All published articles of this journal are available on ScienceDirect.

Successful Treatment of Total Hip Arthroplasty to a Patient Associated with Alcoholic Cirrhosis and Severe Plated Deficiency with Preoperative Partial Splenic Embolization
Abstract
Introduction:
We present the first report of the successful treatment of Total Hip Arthroplasty (THA) to a patient associated with alcoholic cirrhosis and plated deficiency undergoing preoperative Partial Splenic Embolization.
Case Report:
A 45-year woman who had Liver Cirrhosis (LC) and alcohol residue heritage failure suffered from severe groin pain and had a difficulty in walking for a long period due to avascular necrosis of bilateral femoral head. She was referred to our orthopaedic service and THA was planned. Despite preoperative transfusion for her platelet deficiency coursed by LC, preoperative platelet count decreased less than a normal range. Therefore, Partial Splenic Embolization (PSE) was applied to her so as to increase platelet count. PSE could temporally reduce the portal vein pressure and prevent a hyperspleism and cytopenia. After the procedure, THA was performed to bilateral hip safely through a direct anterior approach. At the time of the latest follow-up, the patient had an excellent clinical result.
Conclusion:
Preoperative PSE may be a useful procedure to the patients with LC and severe plated deficiency who need arthroplasty including THA. Pre-existing physical and psychological factors have an effect on the outcome of arthroplasty and appropriate strategies might be needed.
1. INTRODUCTION
We present the case of a patient who had Liver Cirrhosis (LC) after alcoholic hepatopathy and had a difficulty in walking for a long period due to avascular necrosis of bilateral femoral head. Total Hip Arthroplasty (THA) was planned for relieving her severe groin pain. Despite of preoperative transfusion for her platelet deficiency, preoperative platelet count decreased less than a normal range. Having a discussion with Gastroenterology department, Partial Splenic Embolization (PSE) applied to her so as to increase platelet count. PSE could temporally reduce the portal vein pressure and prevent a hypersplenism and cytopenia, secondary coursed by LC [1]. After the procedure, THA was performed to bilateral hip safely through a direct anterior approach. At the time of the latest follow-up, the patient had an excellent clinical result. To our knowledge, this report is the first to describe the successful treatment of Total Hip Arthroplasty to a psychiatric disorder patient associated with alcoholic cirrhosis and plated deficiency undergoing preoperative Partial Splenic Embolization.
2. CASE REPORT
The patient and her family was informed that data concerning this case would be submitted for presentation.
In October 2015, a 45-year woman was referred to our orthopaedic department for severe bilateral groin pain. She had been admitted to a psychiatric hospital for alcohol residue heritage failure and LC after alcoholic hepatopathy and had a difficulty in walking for a long period due to avascular necrosis of bilateral femoral head. Her alcohol dependency had been approximately treated, otherwise her physical condition forced her to stay in the hospital. Physical examination revealed a slim figure woman who was 160 cm tall and weighed 38 kg. She used a wheelchair and was not able to walk by herself because of groin pain. Radiographs and a Computed Tomography (CT) scan revealed collapse of femoral heads and arthritis of bilateral hip (Fig. 1). The Harris hip score was 38 points. Her platelet count was 16,000/μl and other laboratory data are shown in Table 1. She was made a consultation to Gastroenterology service for preoperative treatment. Her LC was diagnosed as Child’s class A, so it was decided to plan THA after transfusion of platelet and fresh frozen plasma. In November 2015, total 15 units of platelets were transfused the day before the surgery, additional 15 units of platelet and 3 units of fresh frozen plasma were transfused immediately before the surgery. Even though the preoperative transfusion, blood examination showed that her platelet count was 27,000/μl, lesser than a normal range. The operation was cancelled because of higher risk of blood loss.

| Normal range | Present case | |
|---|---|---|
| WBC (10³/μl) | 4.5-9.0 | 1.5 |
| RBC (106/μl) | 3.8-5.2 | 3.6 |
| Hb (g/dl) | 11.5-15.0 | 10.9 |
| Plt (10³/μl) | 140-340 | 16 |
| Bil-T (mg/dl) | 0.8> | 0.9 |
| γ-GT (U/l) | 7-77 | 318 |
| AST (U/l) | 5-40 | 66 |
| ALT (U/l) | 0-46 | 59 |
| LDH (U/l) | 119-229 | 168 |
| ALB (g/dl) | 4-5.1 | 3.5 |
| TP (g/dl) | 6.5-8 | 6.1 |
| UN (mg/dl) | 8-20 | 22.7 |
| Cr (mg/dl) | 0.47-0.79 | 0.85 |
| CRP (mg/dl) | 0.3> | 0.28 |
| PT (%) | 85< | 41 |
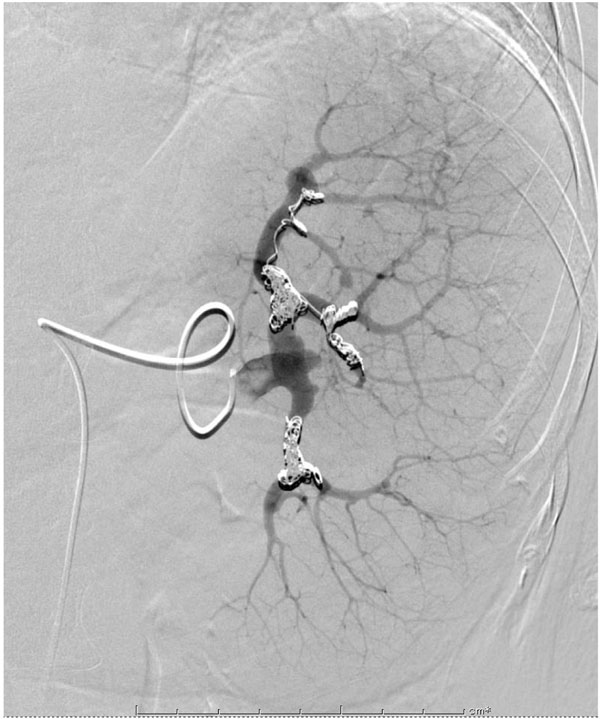
We discussed her physical condition again with Gastroenterology service and decided to apply Partial Splenic Embolization (PSE) to her before THA. LC may course a hypersplenism which enhances the progress of phagocytosis and the destruction of blood cells. And the enlarged spleen may retain a great quantity of blood cells inside which may result in a decrease in peripheral blood cell including platelet. PSE could temporally reduce the portal vein pressure and prevent a hypersplenism [1]. In February 2016, PSE was performed by an experienced radiologist after an informed consent to her and her family about a necessity of the procedure. Under a local anesthesia and sedation, stainless steel spring coils and 50%NBCA-lipiodol were placed in the main branch of the splenic artery. Approximately, 70% of the artery was successfully embolized (Fig. 2).
After the PSE, she had suffered an abdominal pain for a few weeks. Non-steroidal anti-inflammatory agent was administered to her for relieving a pain. Two months later, after the procedure, her platelet count increased to 174,000/μl. In April 2016, her right hip could be treated operatively, THA was performed through a direct anterior approach in order to reduce muscle damage and a risk of dislocation of the hip. After retracting the tensor fasciae lata and sartorius, the anterior hip capsule was exposed and removed. To expose the proximal femur and access to the femur canal, the femur was elevated by releasing the superior capsule. Cementless hip prosthesis was implanted to both acetabular side and femoral side (Trident cup and Accolade TMZF stem, Stryker Inc.). The operating time was 75 minutes, and the blood loss was 400 ml. In June 2016, THA to the left hip was performed. The operating time was 81 minutes, and the blood loss was 170 ml (Fig. 3). Four units of red blood cells and two units of fresh frozen plasma were transfused after each of the operations, no more platelets transfusion were needed. First generation cephalosporin was intravenously admitted immediately before the surgeries and then every eight hour for the first 48 hour postoperatively. The patient was allowed to walk with full weight-bearing.

Two years after the operations, the patient had an excellent clinical result. She was able to walk without crutches. She had discharged the psychiatric hospital and lived by herself without any groin pain and postoperative complications. The latest Harris hip score was 93 points.
3. DISCUSSION
Cirrhosis of the liver, irreversible fibrosis of liver tissue leading to hepatic dysfunction is a well-known risk factor for complication in patient who needs surgery. Patients with cirrhosis have a high risk of infection and excessive bleeding because this may be impaired phagocyte function. Hsieh et.al reported the high rate of early complications and the limited longevity of the prosthesis. They mentioned a 5-year survival rate in patient with cirrhosis after THA was 77.8% [2]. Tiberi et al described within 90 days of the procedure, patient with cirrhosis had greater number of hip dislocation, infection and revision surgeries and appropriate patient counseling is advised if THA is needed [3].
Splenic embolization was first introduced in 1973 to produce splenic artery embolization for hypersplenism treatment [4]. And then, transcatheter partial splenic embolization (PSE) was developed. Following the improvement of techniques [5], the indications have been extended to alteration of blood cell count, cirrhosis with portal hypertension and hypersplenism, Idiopathic thrombocytopenic purpura (ITP), splenic trauma, and so on [6-8]. Hypersplenism enhances the progress of phagocytosis and the destruction of blood cells. And the enlarged spleen may retain a great quantity of blood cells inside the hyperplastic splenic sinusoids, which evoke a decrease in peripheral blood cell including platelet. PSE could temporally reduce the portal vein pressure and prevent a hypersplenism [9]. PSE may resolve cytopenia, increase red blood cell, white blood cell and platelet count. Postembolization Syndrome is common complication after PSE. It includes intermitting fever, abdominal pain, nausea and vomiting but usually resolving without sequelae. It is caused by the acute edema in the infarct area and may be alleviated in a several days after effective pain control. In this report, the patient had suffered abdominal pain but generally resolving without sequelae [10]. The limitation of PSE exists mainly in the difficulties in the arteries to embolize and in evaluating volume [11]. An experienced radiologist may successfully perform PSE.
Netterville et al reported that Total knee replacement was performed for a patient with severe thrombocytopenia due to LC [12]. However, the other serious problem of this present case was that she had an alcohol residue heritage failure. Recent studies suggest that patient with psychiatric disorders tend to be worse than patients without them when undergoing THA [13]. Reports on increased length of stay, non-routine discharge, perioperative morbidity, periprosthetic infection rate, risk of falling and perioperative bleeding are all causes for concern. Furthermore, psychiatric patient may have a potential risk of postoperative artificial joint dislocation [14]. Gylvin et al. described that pre-existing psychological factors have an effect on the outcome of arthroplasty and appropriate strategies might be needed [15]. Tsukada et al. reported the lower dislocation rate following THA via Direct Anterior Approach (DAA) than via posterior approach (PA). In their study, the dislocation was significantly less in the DAA group as compared to the PA group. They described that DAA does not detach muscle or tendon during the operation, thereby maintaining soft tissue tension which is one of the factors of postoperative dislocation [16]. In this case, we performed THA through a direct anterior approach in order to reduce muscle damage and a risk of artificial joint dislocation [17, 18]. At the time of the latest follow-up, the patient had no postoperative complication.
CONCLUSION
To our knowledge, this report first described the successful treatment of THA to a psychiatric disorder patient associated with severe alcoholic cirrhosis and plated deficiency undergoing preoperative Partial Splenic Embolization. Further observation will be needed for perioperative complications.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this article.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all participants.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors thank the department of Gastroenterology and Radiology, Sapporo City General Hospital.

