All published articles of this journal are available on ScienceDirect.

Arthroscopic Lysis of Arthrofibrosis and Manipulation after Knee Surgery
Authors Info & Affiliations
Abstract
Introduction
Arthrofibrosis is a well-known knee surgery complication. Optimal treatment of postoperative knee arthrofibrosis is very important. Arthroscopic lysis and manipulation are often effective. We evaluated the indications for and the utility of arthroscopic lysis and knee manipulation.
Methods
Ten patients (10 knees) underwent arthroscopic lysis of arthrofibrosis and knee manipulation. The follow-up evaluation included a clinical assessment. The mean follow-up time was 3.3 ± 1.2 months (from 2 to 6 months).
Results
The mean final gained arc of motion was 35.2°± 14.4°. The mean preoperative Lysholm score was 73.5 ± 2.5. The mean postoperative score was 90.5 ± 9.5. At the time of the initial surgery, the ROM tended to be lower in patients who had undergone surgery for > 6 months prior.
Conclusion
Final ROM outcomes were better in cases within 6 months of the initial surgery than in cases over 6 months. Arthroscopic lysis and manipulation for postoperative arthrofibrosis of the knee should be performed as early as possible, within 6 months of the initial surgery.
1. INTRODUCTION
Knee arthrofibrosis is often observed as a complication of traumatic injuries or subsequent surgery, both inside and outside the knee joint [1]. The underlying causes include fibrosis of the suprapatellar bursa and the surrounding vastus intermedius muscle, adhesion of the patella to the intercondylar region of the femur, fibrosis of the vastus lateralis muscle with adhesion to the lateral femoral condyle, and the rectus femoris muscle shortening [2]. The arc of motion of a normal knee is widely accepted to be 0° - 135°, with 0° - 120° of flexion required to accomplish most activities of daily living [3, 4]. Early knee motion and dedicated rehabilitation in the acute postoperative period are critical for decreasing the risk of arthrofibrosis [3, 5]. However, even after performing meniscal repair, the knee is often immobilized with a knee brace for one to two weeks [6]. Therefore, early knee motion is delayed. Optimal treatment of postoperative knee arthrofibrosis is very important. Arthroscopic lysis and manipulation are effective methods for postoperative knee arthrofibrosis [7]. In this study, we evaluated the indications for and utility of arthroscopic lysis and knee manipulation.
2. MATERIAL AND METHODS
Ten patients (10 knees) underwent arthroscopic lysis of adhesions at our institution between January 2013 and December 2023 for the treatment of postoperative knee arthrofibrosisis. The causes of knee arthrofibrosis were as follows: anterior cruciate ligament (ACL) injury in four knees, meniscal injury in four knees, patellar fracture in one knee, and patellar cartilage injury in one knee. Inclusion Criteria were patients with limitation of flexion to less than 120 degrees after initial surgery, not responding to physiotherapy for more than two months. Non-traumatic cases of knee stiffness and the presence of knee osteoarthritis were excluded.
The group comprised one male (one knee) and nine females (nine knees). Mean age at surgery was 38.7 ± 18.0 years (from 17 to 70 years old). The mean duration from initial surgery to arthroscopic lysis was 3.9 ± 2.5 months. The mean follow-up time was 3.3 ± 1.2 months (from 2 to 6 months). The subject was simply the number of cases over a 10-year period, and it just so happened that one of them was a man.
2.1. Surgical Technique
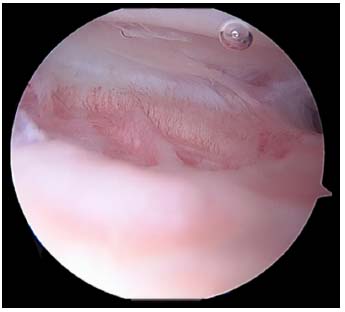
All the patients were placed in the supine position on an operating table. A tourniquet was applied to the thigh with the knee in the maximum possible flexion position to minimize capture of the quadriceps femoris muscle. The procedure was performed using the three-portal technique with two standard anterolateral and anteromedial portals in addition to the accessory superolateral portal [8, 9]. Tissue adhesions were identified (Fig. 1) and debrided using a radiofrequency device (Arthrocare, Arthrocare Sports Medicine, USA) (Fig. 2). Subsequently, gentle manipulation was performed by applying slight pressure on the tibial tubercle to avoid fractures or disruption of the extensor mechanism. After the operation, continuous passive motion was immediately initiated.
2.2. Clinical Assessment
2.2.1. Clinical Evaluations Included Range of Motion (ROM)
Preoperatively, 2 months, 3 months, and at the final follow-up. The correlation between age, time since initial surgery, and ROM was assessed in the final arc of motion. The lysholm score was calculated pre and postoperatively.
Statistical analysis was performed using the T-test and repeated measures ANOVA within and between-group comparisons. p-values less than 0.05 were considered statistically significant.

3. RESULTS
The mean knee ROM was 101.3°± 17.6° preoperatively, 137.4°± 9.5° at 2 months postoperatively, 139.1°± 9.0° at 3 months postoperatively, and was maintained at 138.8° ± 10.0° at the follow-up time.
The mean final gained arc of motion was 35.2°± 14.4°. There was no significant difference in ROM between ACL reconstruction and meniscal repair (Table 1). There was no significant difference in the acquired ROM between patients aged> 40 years and those aged< 40 years. At the time of initial surgery, the ROM tended to be lower in patients who had undergone surgery > 6 months prior. Patients with a pre-operative flexion > 110° had a smaller ROM than those with a ROM of less than 110° (Table 2). The mean preoperative Lysholm score was 73.5 ± 2.5 (range: 71-76). The mean postoperative score was 90.5 ± 9.5 (range: 81-100).
| - | Preop Range (Avg.) | Final Range | ROM Improvement |
|---|---|---|---|
| ACL injury N=4 | 106.3° | 106.3° | 35.5° |
| Meniscal injury 4 | 109.5° | 144° | 34.5° |
| Patellar Fx 1 | 65° | 125° | 60.0° |
| Articular cartilage injury 1 | 85° | 120° | 35.0° |
| - | - | ROM Improvement | p-value |
|---|---|---|---|
| N=10 | 37.5° | - | |
| Age | - | - | - |
| <40 | 4 | 35.5 | 0.77 |
| >40 | 6 | 35 | - |
| Duration from the Primary Surg | - | - | - |
| <3 M | 6 | 37.5 | - |
| 3~6 | 2 | 46 | 0.47 |
| >6 | 2 | 29 | - |
| Preop Range | - | - | - |
| <90° | 2 | 47.5 | - |
| 90~110 | 5 | 41 | 0.31 |
| >110 | 3 | 25 | - |
4. DISCUSSION
This study demonstrates that arthroscopic lysis and knee manipulation is an effective option for the treatment of postoperative knee arthrofibrosisis. However, final ROM outcomes were better in cases within 6 months of the initial surgery than in cases over 6 months.
Knee stiffness can progress to arthrofibrosis and is a frequent complication of fracture fixation and ligament reconstruction with an incidence of up to 17% [4, 5]. Arthrofibrosis is a well-known complication after total knee arthroplasty, occurring in approximately 1.3-5.2% of patients undergoing surgery [4, 5, 10, 11]. In addition, after ACL reconstruction, arthrofibrosis occurs in approximately 2-38% of patients undergoing surgery [10, 12-16]. After performing meniscal repair, knee brace fixation is often necessary to improve postoperative outcomes, and arthrofibrosis may occur [6]. Current studies suggest that a mix of genetic and environmental factors facilitates the upregulation of fibroblastic activity during the acute postoperative period, which plays a dominant role [16-18]. Arthrofibrosis is commonly treated with a combination of closed manual manipulation under anesthesia and physical therapy. Fabricant reported that patients with symptomatic arthrofibrosis of the knee refractory to extensive nonoperative treatment can achieve clinically significant improvements in ROM and knee function after arthroscopic lysis with manual manipulation [11]. In this study, the mean final gained arc of motion was 35.2°± 14.4°. The improvements in postoperative ROM were relatively good. There was no significant difference in ROM between ACL reconstruction and meniscal repair. Norman et al. reported indications for arthroscopic knee manipulation, including patients who had undergone open surgery, those with knee flexion limited to ≤90° under anesthesia, and cases unresponsive to non-invasive treatments [19]. Fackler et al. reported a 42° improvement in the knee arc of motion after arthroscopic lysis and knee manipulation in eight studies comprising 240 patients with all-cause atrial fibrillation [7]. However, in cases of intra-articular and extra-articular contractures, such as those due to quadriceps shortening or adhesions following femoral shaft fractures, sufficient improvement in ROM cannot be expected. Regarding the timing of the procedure, Norman et al. recommended performing the surgery 2-3 months postoperatively [19]. In this study, final ROM outcomes were better in cases within 6 months after the initial surgery than in cases over 6 months. However, in two cases, over 6 months after the initial surgery, intraoperative improvement in ROM was observed. It appears that extra-articular contractures, such as those caused by quadriceps shortening, are not involved. Future research should further investigate the comparison between cases within 6 months after the initial surgery and those beyond 6 months.
5. STUDY LIMITATION
One limitation of our study, which affected the statistical power of the results, was the small number of patients. Further investigation with larger sample sizes is required to obtain more accurate clinical data. Although this study had some limitations, it improved our current understanding of arthroscopic lysis of adhesions and manipulation after knee surgery.
CONCLUSION
Arthroscopic lysis and manipulation were an effective option for the treatment of postoperative knee arthrofibrosisis. Considering the possibility of extra-articular contractures appearing, arthroscopic lysis and manipulation should be performed as early as possible, within 6 months of the initial surgery.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: R.S., T.M.: Designed the study, analyzed the data, and wrote the manuscript; M.S., R.K., T.T., and K.I.: Collected the data and participated in the design of the study; Y.D.: Analyzed the data and helped to write. All authors have read and approved the final manuscript.
LIST OF ABBREVIATIONS
| ROM | = Range of motion |
| ACL | = Anterior cruciate ligament |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by Ethical Review Boards of Kanmon Medical Center Shimonoseki, Japan. A reference number with Ethics Committee approval is R07041.
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent to participate in our study was obtained from participants.
AVAILABILITY OF DATA AND MATERIALS
The authors confirm that the data supporting the findings of this study are available within the manuscript.
FUNDING
This research was supported by the commissioned research expenses to Kanmon Medical Center (Shimonoseki, Japan) from Kyocera Japan and Japan Medical Dynamic Marketing ING.
ACKNOWLEDGEMENTS
Declared none.

