All published articles of this journal are available on ScienceDirect.

Subchondral Insufficiency Fracture of the Femoral Head Complicated after Total Knee Arthroplasty
Authors Info & Affiliations
Abstract
Subchondral Insufficiency Fracture (SIF) of the femoral head has been observed in elderly women with osteoporosis. We present a rare case of subchondral insufficiency fracture of the femoral head complicated after total knee arthroplasty. Histological findings suggested osteonecrosis or SIF of the femoral head. MRI characteristics were considered to be useful for the differentiation between osteonecrosis and SIF. Several pathological conditions may be related to SIF of the femoral head, but its detailed pathogenesis is still unknown.
1. INTRODUCTION
Many complications after total knee arthroplasty (TKA) have been reported. As one of many complications, stress fractures of the femoral neck after TKA have also been reported [1-5]. However, subchondral insufficiency fracture (SIF) of the femoral head after total knee arthroplasty is rare. SIF of the femoral head has been observed in elderly women with osteoporosis [1, 4, 5]. SIF has been reported in 5 to 10% of patients who underwent total hip arthroplasty (THA) with a diagnosis of osteonecrosis of the femoral head [6-8]. SIF has a different pathology from osteonecrosis of the femoral head [9]. We present a rare case of subchondral insufficiency fracture of the femoral head complicated after TKA.
2. CASE REPORT
A 71-year-old female presented with bilateral knee pain and gait disturbance 6 years ago. The pain worsened and she came to our department to undergo bilateral TKA.
Regarding physical findings, swelling and tenderness were observed on both sides. The range of motion (ROM) was limited from 10° to 140°. There were no problems in the patellofemoral joint. There was no significant muscle weakness of the lower limbs.
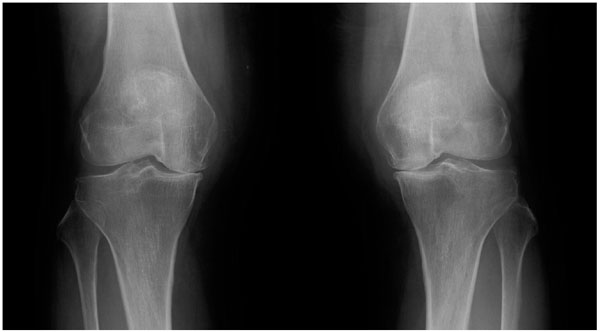
The hip-to-ankle standing X-ray image showed a Kellgren-Lawrence OA grade of 4. The anatomical lateral femur - tibia angle (FTA) was 187° on the right and 183° on the left (Fig. 1).
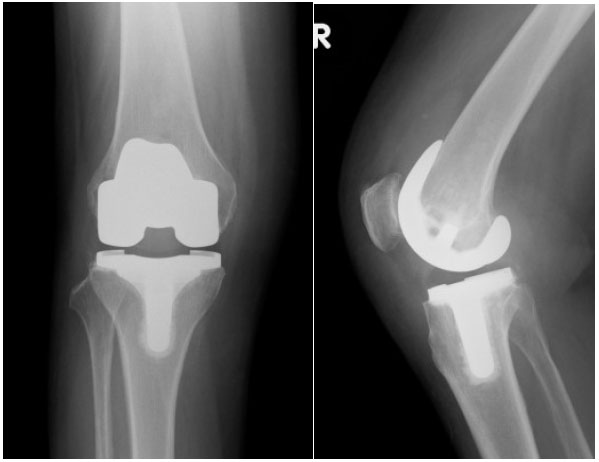
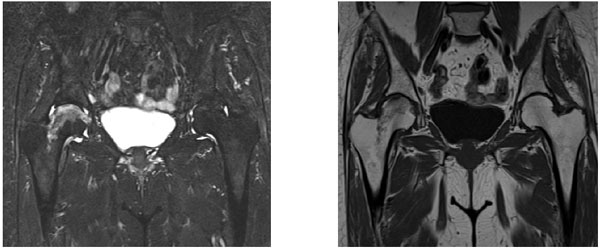
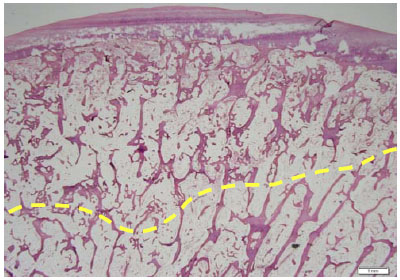
At first, right TKA was performed using a Bi-surface 5 PS type (Kyocera) with cement (Fig. 2). The patella was not replaced. To prevent pain after the operation, local periarticular injection was performed. After the operation, ROM exercise and partial weight bearing were started. Her postoperative course was good, and the ROM was from 10° to 120°. She was discharged 4 weeks after surgery. However, she developed pain in her right hip joint 4 weeks later, which progressively worsened. The X-ray film showed no sign of joint space narrowing, collapse of the femoral head, or osteophyte formation. The Sharp angle was 45°. The Center-edge (CE) angle was 35°. The Acetabular head index (AHI) was 86.7. The radiograph was normal. MRI revealed joint effusion and edematous area in the bone marrow of the right femoral head. An irregular low-signal-intensity band parallel to the articular surface was also observed (Fig. 3). Conservative therapy, such as rest and administration of NSAIDs, was attempted. The symptoms almost disappeared after 2 weeks and she was discharged. However, they worsened 2 weeks later. MRI revealed further joint effusion and greater edematous area in the bone marrow of the right femoral head. An irregularly serpentine shaped low-signal-intensity band parallel to the articular surface was observed (Fig. 4). We thought that the shape of the low-signal-intensity band was different from the band of ON. Right total hip arthroplasty was performed using a DJO linear THA system (Fig. 5). Histological examination revealed creeping substitution, necrotic debris and necrotic change of fatty bone marrow in subchondral bone (Fig. 6). These findings suggested osteonecrosis or SIF of the femoral head. We diagnosed her with subchondral insufficiency fracture of the femoral head based on MRI findings. Her postoperative course was good, and she was discharged 4 weeks after surgery. The patient was asymptomatic for two years postoperatively.


3. DISCUSSION
In cases of complication of the femoral head after TKA, stress fractures of the femoral neck have been reported [1-5]. However, SIF of the femoral head complicated after TKA is rare. There have been clinical reports of primary SIF in the femoral head since 1996. SIF of the femoral head without evidence of predisposing osteonecrosis has been reported as a new concept regarding femoral head collapse. However, it remains difficult to differentiate SIF and Osteonecrosis (ON) of the femoral head. In this case, histological findings suggested osteonecrosis or SIF of the femoral head. Several reports have proposed that the shape of the low-intensity band on T1 imaging may be useful for differentiating SIF from ON of the femoral head [10-15]. However, some cases of SIF have been reported to exhibit a smooth, well-delineated shape similar to that seen in ON. Yamamoto reported that both the clinical course and MRI characteristics are useful for the differentiation between ON and SIF. SIF of the femoral head is more common in elderly women. SIF has also been reported in renal and liver transplant recipients, and systemic lupus erythematosus patients after kidney transplantation [16-22]. The pathomechanism of SIF is unclear. Etiologically, bone fragility due to osteoporosis is considered to be the largest factor. Excessive contact pressure at the femoral head is a risk factor in addition to osteoporosis. Lumbar kyphosis leads to a posterior tilt of the pelvis to maintain the balance in the standing position. The posterior pelvic tilt causes a decrease in anterior coverage of the acetabulum [8]. This also induces excessive pressure on the femoral head [8]. In this case, the restriction of knee extension after TKA was 10°, and there was no change compared with preoperative restriction of knee extension. Therefore, there may be little change in the lumbar kyphosis and posterior pelvic tilt after TKA. We considered that TKA did not induce excessive pressure on the femoral head. Based on the intraoperative pressure on the femoral head when inserting the femoral component, we performed the technique as usual. This technique was not considered to influence SIF of the femoral head in this case. Several pathological conditions may be related to SIF of the femoral head, but the detailed pathogenesis remains unknown.
CONCLUSION
We reported a rare case of subchondral insufficiency fracture of the femoral head after TKA. Pathological findings suggested osteonecrosis or SIF of the femoral head, but the clinical course and MRI characteristics were considered to be useful for the differentiation between ON and SIF. It is important to recognize that SIF of the femoral head can develop in postoperative TKA patients.
LIST OF ABBREVIATIONS
| TKA | = Total Knee Arthroplasty |
| THA | = Total Hip Arthroplasty |
| MRI | = Magnetic Resonance Imaging |
| SIF | = Subchondral Insufficiency Fracture |
| ROM | = Range of Motion |
| FTA | = Femur - Tibia Angle |
| ON | = Osteonecrosis |
| OA | = Osteoarthritis |
ETHICS APPROVAL AND CONTENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
We have obtained consent to publish from the patient.
GUIDLINE REPORTING
CARE guidline have been followed.
FUNDING
None.
CONFLICT OF INTERST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEGEMENTS
Declared none.

