All published articles of this journal are available on ScienceDirect.

Early Degenerative Change After Anterior Cruciate Ligament Augmentation of the Knee: A Case Report
Authors Info & Affiliations
Abstract
Introduction
Anterior Cruciate Ligament (ACL) reconstruction is performed to improve activities of daily living and return to sports. However, it remains to be proven whether ACL reconstruction can prevent later development of Posttraumatic Osteoarthritis (PTOA).
Case
A 36-year-old male presented with moderate right knee pain and gait disturbance persisting for approximately three months. Arthroscopic examination revealed a slightly lax ACL and a medial meniscal tear. ACL augmentation using a 7-mm single-bundle semitendinosus tendon graft and partial medial meniscectomy was performed. Five months postoperatively, mild knee pain occurred at his work. Magnetic resonance imaging showed osteoarthritic change in the medial tibiofemoral joint. Conservative treatment, including muscle exercises and dietary weight loss were initiated. One year postoperatively, the patient was almost asymptomatic and had resumed daily activities.
Conclusion
ACL reconstruction can improve knee stability in ACL-deficient knees. However, it could not delay the later development of Posttraumatic Osteoarthritis (PTOA) completely. Meniscus status and body mass index may be risk factors for PTOA after ACL reconstruction in this case.
1. INTRODUCTION
The Anterior Cruciate Ligament (ACL) is one of the important ligaments that provide stability to the knee. Andriacchi et al. reported that ACL deficiency leads to chronic changes in knee loading and increased forces on the cartilage and other joint structures [1]. Luc B et al. reported that 50-90% of ACL injuries progress to Posttraumatic Osteoarthritis (PTOA) [2]. It is believed that ACL reconstruction helps to restrain the anterior tibial translation, regain proper joint kinematics, restore knee stability, and prevent excessive torsional loading [3]. Hohmann E et al. reviewed that ACL reconstruction results in a significantly more stable knee with superior clinical and functional outcomes. However, these advantages over conservative treatment were not routine activities of daily living, and subjective patient-perceived outcomes favored nonsurgical treatment [4]. Convincing evidence for the superiority of ACL reconstruction over conservative management in reducing the incidence of PTOA remains lacking [5]. We report a case of early degenerative changes following ACL augmentation of the knee.
2. CASE
A 36-year-old male presented with moderate right knee pain and gait disturbance. The symptoms began after stair climbing and persisted for approximately three months. At a nearby hospital, Magnetic Resonance Imaging (MRI) revealed a medial meniscal tear Fig. (1), prompting referral to our department. The patient’s past medical history included a traffic accident (no injury to the knee joint).
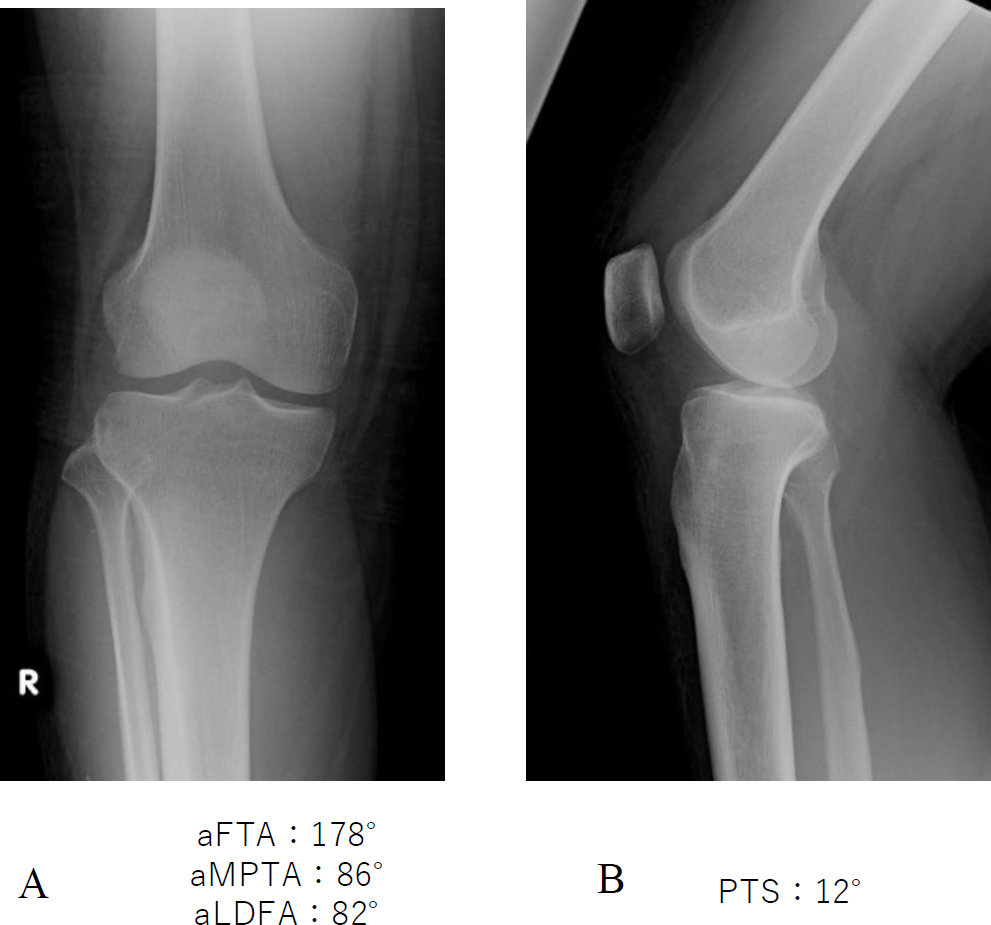
Preoperative radiograph.
A. The anatomical lateral distal femoro-tibial angle was 178°. B. The posterior tibial slope was 12°.
Physical examination revealed swelling and no effusion, but tenderness was noted in the right knee. The range of motion was 0° to 140°. The McMurray test for meniscal injury, the anterior drawer test, and the Lachman test were positive. The Body Mass Index (BMI) was 33.48. The Lysholm knee score was 75. The patient had no patellofemoral symptoms. Plane radiographs showed no bony or soft tissue abnormalities, including intra-articular loose bodies. The anatomical lateral distal femorotibial angle was 178°. The posterior tibial slope was 12° Fig. (1A, B). MRI confirmed ACL insufficiency and a medial meniscal tear Fig. (2A, B).

Preoperative MRI (right knee, A: T2-weight gradient echo image B:T2-weighted image) showed ACL, medial meniscal tear, and a bone bruise in medial tibial plateau.
Arthroscopic examination revealed a slightly lax ACL Fig. (3A, B) and a medial meniscal meniscotibial-side flap tear of the middle portion. ACL augmentation was performed using a 7-mm single-bundle semitendinosus tendon graft Fig. (4). Partial meniscectomy for a meniscotibial-side flap tear of the middle portion was performed Fig. (5A, B).
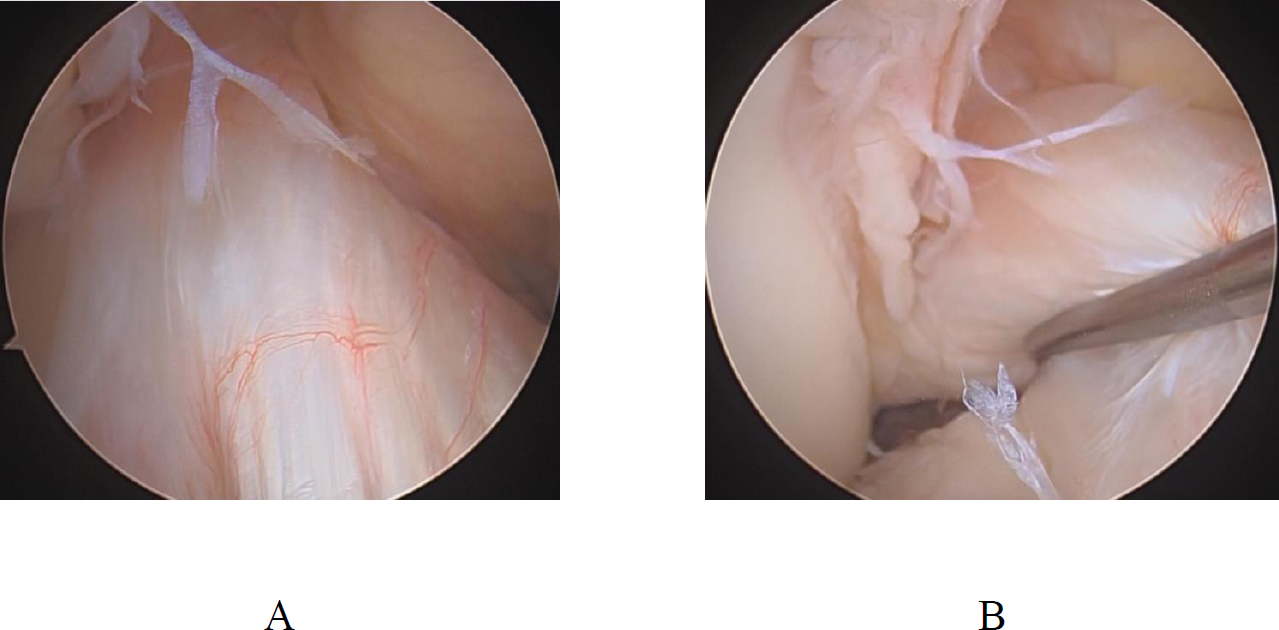
Arthroscopic view from an anterolateral portal.
A. ACL appears normal.
B. ACL is relaxed in probing.

Postoperative X-ray image (A-P view).
ACL augmentation was performed using single-bundle graft.
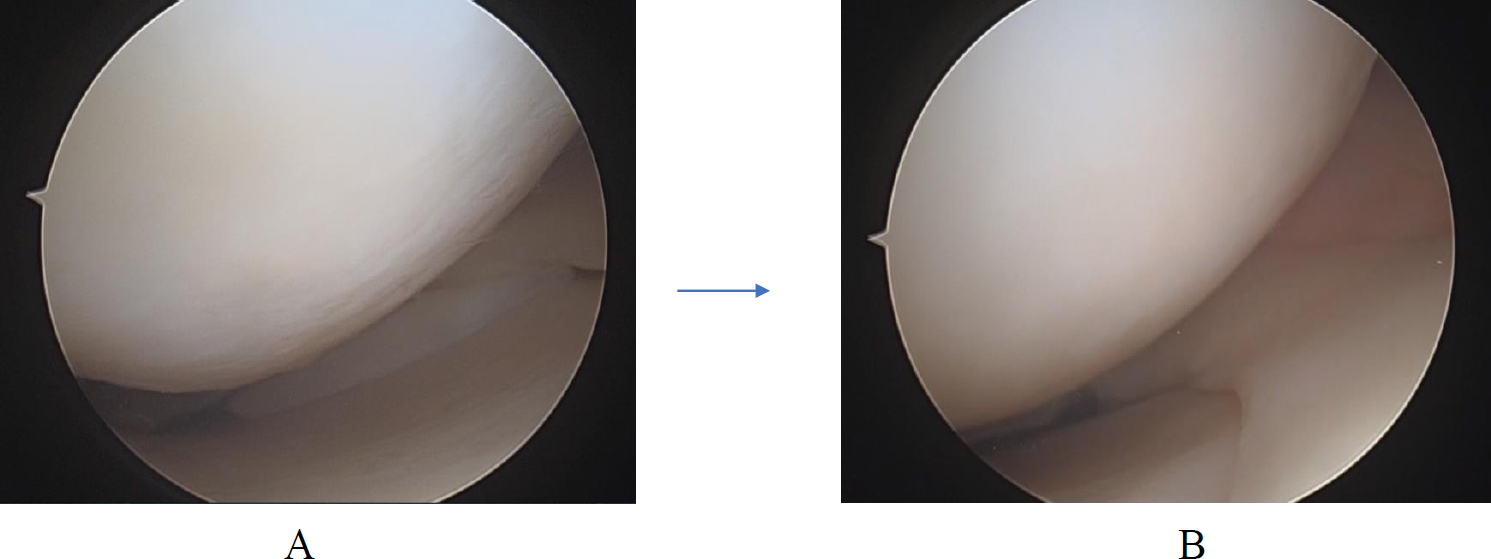
Arthroscopic view from an anterolateral portal.
A. medial meniscal meniscotibial side flap tear of middle portion.
B. Medial meniscus after partial meniscectomy.
Postoperatively, the patient had the knee immobilized in a knee brace for two weeks, after which range-of-motion and muscle-strengthening exercises were initiated. Full weight bearing was permitted at six weeks. Rehabilitation was conducted consistently at least twice a week. Five months postoperatively, mild knee pain occurred at work. MRI showed osteoarthritic change in the medial tibiofemoral joint Fig. (6A). Six months postoperatively, knee instability and severe knee pain occurred at work. MRI showed a bone bruise of the medial femoral condyle Fig. (6B). Swelling and medial knee joint line tenderness were noted. The range of motion was -5° to 140°. The McMurray test for meniscal injury, anterior drawer, and Lachman tests were negative. The symptoms had gradually subsided over two weeks. The bone bruise decreased on follow-up MRI Fig. (6C). Conservative treatment, including muscle-strengthening exercises and intentional dietary weight loss, was initiated. The diet was drug-free, self-administered, and not supervised. The patient’s BMI improved to 27.76 in four months. At one year postoperatively, the patient was almost asymptomatic with a Lysholm knee score of 90.
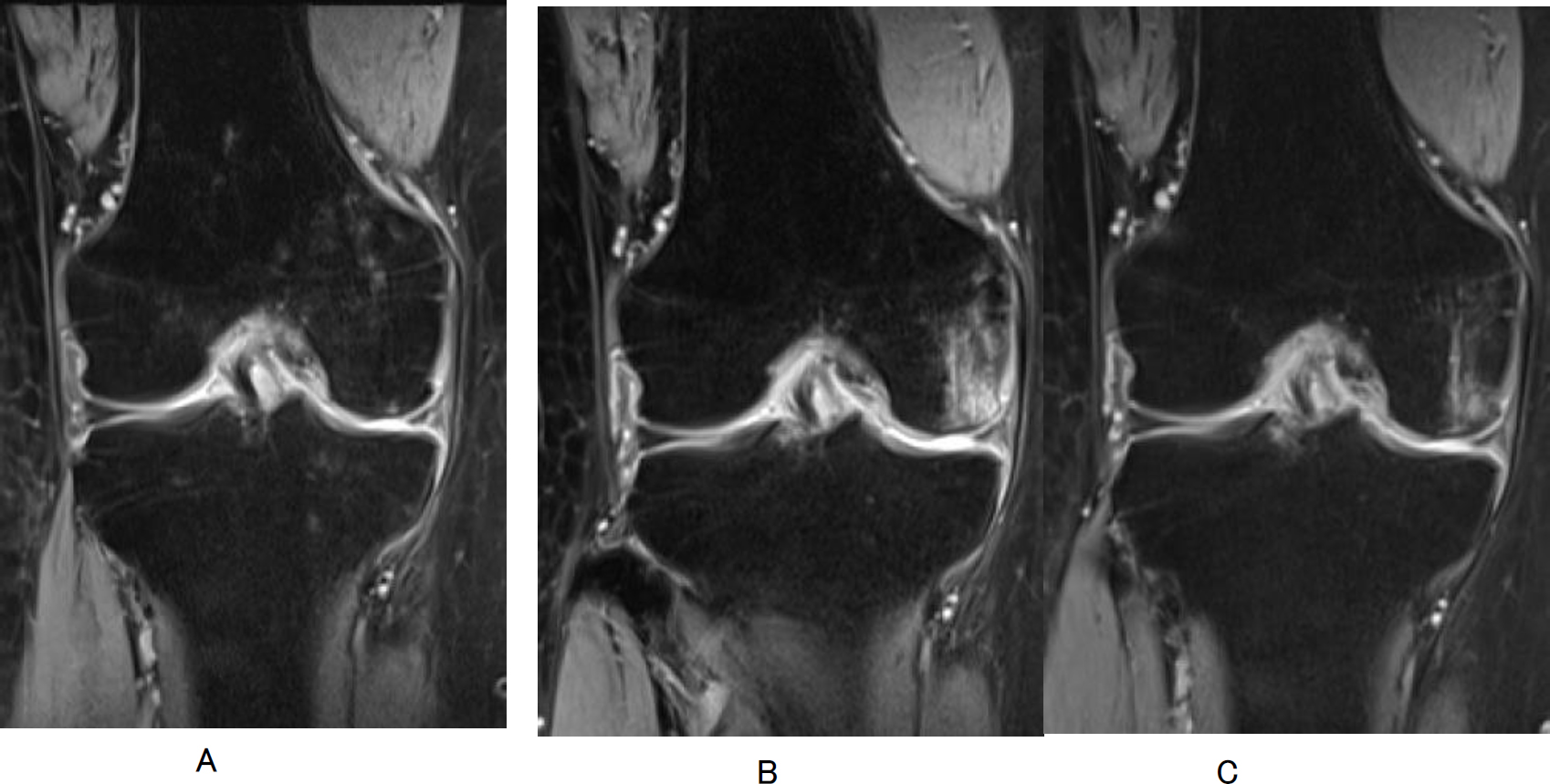
MRI A:5months, B:6months, C:7 months after the injury (right knee, T2-weight gradient echo image) showed A bone bruise were found in femoral medial condyle.
3. DISCUSSION
ACL reconstruction is performed to stabilize the knee joint and improve quality of life. Lohmander et al. reported that ACL injuries can result in early onset osteoarthritis, with pain, functional limitations, and decreased quality of life [6,7]. In the present case, ACL augmentation was performed to treat ACL dysfunction. However, the symptoms in the knee had appeared at five months postoperatively. MRI revealed early osteoarthritic changes without evidence of bone bruising. One month later, as the patient’s pain had worsened, a bone bruise appeared in the medial femoral condyle on MRI. The symptoms were reduced with conservative treatment in about one month, and the bone bruise gradually decreased on MRI. Kroker et al. reported that 19 of 21 bone bruises healed within 2 months and all 21 resolved by 8 months [8]. Mine et al. reported that the bone bruise almost disappeared in parallel with the reduction of pain symptoms in a case report [9]. ACL reconstruction can prevent Osteoarthritis (OA) by restoring the biomechanical stability of the knee joint [7,10]. Papannagari et al. reported that although ACL reconstruction improves knee stability in ACL-deficient knees, it does not restore normal knee kinematics [11]. Friel et al. review that ACL reconstruction has not been shown to prevent later development of Posttraumatic Osteoarthritis (PTOA) [7]. Moreover, they stated candidate risk factors for PTOA, including neuromuscular factors, meniscus status, BMI, chondral damage, age, graft choice, and time interval between injury and surgical intervention [10,12]. In the present case, meniscus status and elevated BMI were considered particularly relevant risk factors.
Multiple studies have reported that meniscal injury, meniscus surgery, or meniscectomy upon ACL repair or reconstruction increases the risk of OA development [7,13-19]. Amin et al. reported ACL deficiency increased the risk for cartilage loss of the medial tibiofemoral compartment; however, there was no increased risk for cartilage loss following adjustment for the presence of medial meniscus tears [20]. Aglietti et al. reported that the incidence of OA in ACL-reconstructed patients with repaired menisci is lower than that of those with partial meniscectomy [21]. Oiestad BE et al. reported that the status of the meniscus has been identified as the most important factor for developing posttraumatic OA after an ACL injury, regardless of whether the patient undergoes ACL surgery or nonoperative treatment [22]. In this case, meniscal repair may have been better despite potential healing challenges. However, considering the type and location of the meniscal tear, the probability of meniscal healing after meniscal repair appears to be quite low. Mehl J et al. reported that medial opening-wedge High Tibial Osteotomy (HTO) alone can improve pain and even subjective knee stability [23]. Therefore, assuming that there was ACL dysfunction and that the meniscus may be damaged due to a change in early OA, HTO may have been considered as the initial surgical option, even though there was no degenerative change in the medial tibiofemoral joint.
Moreover, BMI may be another important risk factor. Bodkin et al. and Ang et al. have reported that patient BMI was correlated with PTOA after ACL reconstruction [17,24]. Lieberthal J et al. reported that obesity is related to increased levels of IL-6 and TNF-α, which are pro-inflammatory indicators of PTOA development [25]. In this case, obesity is likely to be involved in the PTOA development. Actually, the patient’s symptoms improved significantly with dietary weight loss and muscle-strengthening exercises.
CONCLUSION
ACL reconstruction can improve knee stability, but may not completely prevent the development of PTOA. Meniscal status and elevated BMI may be particularly applicable risk factors for early PTOA development in this case.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: T.M.: Designed the study, analyzed the data, and wrote the manuscript; K.Y., M.S., R.K., T.T., and K.I.: Collected the data and participated in the design of the study; T.Y.: Analyzed the data and helped write. All authors have read and approved the final manuscript.
LIST OF ABBREVIATIONS
| MRI | = Magnetic Resonance Imaging |
| ACL | = Anterior Cruciate Ligament |
| BMI | = Body Mass Index |
| PTOA | = Posttraumatic Osteoarthritis |
| OA | = Osteoarthritis |
| HTO | = High Tibial Osteotomy |
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
All data generated or analyzed during this study are included in this published article.
FUNDING
This research was supported by the commissioned research expenses to Kanmon Medical Center (Shimonoseki, Japan) from Kyocera Japan and Japan Medical Dynamic Marketing ING.
ACKNOWLEDGEMENTS
Declared none.

