All published articles of this journal are available on ScienceDirect.

Lower Limbs Alignment in Patients with a Unilateral Completely Dislocated Hip
Authors Info & Affiliations
Abstract
Background:
Severe hip osteoarthritis is known to lead to secondary osteoarthritis of the knee joint. It is not clear whether contracture or a leg length discrepancy is more important in determining the knee alignment.
Methods:
In this study, 48 hips in 48 patients with a unilateral completely dislocated hip (Crowe IV) were recruited. The patients were divided into two groups (Crowe IVa and IVb). The Crowe IVa group had completely dislocation with psudo-articulation, and the Crowe IVb group had completely dislocation without psudo-articulation. The lower limb alignment was divided into three patterns according to the femorotibial angle; varus (≥176 degrees), neutral(170 to 175 degrees) and valgus(≤169 degrees).
Results:
The combination of valgus alignment on the affected side and varus alignment on the unaffected side, so-called “windswept deformity” was observed in 12.5% of the patients; this included 18.2% and 7.7%, in the Crowe IVa and Crowe IVb groups, respectively. The valgus alignment on the unaffected side, namely “long leg arthropathy,” was found to have occurred in 6.3% of the patients, including 13.6% of the patients in the Crowe IVa group; there were no cases of long “leg arthropathy” in the Crowe IVb group.
Conclusion:
The lower limb alignment on the unaffected side had a tendency to be varus in the Crowe IV patients. The “windswept deformity” was observed in each of the groups; however, “long leg arthropathy” was only found in the Crowe IVa group.
INTRODUCTION
It is known that patients with hip osteoarthritis (OA) have disturbed kinetics in adjacent joints and in the pelvis due to the impaired hip. Severe hip OA is known to lead to secondary OA of the knee joint. Smillie et al. described this phenomenon as “Coxitis Knee” [1]. This is the name applied to the particular form of hip OA associated with ankylosis, arthrodesis or any condition of the hip joint in which the rotation is severely restricted. On the other hand, Brattstrome et al. described that a leg length discrepancy (LLD) causes disease of knee known as “long leg arthropathy” [2]. William et al. described that a leg-length inequality of 1 cm or more increased the odds of incident symptomatic knee OA in both the shorter and longer legs compared with patients who have an inequality less than 1 cm [3]. Most cases of hip OA have both contracture and LLD. Therefore, it is not clear which factor would more strongly affect the knee alignment.
The aim of the present study was to investigate the differences in the effects of LLD and hip contracture on the knee alignment in a preliminary observational retrospective study. To compare the impact of LLD and hip contracture, patients with a unilateral completely dislocated hip joint with or without contracture were selected for the present study. These two types of hip conditions could provide a model for analyzing the roles of LLD and hip contracture in knee alignment.
The current study protocol adhered to the ethical guidelines of the 1975 Declaration of Helsinki. The review board of the Faculty of Medicine, Saga University at Saga approved this study.
MATERIALS AND METHODS
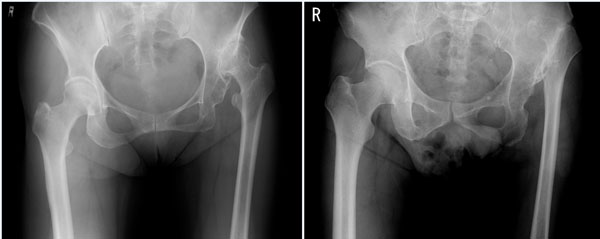
This study was a preliminary retrospective observational cohort study. Between January 2006 and July 2013, 87 total hip arthroplasty were performed in our institution for the patients with highly dislocated hip joint classified as type IV according to the Crowe classification [4], which classifies the developmental dysplastic hips according to the magnitude of subluxation of the femoral head. Crowe IV indicates more than 100% subluxation. The cases of unilateral completely dislocated hip were recruited for this study. And we excluded any patients with previous knee surgery or who were missing data for this study. Finally, 48 hips in 48 patients were recruited for this study (Table 1). The forty eight hips were classified Crowe IV into IVa and IVb. The Crowe IVa group had completely dislocation with psudo-articulation, and the Crowe IVb group had completely dislocation without psudo-articulation (Fig. 1). Twenty-two patients were classified at Crowe IVa, and 26 patients were classified at Crowe IVb in the present study.
| Crowe classification | ||||
|---|---|---|---|---|
| Characteristic | Total (n=48) | IVa (n=22) | IVb (n=26) | P-value |
| Age (year)(mean±SD) | 66.3±7.9 | 68.2±8.2 | 64.7±7.6 | 0.131 |
| Women (%) | 91.7 | 95.5 | 88.5 | |
| Height (cm)(mean±SD) | 148.0±6.0 | 148.1±7.0 | 147.9±5.4 | 0.941 |
| Weight (kg)(mean±SD) | 52.2±7.3 | 49.8±6.0 | 54.1±7.7 | <0.05 |
| BMI(kg/m2)(mean±SD) | 23.8±3.1 | 22.7±1.9 | 24.8±3.6 | <0.05 |
All data were reviewed retrospectively from preoperative medical records or preoperative radiographs of the pelvis with the patient in a supine position, and both lower legs in entirety with the patient in a standing position. The hip range of motion (ROM) was reviewed from medical records. The LLD was measured by preoperative anteroposterior radiographs of the pelvis with the patient in a supine position. The LLD was defined as the difference in the distance from the inter-teardrop line to the bilateral tips of the lesser trochanters [5].
The radiographs of the entire lower legs were used to assess the lower limb alignment. The lateral angle at the intersection between the femoral axis and the tibial axis, the femorotibial angle (FTA), was measured [6]. We classified the FTA according to Knee Society classifications [7]: varus (≥176 degree), neutral (170 to 175 degree) and valgus (≤169 degree).
Furthermore, all patients were sub-classified into nine groups based on the combination of the alignment of the affected and unaffected sides.
Osteoarthritis of knee joints was defined using Kellgren-Lawrence (K-L) grading scale [8]. The K-L grading scale consisted of five categories: grade 0 (no radiographic features of osteoarthritis), grade 1 (possible joint space narrowing and osteophyte formation), grade 2 (definite osteophyte formation with possible joint space narrowing), grade 3 (multiple osteophytes, definite joint space narrowing, sclerosis and possible bony deformity), grade 4 (large osteophytes, marked joint space narrowing, severe sclerosis and definite bony deformity).
The correlation with the adduction contracture of the hip and the lower leg alignment was assessed to investigate the correlation between the abduction angle of the hip joint and the FTA.
We calculated the means and standard deviations for the characteristic of the study participant. Paired-t tests were used to compare the FTA and ROM of the hip between the affected and unaffected sides. Student’s t test was used to compare the age, height, weight, body mass index, LLD, FTA and ROM of the hip between the Crowe IVa and Crowe IVb groups. Pearson's product-moment correlation coefficient was used to highlight abduction of hip joint vs FTA
A value of p<0.05 was considered to be significant. All analyses were done using the SPSS Version 21 for Windows software program (IBM Corp, Armonk, NY, USA).
RESULTS
Table 1 shows the characteristics of the study participants. The Crowe IVb group had a higher body mass index than the Crowe IVa group (p<0.05). Table 2 shows the FTA and ROM of the hip on both the affected and unaffected sides. The FTA of the affected side was smaller than the FTA of the unaffected side (p<0.01). With the exception of the internal and external rotation, the affected side demonstrated a significantly smaller ROM in comparison with the unaffected side. Table 3 shows the results of a comparison of the physiological findings of the affected and unaffected sides between Crowe IVa and IVb. The LLD of the Crowe IVb group was greater than that of the Crowe IVa group (p<0.05). On the affected side, the Crowe IVa group demonstrated a significantly smaller ROM in comparison with the Crowe IVb group in all directions (p<0.01). In contradiction to the affected side, there were no significant differences between the Crowe IVa and IVb groups in the ROM of the unaffected side.
| Affected side | Unaffected side | P-value | |
|---|---|---|---|
| FTA (degrees)(mean±SD) | 173.9±4.3 | 179.5±6.1 | <0.01 |
| ROM (degrees)(mean±SD) | |||
| Flexion | 82.8±27.8 | 112.6±9.3 | <0.01 |
| Extention | -3.6±6.0 | -0.1±1.6 | <0.01 |
| Abduction | 18.9±12.0 | 34.7±7.2 | <0.01 |
| Adduction | 15.7±8.0 | 21.1±4.3 | <0.01 |
| External rotation | 34.2±26.5 | 37.1±12.1 | 0.487 |
| Internal rotation | 39.1±34.0 | 29.9±13.1 | 0.102 |
Fig. (2) is a representation of the knee alignment, which has been divided into nine combinations of varus (FTA≥176 degrees), neutral (170 to 175 degrees) and valgus (FTA≤169 degrees) for the affected and unaffected knees. Normal alignment was most frequently (58.3%) observed on the affected side, and the varus deformity most frequently (85.4%) occurred on the unaffected side. The combination of valgus alignment on the affected side and varus alignment on the unaffected side, the so-called “windswept deformity (Fig. 3) ” [9], was observed in 12.5% of the Crowe IV patients; this included 18.2% and 7.7%, in the Crowe IVa and Crowe IVb groups, respectively Figs. (2, 4 and 5).


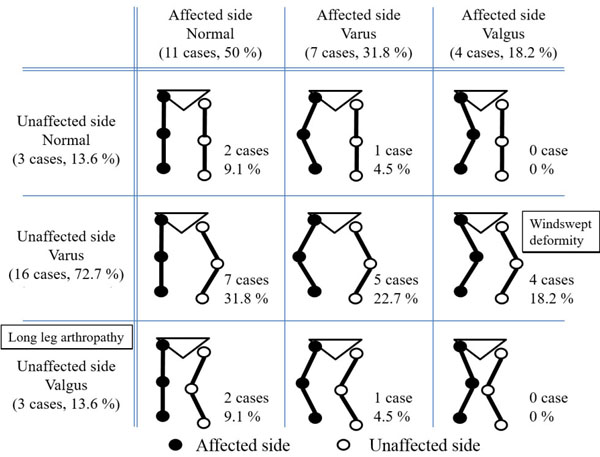

The valgus alignment on the unaffected side, with so-called “long leg arthropathy (Fig. 3)” [2], was present in 6.3% of the Crowe IV patients (Fig 2). In the Crowe IVa group, a valgus deformity on the unaffected side, “long leg arthropathy”, was observed in 13.6% of the patients, but it was not observed in any of the patients in the Crowe IVb group Figs. (4 and 5).
| Crowe classification | |||||
|---|---|---|---|---|---|
| IVa (n=22) | IVb (n=26) | P-value | |||
| LLD (mm) (mean±SD) | 53.1±12.8 | 63.1±12.4 | <0.05 | ||
| FTA degrees) (mean±SD) | |||||
| Affected side Unaffected side |
173.1±4.7 177.5±7.5 |
 |
174.5±3.8 181.2±4.0 |
 |
0.282 0.050 |
| ROM (degrees) (mean±SD) | |||||
| Flexion | |||||
| Affected side Unaffected side |
64.5±25.6 111.6±8.9 |
|
98.3±19.1 113.5±9.7 |
|
<0.01 0.490 |
| Extention | |||||
| Affected side Unaffected side |
-6.6±7.1 -0.5±2.1 |
|
-1.2±3.3 0.2±1.0 |
<0.01 0.200 |
|
| Abduction | |||||
| Affected side Unaffected side |
13.0±10.4 34.3±8.8 |
|
23.8±11.1 35.0±5.7 |
|
<0.01 0.756 |
| Adduction | |||||
| Affected side Unaffected side |
13.2±7.0 21.4±4.7 |
|
17.9±8.3 21.0±4.0 |
<0.01 0.753 |
|
| External rotation | |||||
| Affected side Unaffected side |
13.4±8.2 34.8±13.0 |
|
51.9±23.5 39.0±11.1 |
|
<0.01 0.235 |
| Internal rotation | |||||
| Affected side Unaffected side |
12.7±22.7 32.7±11.6 |
|
61.5±24.6 27.5±13.9 |
|
<0.01 0.163 |
Osteoarthritis of the knee joint was observed in 57% of all knee joints (Table 4). In patients with grade 3 or 4 osteoarthritis according to the K-L grading scale, only the knee joint on the affected side was observed; however, 12 knee joints were observed on the unaffected side (Table 5). There was no significantly correlation between the abduction of the hip joint and the FTA (Table 6).
| Grade 0 | Grade 1 | Grade 2 | Grade 3 | Grade 4 | |
|---|---|---|---|---|---|
| Varus group (number of knees) |
8 | 7 | 2 | 4 | 5 |
| Neutral group (number of knees) |
21 | 11 | 5 | 1 | 0 |
| Valgus group (number of knees) |
12 | 12 | 5 | 2 | 1 |
| Grade 0 | Grade 1 | Grade 2 | Grade 3 | Grade 4 | ||
|---|---|---|---|---|---|---|
| Varus group (number of knees) |
affected side | 2 | 1 | 0 | 0 | 0 |
| unaffected side | 6 | 6 | 2 | 4 | 5 | |
| Neutral group (number of knees) |
affected side | 11 | 5 | 2 | 0 | 0 |
| unaffected side | 10 | 6 | 3 | 1 | 0 | |
| Valgus group (number of knees) |
affected side | 12 | 10 | 4 | 1 | 0 |
| unaffected side | 0 | 2 | 1 | 1 | 1 | |
| r | P value | |
|---|---|---|
| Total (n=48) | 0.078 | 0.597 |
| IVa group (n=22) | 0..074 | 0.743 |
| IVb group (n=26) | -0.005 | 0.982 |
DISCUSSION
In the present study, we investigated the lower limb alignment in patients with a unilateral completely dislocated hip, with or without contracture. We found that the “windswept deformity” was observed in each group; however, “long leg arthropathy” was only found in the Crowe IVa group. It is possible that “long leg arthropathy” was mainly influenced by the contracture of the affected hip joint.
The present study is associated with several limitations. First, the present study is considered to be a preliminary retrospective observational cohort study because of the relatively small study population of 48 patients. Second, the present study used only anteroposterior radiographs, without a lateral view, for the radiological evaluation. Thus, we only examined the coronal alignment. Third, several investigators performed the measurements of the hip ROM in a retrospective fashion; thus, inter-observer variability existed. Finally, only the morphological changes in the knee alignment were evaluated. The pathological process was not evaluated.
A recent study showed that patients with unilateral hip OA have a higher incidence of lateral knee OA than medial knee OA on the ipsilateral side [10]. Fujimaki et al. noted that when the affected hip joints presented with adduction contracture, the knee joints of the affected side are thought to have become valgus due to unilateral hip OA [11]. Kandemir et al. noted that the pathological condition of the hip joint in patients with developmental dysplasia of the hip results in developmental changes in the osseous anatomy of the knee joint, with the development of a valgus deformity of the lower extremity [12]. However, valgus deformities on the affected side were only observed in 12.5% of the whole Crowe IV patient population. A similar tendency was observed in both the Crowe IVa (18.2%) and IVb (7.7%) groups. The discrepancy in these results might be due to the baseline of the classification of varus and valgus. In the current study, the FTA was classifiedaccording to the Knee Society classification [7]. However, all of the subjects in this study were Japanese and Ariumi et al. [13] previously investigated lower limb alignment in healthy elderly Japanese subjects by computed tomography and reported that the mean FTA was 177.5±2.5° in males, 176.6±2.5° in females and 177.0±2.5° overall. Japanese individuals show a tendency to develop varus deformities.
Previous studies have confirmed that the knee contralateral to the affected hip tends to be varus, and that the ipsilateral knee tends to be valgus, similar to the phenomenon known as the “windswept deformity” [9]. In the current study, the “windswept deformity” was 12.5% in the whole Crowe IV patient population.
“Long leg arthropathy” indicates the presence of valgus deformity on the unaffected side [2]. In the present study, “long leg arthropathy” was observed in three cases, all of whom were in the Crowe IVa group.
Kandemir et al. [12] described that the accentuation of the valgus deformity of the knee has been recognized as a problem after hip reconstruction at the true acetabulum in patients with developmental dysplasia of the hip. The alignment between the femur and the tibia does not change, but as the patient tries to walk, either with the knees closer together or with a greater interfoot distance, the valgus deformity appears to increase. Shakoor et al. [13] showed that the medial compartment load of the knee was significantly higher in the contralateral knee relative to the treated side after unilateral THA, and that patients undergoing unilateral THA were more likely to have TKA on the contralateral side than on the ipsilateral side. Thus, a meticulous preoperative analysis and planning should be performed to avoid creating postoperative problems.
Contrary to all expectations, we did not observe a correlation between the abduction of hip joint and the FTA. The FTA might have been affected by multifactorial anatomical abnormalities, for example lumber scoliosis.
In the present study, severe osteoarthritis was more frequently observed in the knee joints on the unaffected side. The overloading of weight on the unaffected side might have been affected the development of osteoarthritis in the knee joints.
CONCLUSION
In conclusion, the lower limb alignment on the affected side had a tendency to remain normal in the Crowe IV patients. The “windswept deformity” was observed in each of the groups. On the unaffected side, although there was valgus alignment, “long leg arthropathy” was only found in the Crowe IVa group; no cases were observed in the Crowe IVb group. The accumulation of information about the adjacent joint in hip OA will contribute to determining the optimal treatment for patients with multiple joint disorders.
LIST OF ABBREVIATIONS
| FTA | = Femorotibial angle |
| K-L | = Kellgren-Lawrence |
| LLD | = Leg length discrepancy |
| OA | = Osteoarthritis |
| ROM | = Range of motion |
CONFLICT OF INTEREST
The authors did not receive and will not receive any benefits or funding from any commercial party related directly or indirectly to the subject of this article.
ACKNOWLEDGEMENTS
The authors thank Drs. Satoshi Ikebe, Masaya Ueno and Sakumo Kii for their contributions to this study.

