SLAP tears include non-operative, direct labral-bicep complex repair, and debridement with tenodesis or tenotomy. The primary treatment in type II SLAP tears was originally direct repair, but has undergone a slow development of a treatment algorithm that is based on the patient’s age and activity level for most surgeons as reflected in the most recent ABOS board review data [19]. A database of our senior author (BJC) and his colleagues have reflected a growing use of bicep tenodesis for SLAP tears and other shoulder pathologies [42]. A recent randomized control trial out of Norway looked at outcomes between sham surgery, labral repair, and bicep tenodesis for Type II SLAP tears [36]. The authors report no significant difference between the three groups in terms of outcomes. These results need to be tempered as patients were organized as intent to treat and 14 of 39 (35.9%) of sham patients required repeat surgeries (either for repair or tenodesis), while the tenodesis group had 6 repeat surgeries (2 capsular releases, 3 labral repair, and 1 AC joint resection) and the repair group had only 4 repeat surgeries (3 bicep tenodesis and 1 AC joint resection) [36]. Schrøeder et al recognizes the influence of these cross over patients and concludes that SLAP tears may be overtreated and requires more narrowed indications in the case of repair. In that light, our paper explains the senior author’s indications and reasoning behind the treatment for each treatment group (Fig. 1).
2. NON-OPERATIVE MANAGEMENT
In most cases, all patients should first be trialed with non-operative treatment. This decision-making is in the context that incidental labral abnormalities are common by MRI, and the natural history of the neglected-labral tear is not associated with the development of other relevant pathology that can otherwise be prevented with early treatment. In other words, benign neglect is acceptable if the patient can be made to tolerate their symptoms or to become asymptomatic with normal function. Non-operative treatment has shown success in groups including high-level athletes [43-45]. Edwards et al [43] performed a retrospective review of people treated non-operatively including athletes. While the paper is limited by poor response (39 out of 371 eligible patients) their findings demonstrated 49% of patients were deemed successfully treated with posterior capsular stretching and scapular stabilization programs. Those that were successful saw significant improvements in ASES (58.5 to 84.7) and VAS (4.5 to 2.1) and all athletes were able to return to their sport. Including the failure 71% of athletes returned to their sport with non-operative treatment and 67% for overhead athletes [43]. Jang et al [45] investigated possible risk factors for people who would fail non-operative treatment. In their retrospective study of 63 patients, 71% of patients had successful non-operative treatment at 21 months. Multivariate analysis demonstrated that patients with a history of trauma (OR 9.8), positive compression test (OR 8.8), and participation in overhead activities (OR 19.1) were more likely to fail non-operative treatment [45]. Non-operative management may have even a small but less successful role in elite overhead athletes. A retrospective review of a single major league baseball organization’s players demonstrated a return to play rate of 40% for pitchers and a return to previous level of play of only 22% with non-operative treatment. Despite a high failure rate, non-operative treatment did not differ much from surgical interventions, which saw a return to play rate of 48% and a return to previous level of play of 7% [44]. Of note, positional players fared much better with operative treatment, returning to play in 85% of cases versus 39% of those treated non-operatively, and those with concomitant partial cuff tears fared worse [44]. While successful non-operative treatment ranges from 40% to 70%, it should be at least trialed in most patient populations including elite throwers especially given the heterogeneous outcome in this population following surgical intervention.
3. YOUNG, ATHLETIC PATIENTS AND OVERHEAD THROWERS
Repetitive overhead motion, especially amongst throwers is believed to be one of the primary causes of SLAP tears. The biological adaptations in muscular and ligamentous anatomy in an overhead thrower was outlined by Burkhart et al [7] including the series of events that lead to the “peel back” mechanism that predisposes throwers to SLAP tears [4]. While not clearly defined, the role of the bicep tendon has been considered a vestigial organ [46] and primarily a pain generator for a dysfunctional shoulder [47]. Cadaveric studies, however, have pointed to the superior labrum and the long head of the bicep as an important glenohumeral stabilizer [48-52], especially in overhead throwers [53]. These studies however, had varying lesion size with significant but small changes in glenohumeral motion that may not be clinically significant and do not account for additional factors for glenohumeral motion and stability [46, 54].
Despite conflicting cadaveric studies, young active patients, particularly overhead throwers, have been deemed the best candidates for repair of type II SLAP tears. Systematic reviews have demonstrated that patients who are younger athletes have better outcome scores and more reliable return to sport following SLAP repair [26, 55]. Sayde et al [55] demonstrated 83% of patients reporting good to excellent results and 73% of athletes (63% overhead athletes) returned to their previous level of play. Kim et al [32] and Ide et al [56] reported excellent outcomes in 79% and 75% of their young (<40) athletic cohorts, respectively. Studies of athletic populations have consistently shown that overhead athletes do not have the same return to sport rates as non-overhead athletes despite both groups having excellent outcomes [26, 28, 32, 55-58]. Friel et al with the senior author (BJC) [28] exemplified this with excellent functional outcome scores, but five of the thirteen overhead athletes failed to return to previous level. Similar disparities in return to sport rates were found in larger studies by Kim et al [32] and Ide et al [56]. An exception to this trend was Morgan et al [57] who reviewed 102 patients (53 overhead athletes) and found that 87% had excellent one-year post-operative outcomes based on their UCLA shoulder scores. More specifically, of the 44 pitchers, 37 (84%) of them reported excellent outcomes at one year and only seven (all had partial cuff tears) subjectively did not return to their previous level of performance [57].
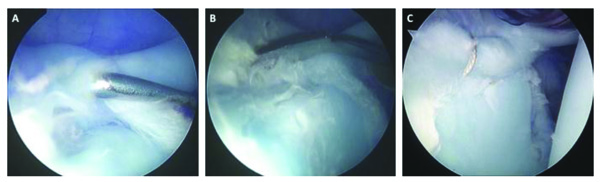
Elite level throwers are a population that has been closely studied. Baseball players, specifically pitchers, are susceptible to SLAP tears and have the lowest return to sport outcomes [58]. While overall shoulder scores improve with surgical treatment of Type II SLAP tears, the return to play outcome is significantly lower then other athletic populations [44, 59]. Smith et al [59] found that only 62.5% of Major League Baseball pitchers were able to return to the major league level, and only 54% returned to their previous level of performance. This is still an improvement compared to non-operative outcomes report by Fedoriw et al [44]. Military populations also tend to have worse outcomes then the general population. A study of 179 military patients with a mean follow up of 40 months saw significant improvement in their outcome scores, but 66 (36.8%) patients had failed SLAP repair requiring either medical discharge or revision surgery [34]. Age greater then thirty-six was the only risk factor for failure on sub group analysis. Due to the excellent outcomes, we recommend SLAP repair for most young and athletic patients who have no overlapping biceps pain and who have failed non-surgical intervention (Fig. 2). At some point, we will often utilize selective injections as a pre-operative diagnostic tool. Immediate but temporary relief with a local anesthetic injection into the glenhohumeral joint in the absence of biceps pain or provocative symptoms in the biceps with physical examination is relatively specific to labral pathology in the absence of any other identifiable pain generator.
Tenodesis in a younger athletic patient may have a limited role in treating this patient group. Bicep tenodesis has proven effective in revision SLAP tears [23, 60-62]. McCormick et al [61] reviewed 42 patients with failed SLAP repairs, following tenodesis the ASES (68 to 89), SANE (64 to 84), and WOSI (65 to 81) scores improved significantly with 81% of participants returning to active duty and sports. A smaller civilian cohort of 11 patients saw similar improvements in functional outcome scores (ASES 54.5 to 78; SANE 42.5 to 70.4) and the 3 athletes returned to their sport [62]. While no study has specifically analyzed the outcomes of primary bicep tenodesis of overhead and throwing athletes, their results have been included in cohort studies [23, 25, 29, 30, 63]. Pogorzelski et al [63] reviewed 20 patients at an average follow up of 3.4 years and found that recreation athletes do benefit from primary subpectoral biceps tenodesis with 73% return to previous level including 80% of overhead athletes. Only two of the patients were throwers and two were volleyball players. Schöffl et al [64] demonstrated that non-throwing overhead athletes rock climbers have performed well with full return to sport following primary biceps tenodesis. Outcomes of elite throwers, however, following primary or revision bicep tenodesis have not been published to date. In fact a systematic review reported that only 71% of 49 studies of outcomes in baseball throwers with shoulder and elbow injuries reported return to play and 31% reported return to previous level [65]. As outlined earlier, the concern of glenohumeral stability without an intact biceps anchor has been a major concern [52], but a recent EMG and motion analysis study reports that pitchers regain physiologic neuromuscular control and normal pitching mechanics whether treated with SLAP repair or bicep tenodesis versus controls [66]. Chalmers et al [66] found that those with SLAP repairs had significantly different thoracic rotation movements compared to those with biceps tenodesis and controls. Another cadaveric study showed that bicep tenodesis had no detrimental effect on glenohumeral stability and repair of an anterior SLAP tear was the only intervention to restore translational stability [67]. Strauss et al including our senior author (BJC) concluded that bicep tenodesis is viable option for both primary and revision cases, but should be used with caution in overhead athletes. Despite these findings, Major League Baseball team surgeons still overwhelming favor repair over debridement or tenodesis [68].
Due to the results of biomechanical studies of the role of the biceps labral complex in glenohumeral stability [48-52] some have considered repair of SLAP lesion with a biceps tenodesis. Despite having similar return to sport or work, Chalmers et al [24] found that patients treated with combined procedures did significantly worse in terms of ASES and VAS scores. Even subgroup analysis with exclusion of worker’s compensation patients resulted in similar findings. At this time, the author recommends bicep tenodesis young patients in revision cases and in primary cases where the biceps is considered as a source of pain and selective injections into the biceps sheath temporarily relieves their pain.
4. OLDER, ATHLETIC PATIENTS
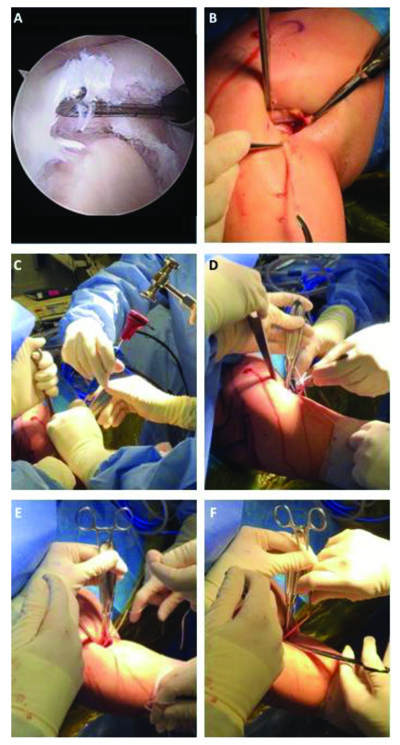
Numerous studies to date have linked the outcomes of SLAP repair versus tenodesis to the patient’s age [22, 23, 25-27, 35, 41, 61, 69]. The cohort studies of Alpert et al [22] and Schrøder et al [35] documented in the long-term, patients older and younger than forty years of age perform as well in terms of functional scores and outcomes. These studies however, discuss that the older patients were more inclined to get stiffer post operatively and took longer to regain full motion [22]. Katz et al [31] retrospectively looked at patients with poor outcomes, and the average age of the study was 43 years old. One of the largest cohort studies (179 patients), albeit a military population, found the relative risk for failure to be 3.45 in patients older than 36 years of age [34]. Taylor et al [69] performed a database study that demonstrated age greater than 40 (OR 1.5), Female Sex (OR 1.5), obesity (OR 1.8), smoking (OR 2.0) were all significant risk factors for failure following SLAP repair. Frank et al [70] analysis of a 62 patient cohort found similar risk factors for failure of SLAP repairs including age, smoking, diabetes, high demand labor and concomitant biceps symptoms. A systematic review pooled the studies and found that the rate of stiffness and post-operative complications increased with age leading the authors to recommend bicep tenodesis in patients over the age of forty [26]. This study also demonstrated that worker’s compensation is a risk factor for complications, and recommend bicep tenodesis in those cases as well. Denard et al [71] found similar findings that older patients with a SLAP repair had a delay in recovery of full motion compared to the tenodesis group. Retrospective studies have demonstrated equivalent outcomes between SLAP repair in younger patients and bicep tenodesis in older patients [23, 25, 29]. The cohort studies by Boileau et al [23] and Ek et al [25], had significantly older patients in the tenodesis group (37 versus 52; and 31 versus 47; respectively). These and other retrospective studies like Gottschalk et al [29] demonstrated that older patients may benefit from tenodesis instead of repair. The patients saw significantly better rates of return to sport following tenodesis. Boileau et al [23] had 93% satisfaction rate and 87% return to previous level of sport versus only 20% on the SLAP repair side. Bicep tenodesis allowed 89.66% of patients with either type II or Type IV lesions to return to their previous level of athletic activity [29]. Though not significant Ek et al [25] also saw a greater return to sport in the tenodesis versus repair groups (73% versus 60%; p=0.66). Due to the similar outcomes with fewer complications, the senior author recommends debridement and bicep tenodesis for older patients regardless of activity level and often in patients with third party liability or worker’s compensation cases (Fig. 3). Notably, there is a trend toward the use of biceps tenodesis in younger patients as a primary treatment.
5. PATIENTS WITH CONCOMITANT PATHOLOGY
Superior labrum anterior to posterior tears often do not present in isolation [12, 13], and as a result patients with concomitant pathology should not only have the additional pathology addressed [72], but receive a bicep tenodesis. Gupta et al [30] retrospectively studied 28 patients with the average age of 43.7 years and concomitant bicep tendonitis and SLAP tear demonstrated significant improvements in ASES, SANE, SST, VAS, and SF-12 scores with excellent satisfaction in 80% of patients. A recent randomized control trial of patients with rotator cuff tears and labral-biceps lesions were broken into three treatment arms: debridement, tenotomy, and tenodesis. There was no difference in the outcome scores across all three groups in terms of range of motion and functional scores [33]. Franceschi et al [27] found patients with a rotator cuff tear in the presence of a SLAP tear who received bicep tenotomy performed better in terms improvement of UCLA scores (10.1 to 32.1) compared to the patients who received SLAP repair (10.4 to 27.9). Another cohort study also demonstrated greater improvement in function in terms of ASES (88.6 versus 80.4) and UCLA scores (29.6 versus 26.0) when patients underwent biceps tenotomy instead of slap repair when the patient had large to massive cuff tears [73]. In many of these studies the patient cohorts were older than 50 years of age, which could skew outcomes against SLAP repairs, however, we still recommend patients with concomitant pathology be treated with bicep tenodesis or tenotomy unless the patient is a young athlete or high demand patient.
When deciding between tenodesis and tenotomy in treatment of SLAP tears, the senior author recommends a thorough discussion with the patient and selective intraarticular and biceps tendon sheath injections to assess for primary pain generators. Hsu et al [39] performed a systematic review and found that tenodesis had less cosmetic deformity but increase chance of bicep pain when compared to patients who received tenotomy. The study recommended tenotomy for patients who were older, more overweight, low demand, non-worker’s compensation, and less concerned about cosmesis. Another systematic review of tenodesis versus tenotomy demonstrated equal excellent/good outcomes (74% versus 77%), an 8% versus 43% cosmetic deformity, and 24% versus 19% post-operative occurrence of bicipital pain [37]. We agree with Hsu et al [39] in that a discussion with the patient and a consideration of patient factors be considered in the final decision between tenodesis versus tenotomy. The senior author primarily relies upon biceps tenodesis to minimize the chance of postoperative deformity and the possibility of cramping and does so utilizing a sub-pectoral tenodesis using a suture anchor (Arthrex, Naples, FL, Fibertac, Biceps Anchor).
6. REVISION CASES
Risk factors for failure of SLAP repair include age, smoking, obesity, female sex, and concomitant bicep pathology [31, 38, 69, 70]. Katz et al. [31] found that once a patient has failed first time repair, 71% will fail conservative therapy and 32% will continue to have suboptimal outcomes after a second surgical intervention. Revision SLAP repair has limited data, but an 11 patient review of six overhead athletes and five workers compensation cases saw only improvement of ASES to 72.5 and return to work and sport of 57.8% and 42.2% respectively [74]. McCormick et al [61], however, demonstrated significant improvements in ASES, SANE, and WOSI scores in their retrospective review of bicep tenodesis of 42 patients with failed SLAP repairs, including an 81% return to sports. A smaller civilian cohort of 11 patients saw similar improvements in functional outcome scores (ASES 54.5 to 78; SANE 42.5 to 70.4) and the 3 athletes returned to their sport [62]. In the cohort published by Boileau et al [23] there were 4/10 patients in the repair group who were unsatisfied and underwent revision surgery to bicep tenodesis. All four patients had excellent outcomes and returned to sport. In agreement with previous studies [46, 60, 62], the senior author believes that bicep tenodesis is a reliable solution to failed SLAP repairs.
CONCLUSION
SLAP tears can cause persistent pain and dysfunction in the shoulder and the management of Type II tears remains an evolving process with narrowing indications. Based on the existing literature, Type II tears in young (<40 years of age), athletic or high demand patients should be treated with direct SLAP repair. In older patients and worker’s compensation patients, Type II tears should often be treated with bicep tenodesis do to the higher rate of complications and revision/failures of repair in this population. In the cases of revision, bicep tenodesis remains an excellent solution for a difficult clinical scenario.
DISCLOSOURE
Brian J. Cole reports the following disclosures: Aesculap/B.Braun: Research support; American Journal of Orthopedics: Editorial or governing board; American Journal of Sports Medicine: Editorial or governing board; Aqua Boom: Stock or stock Options; Arthrex, Inc: IP royalties, Paid consultant, Research support; Arthroscopy: Editorial or governing board; Arthroscopy Association of North America: Board or committee member; Athletico: Other financial or material support; Biomerix: Stock or stock Options; Cartilage: Editorial or governing board; DJ Orthopaedics: IP royalties; Elsevier Publishing: IP royalties; Flexion: Paid consultant; Geistlich: Research support; Giteliscope: Stock or stock Options; International Cartilage Repair Society: Board or committee member; Journal of Bone and Joint Surgery - American: Editor only: Editorial or governing board; Journal of Shoulder and Elbow Surgery: Editor only: Editorial or governing board; Journal of the American Academy of Orthopaedic Surgeons: Editor only: Editorial or governing board; JRF Ortho: Other financial or material support; National Institutes of Health (NIAMS & NICHD): Research support; Operative Techniques in Sports Medicine: Publishing royalties, financial or material support; Ossio: Stock or stock Options; Regentis: Paid consultant, Stock or stock Options; Sanofi-Aventis: Research support; Smith & Nephew: Other financial or material support; Paid consultant; Tornier: Other financial or material support; Zimmer: Paid consultant; Research support.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Not applicable.
CONFLICT OF INTEREST
David Christian and Michael Charles have no conflict of interest. Brian Cole has no conflict of interest related to the content of this manuscript.
ACKNOWLEDGEMENTS
Decleared none.

